I’ve updated my model for recent news, and after a series of assumption changes that mostly net out, it still predicts a very small exit wave with ~4k additional deaths (reduced from 9k previously) – and with a small added dose of seasonality, no exit wave at all. 1/n 

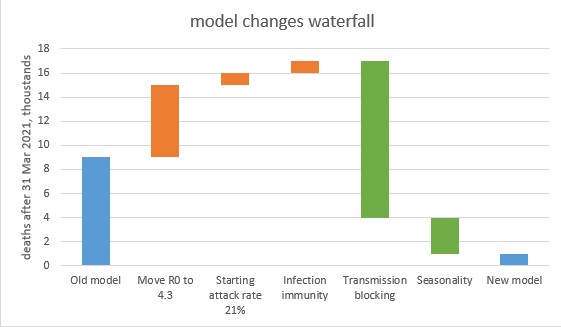
The key changes in the model are shown in the waterfall chart below, and explored in more detail in the thread that follows this summary. 2/n
This conclusion feels more solid than before, as no single-factor sensitivity (within plausible ranges of uncertainty) takes the exit-wave deaths over 10k- see 1st chart. To get significantly higher deaths I have to move multiple assumptions at the same time– see 2nd chart. 3/n


That’s the end of the summary – the remainder of this thread is for those interested in the details. First, a reminder of where we’re starting from: the old model predicted a small, slow-burning exit wave through this autumn with ~9k deaths. 4/n

My first change is to adjust R0 from 4.0 to 4.3. I don’t have much science for this, but my sense from comparing to other models is that I’m on the low end of the consensus. This change increases deaths in the exit wave to ~15k. 5/n

The second change is to nudge the starting attack rate (in Jan ’21) down to 21%, from 23%. Regular readers will note that I’m partly undoing a previous shift from 18% to 23%. I believe the 21% is consistent with ONS, MRC and other data; this takes deaths up to ~16k. 6/n
The third change is to switch from assuming that infection causes 100% sterilising immunity to 83% (consistent with SIREN data), with a further 9% getting partial immunity. This caused a *lot* of modelling work, but the impact is only another ~1k deaths (to ~17k) 7/n

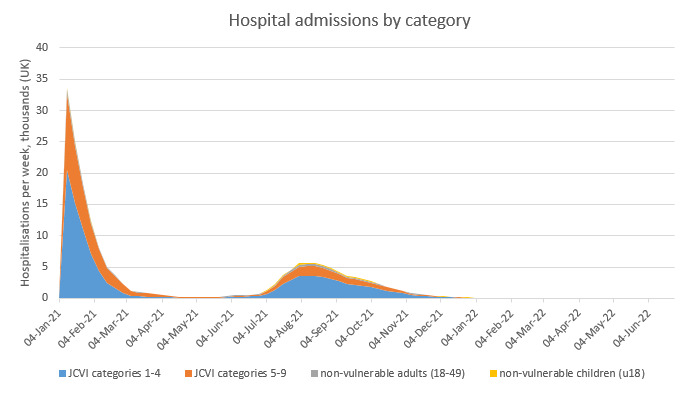
The most significant change is to introduce an assumption that the lower viral loads in post-vaccination infections (and similarly reinfections) cause a 30% reduction in onward transmission. This reduces the size of the exit wave significantly, with deaths down to ~4k. 8/n

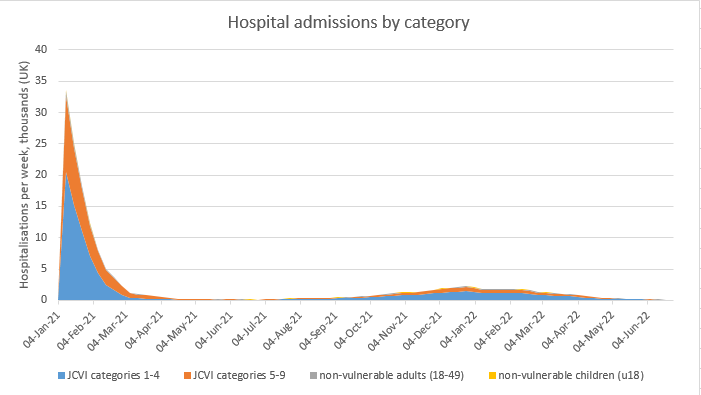
Finally, I am re-introducing an assumption of mild seasonality, with R0 reducing by c. 18% in mid-summer compared to mid-winter. This is enough to squash the exit wave, with just ~1k further deaths after the end of March (and most of those in April). 9/n

So, this is my new base case – with a very small or no exit wave. I’ve also updated the sensitivity analysis (using the no-seasonality case as a basis) – this shows that no single assumption change takes the exit-wave death toll over 10k. 10/n

To get larger movements, I’ve put the assumptions into 3 groups: one linked to R0 and infection, one linked to vaccine supply and take-up, and linked to vaccine efficacy. Only the last group has a large impact: over 30k deaths if all my VE assumptions are too optimistic. 11/n

Hence my conclusion is that while a large exit wave is still possible, it is looking increasingly unlikely, provided that we stick to the roadmap (roughly) as advertised, vaccine supply and take-up continues to be healthy, and that real-life vaccine efficacy turns out OK. 12/n
To finish, some brief comments on things the model doesn’t handle (the list is getting shorter as I gradually knock them off one by one, but there’s still a few there): 13/n
1) Firstly, heterogeneity of contacts &/or susceptibility could reduce the herd immunity threshold (HIT), but with people being vaccinated at random (and favouring older, less sociable groups) in my view this is unlikely to make a big difference in the UK this summer 14/n
2) On the other hand, spatial heterogeneity could make a difference – i.e. some local areas with lower vaccine uptake and attack rate &/or higher natural R0 could be further away from HIT and therefore susceptible to local outbreaks, even if UK as a whole is over its HIT. 15/n
3) The model makes no attempt to model ‘waning’ of immunity over time, or the potential impact of new variants that could fully or partially ‘escape’ the immunity that has built up so far. I hope to let you have some modelling of potential variant impacts after Easter. 16/n
And just to conclude with thanks to those who have helped me with advice on input-setting, assumptions and model design – you know who you are, and I won’t @ you here to avoid embarrassment and hate mail, but it’s much appreciated. Happy Easter everyone! /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh