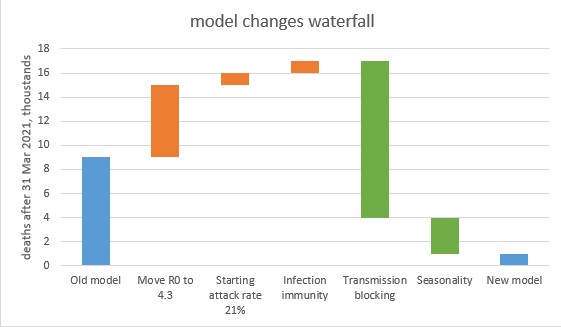
After yesterday’s model update (
https://twitter.com/JamesWard73/status/1377640517379497987?s=20) a few people have asked: so if there’s no exit wave, or just a small one, does that mean we could open up earlier? And the answer is: maybe, but it’s complicated. If you’re interested in the details, read on… 1/n
All of yesterday’s modelling assumed that we follow the government’s roadmap to 21st June, when we remove all remaining restrictions and controls, and behaviour returns to normal. (note that point: all controls removed on 21st June, it will become important later on). 2/n
But what happens if we vary this date? I’ve adjusted this in the model, bringing it back 1 week at a time up to 5th April, and also extending it the other way to 26th July, for completeness. As you can see (from blue line below), opening on 21st June looks OK, and you could 3/n 

…probably bring it forward a couple of weeks (e.g. to 7th June) without much risk, but as you come back into May, the additional deaths start to ramp up, and any final unlocking before mid-May looks very dangerous (with ~40k deaths in the exit wave). 4/n
The green line on the chart shows what happens if I turn on the “mild seasonality” switch in my model. Here, things look a lot easier, and unlocking in mid-May is probably fine. (but April is still a bad idea if you don’t want 20-50k deaths in the exit wave). 5/n

But what if my model, or the assumptions in it, is wrong? I’ve tried to explore this by adding three more scenarios, which correspond to the assumption groups in yesterday’s sensitivity analysis. So the yellow, orange and red lines below correspond to worse assumptions for… 6/n

… vaccine supply & take-up, R0 and infection rates, and vaccine efficacy respectively. Inevitably, the outcomes are worse, and if you thought you were on one of those lines, you probably wouldn’t want to unlock much earlier than planned (and could argue for a bit later). 7/n
So what to do? Well, as we get closer in we should be able to narrow the range of uncertainty, and hopefully can then dismiss the yellow/orange/red lines as unlikely. With that knowledge, there could be a good argument for bringing forward the unlocking e.g. to 7th June. 8/n
Going further than that would be a bet on seasonality, which the government may well be reluctant to take, as it will be difficult to get data on this ahead of time. (ideally we’d have a well-defined “hot week” of summery weather in April, which would help the analysis!). 9/n
But I think there is a way we can accelerate the timetable while limiting the risks. And that would be to exit earlier (e.g. in mid-May), but into a near-normal state with baseline controls (such as TTI and masks in crowded indoor spaces) maintained up to the end of July. 10/n
We’re not sure what effect those baseline controls will have on R, I’ve seen estimates ranging from 10-30% reduction in transmission. So here are two scenarios, one set at 10% reduction (dashed line) and one at 25% reduction (dotted line), assuming no seasonality. 11/n

As you can see, this brings the risk level down much closer to the model with seasonality (green), and means the govt might feel more comfortable opening up in mid-May. In a pessimistic scenario, that could cause another 10-12k deaths – but more likely it would be 3-5k. 12/n
Is that “worth it”? I don’t know, it’s hard even talking and writing about this, and these are real people’s lives, not pixels on a chart. But the reality, whether we like it or not, is that we face a trade-off between the speed of opening up and covid deaths on the way out. 13/n
Your view on the optimal trade-off will depend on how bad you think the ongoing controls are – and note between mid-May and mid-June we’re not talking about lockdown, this is more like Tier 1 with pubs & restaurants open + rule of 6 indoors (but nightclubs closed). 14/n
Would you impose those controls for a month to save one life? ten? a hundred? a thousand? ten thousand? a hundred thousand? I’m glad I don’t have to make those decisions, but hopefully the analysis supports a debate on where, as a society, we should draw the line. /end
• • •
Missing some Tweet in this thread? You can try to
force a refresh