I am interested (as an anaesthetist/intensivist) in the claims that N95/FFP masks could
-raise CO2
-decreased oxygen uptake in pregnant patients
It is not a trivial claim
aricjournal.biomedcentral.com/articles/10.11…
& is stated here by a WHO IPC expert group
..among a long list of downsides
1/15
-raise CO2
-decreased oxygen uptake in pregnant patients
It is not a trivial claim
aricjournal.biomedcentral.com/articles/10.11…
& is stated here by a WHO IPC expert group
..among a long list of downsides
1/15
The paper quoted regarding CO2 elevation is this one
ajicjournal.org/article/S0196-…
It studied
10 nurses
All white
9 female
9 elevated BMI, 5 BMI >30 kg/m2
2x 12 hour shifts
N95 +/- surgical mask over it
Unclear whether expiratory valve
Assessed
compliance comfort & physiology
2/15
ajicjournal.org/article/S0196-…
It studied
10 nurses
All white
9 female
9 elevated BMI, 5 BMI >30 kg/m2
2x 12 hour shifts
N95 +/- surgical mask over it
Unclear whether expiratory valve
Assessed
compliance comfort & physiology
2/15
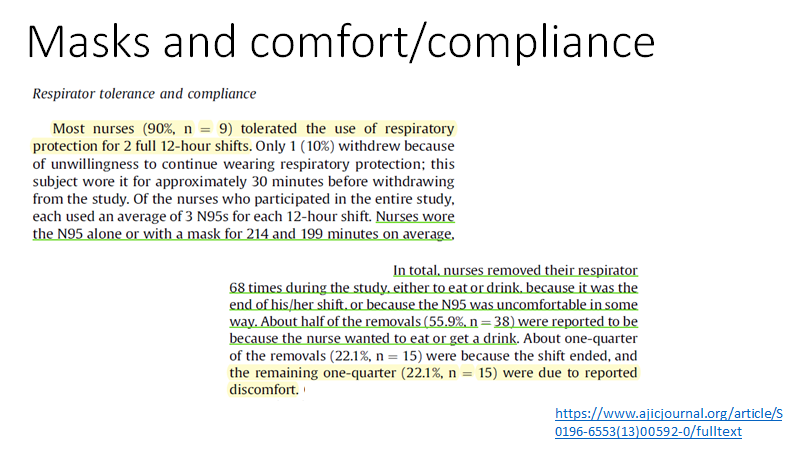
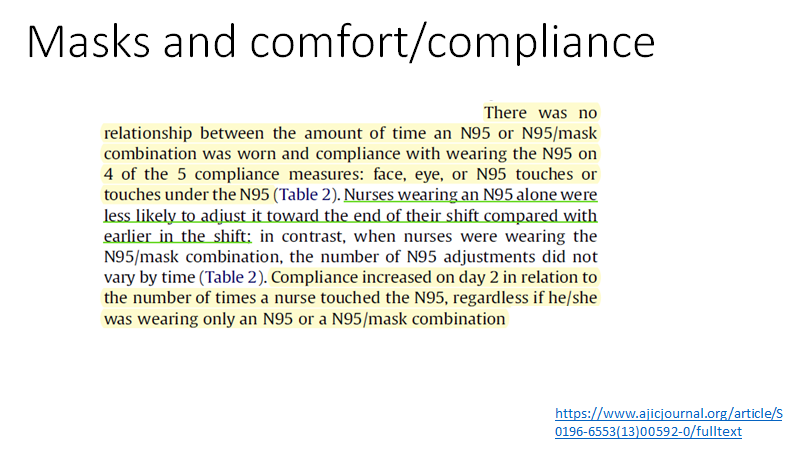
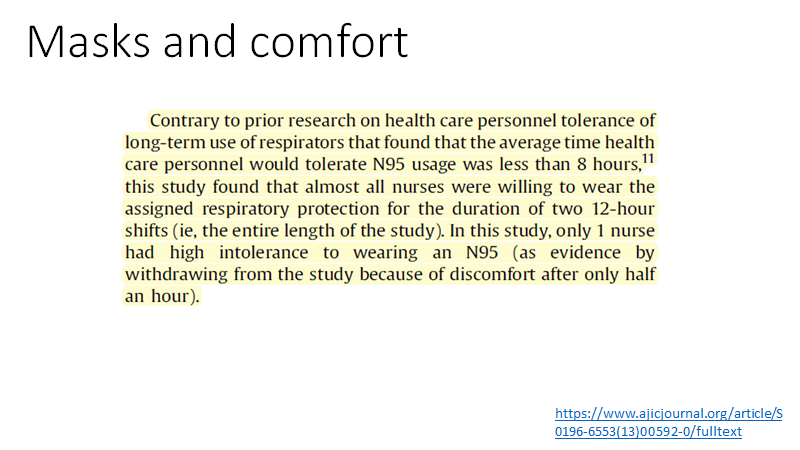
The compliance and comfort evaluations showed
-lots of minor discomfort
-but rather well tolerated
-most removals at shift end or to drink
-compliance on day 2 better than day 1
3/15
-lots of minor discomfort
-but rather well tolerated
-most removals at shift end or to drink
-compliance on day 2 better than day 1
3/15
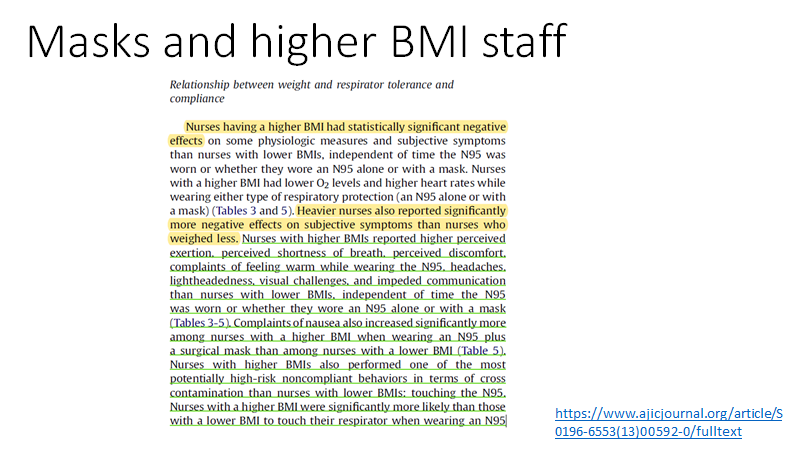
Of note, many of the staff had elevated BMIs
Poor compliance and discomfort was much more common in those with the higher BMI
The authors note of the US population
- 1 in 3 overweight
- 1 in 3 obese
4/15
Poor compliance and discomfort was much more common in those with the higher BMI
The authors note of the US population
- 1 in 3 overweight
- 1 in 3 obese
4/15
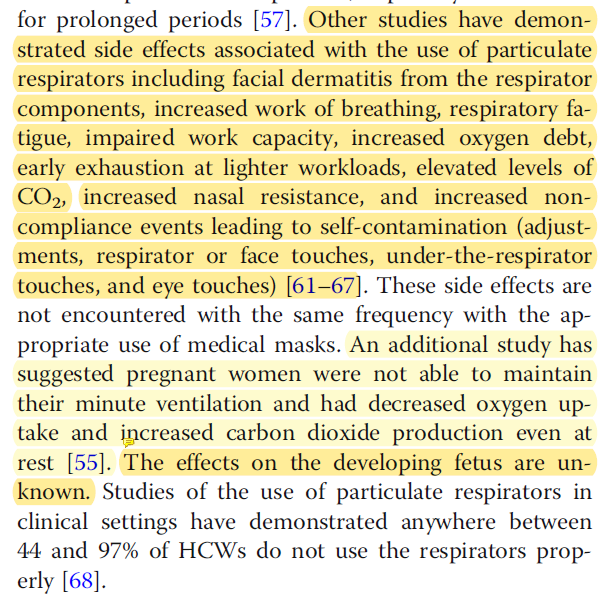
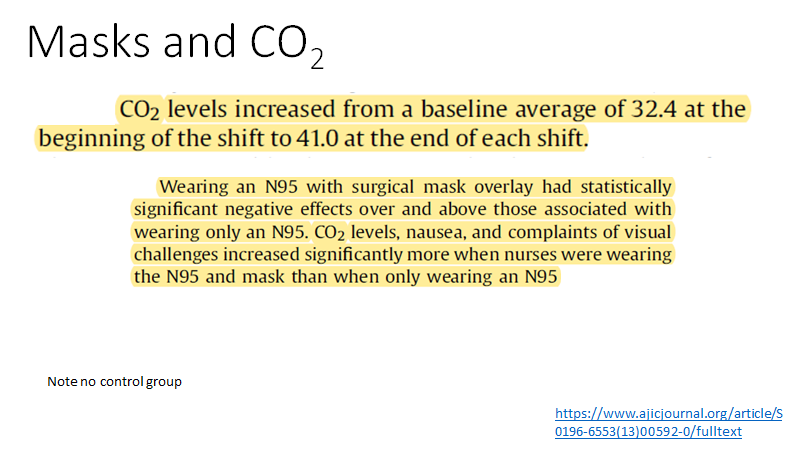
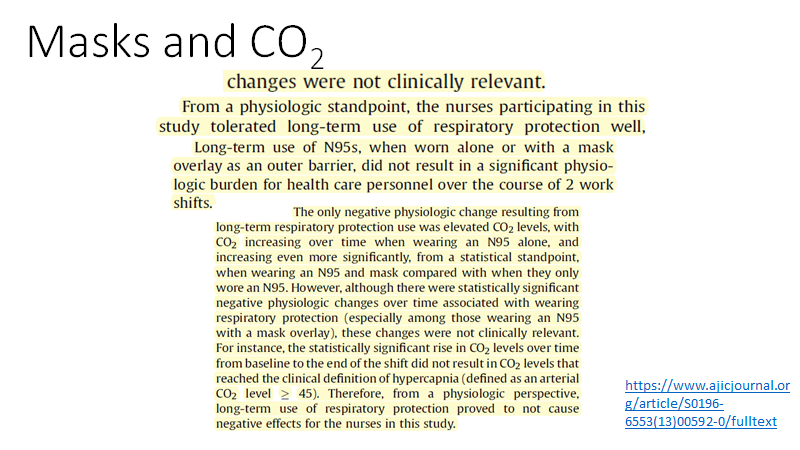
As for N95 and CO2
-this was measured through the skin
-rose from 32 mmHg (4.3kPa) to 41 (5.5) at end of shift
-rise was more marked if a face mask was worn over the N95
-there were no physiological disturbances associated with the rise
5/15
-this was measured through the skin
-rose from 32 mmHg (4.3kPa) to 41 (5.5) at end of shift
-rise was more marked if a face mask was worn over the N95
-there were no physiological disturbances associated with the rise
5/15
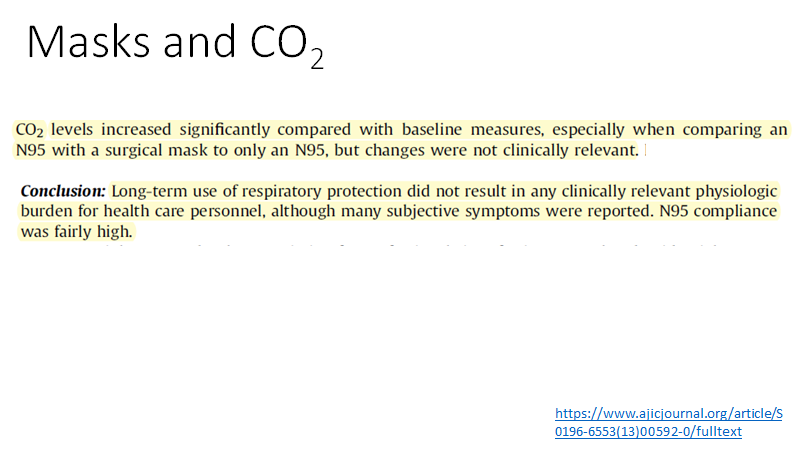
So does the CO2 rise with N95 mask matter?
-the authors clearly think it does not
(which makes it slightly odd for the review above to quote it)
But it does show that filtering masks are harder to breath through
6/15
-the authors clearly think it does not
(which makes it slightly odd for the review above to quote it)
But it does show that filtering masks are harder to breath through
6/15
Does a 6 mmHg (0.8kPa) CO2 rise have adverse physiological effects?
Much higher rises in a person with poor health might have plausibly have clinical impact
But generally a mildly elevated CO2 is not of itself harmful - more likely its the process causing it
So no!
7/15
Much higher rises in a person with poor health might have plausibly have clinical impact
But generally a mildly elevated CO2 is not of itself harmful - more likely its the process causing it
So no!
7/15
So, on to the next quoted paper.
aricjournal.biomedcentral.com/articles/10.11…
Suggesting use of N95 mask use is risky for the pregnant woman
The limitations of this paper are well covered from a 'physics' perspective in this thread
8/15
aricjournal.biomedcentral.com/articles/10.11…
Suggesting use of N95 mask use is risky for the pregnant woman
The limitations of this paper are well covered from a 'physics' perspective in this thread
https://twitter.com/caruzycki/status/1380711275307540481?s=20
8/15
My thoughts..
19 mid-pregnancy subjects did the main study
Av 30 weeks gestation, BMI 26.6 kg/m2
Exercised to simulate active nursing activity
Then did this level of exercise for 15 minutes on treadmill
With and without "N95 mask apparatus"
9/15
19 mid-pregnancy subjects did the main study
Av 30 weeks gestation, BMI 26.6 kg/m2
Exercised to simulate active nursing activity
Then did this level of exercise for 15 minutes on treadmill
With and without "N95 mask apparatus"
9/15

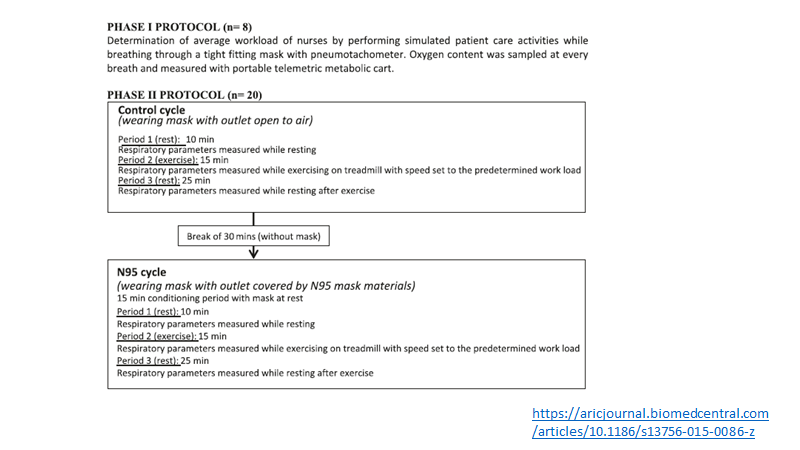
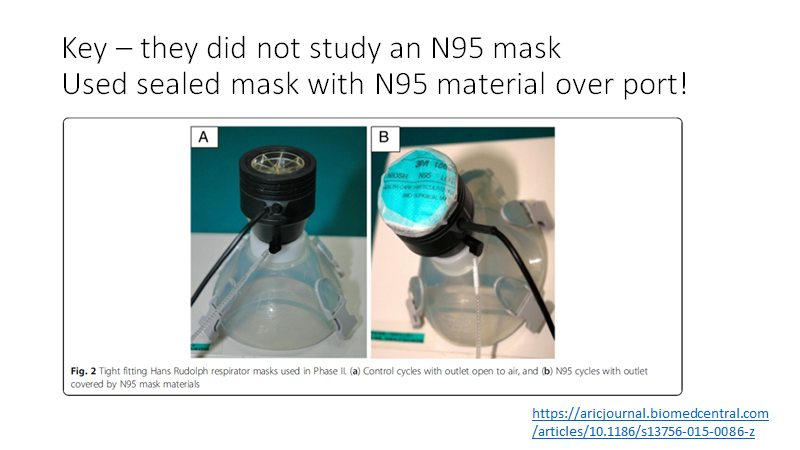
Important limitation is that the study was not of N95 use
Used a tight mask used with N95 material over port
This makes study protocol easier but real concerns whether this experimental set up is valid... (creates excessive respiratory resistance)
10/15
Used a tight mask used with N95 material over port
This makes study protocol easier but real concerns whether this experimental set up is valid... (creates excessive respiratory resistance)
10/15
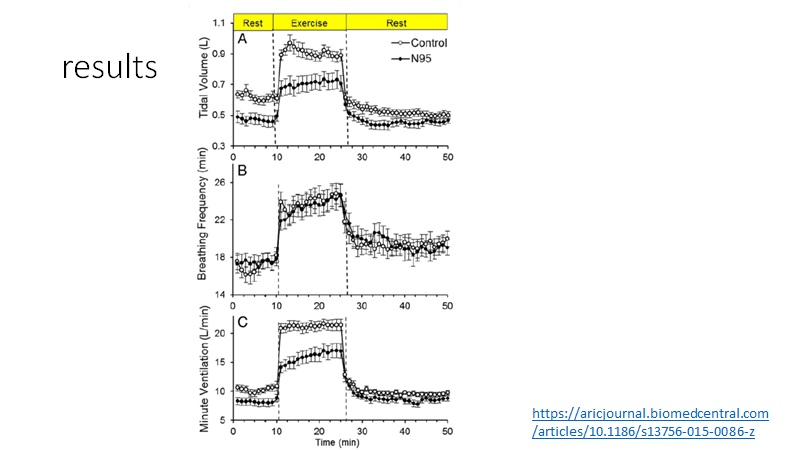
Results
The N95 apparatus
-reduced breathing depth but not rate
-reduced min volume on exercise
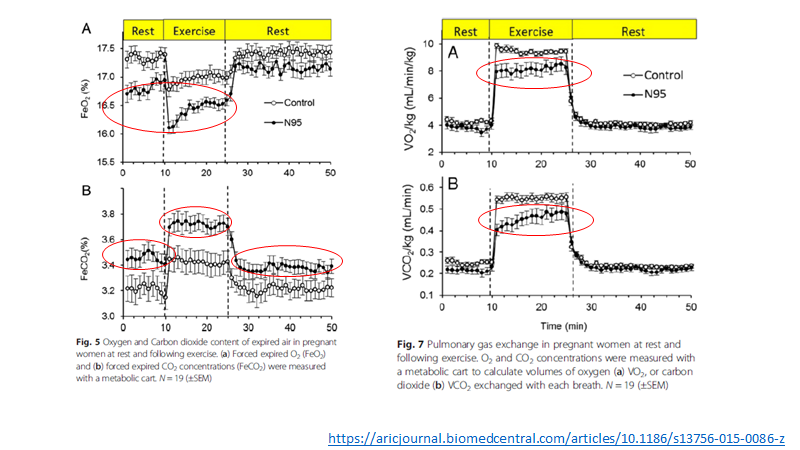
-reduced expired O2
-raised expired CO2
-reduced VO2 and VCO2 during exercise
did not change mothers SpO2, HR, lactate or baby HR or variability
11/15
The N95 apparatus
-reduced breathing depth but not rate
-reduced min volume on exercise
-reduced expired O2
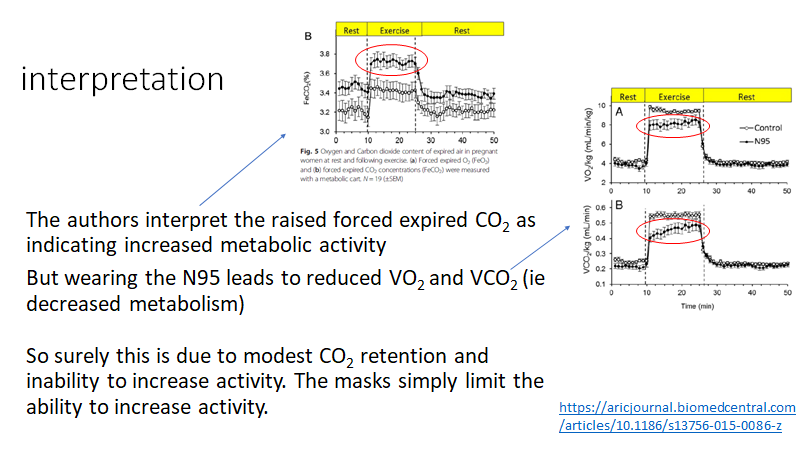
-raised expired CO2
-reduced VO2 and VCO2 during exercise
did not change mothers SpO2, HR, lactate or baby HR or variability
11/15
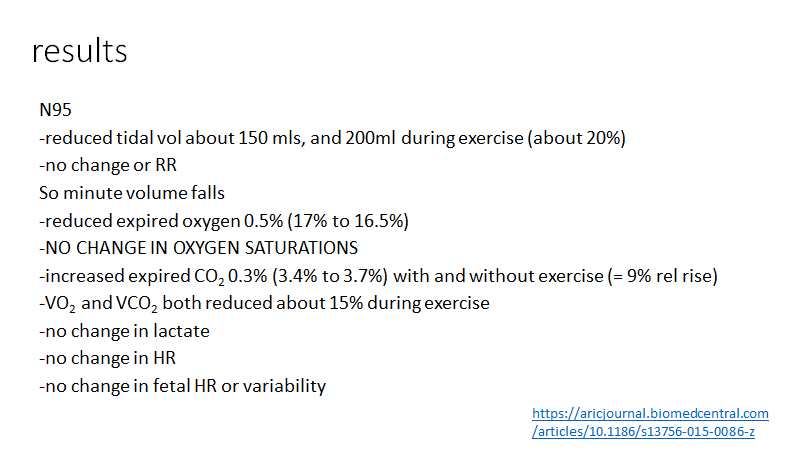
For me the KEY result in all this is that maternal oxygen (saturation) is maintained.
Therefore no alteration to oxygen delivered via placenta to fetus
The maternal CO2 is raised (as expected) but again the clinical impact of this is likely to be negligible or zero
12/15
Therefore no alteration to oxygen delivered via placenta to fetus
The maternal CO2 is raised (as expected) but again the clinical impact of this is likely to be negligible or zero
12/15
I differ in my interpretation of the results from the authors
13/15
13/15
Overall I'm reassured
-N95/FFP3 masks increase breathing resistance compared to no mask or surgical mask
-physiological response is to breathe harder (maintain CO2) or let CO2 rise a bit
-this CO2 rise is not harmful
-there is no impact on oxygenation
-including if pregant
15/15
-N95/FFP3 masks increase breathing resistance compared to no mask or surgical mask
-physiological response is to breathe harder (maintain CO2) or let CO2 rise a bit
-this CO2 rise is not harmful
-there is no impact on oxygenation
-including if pregant
15/15
• • •
Missing some Tweet in this thread? You can try to
force a refresh