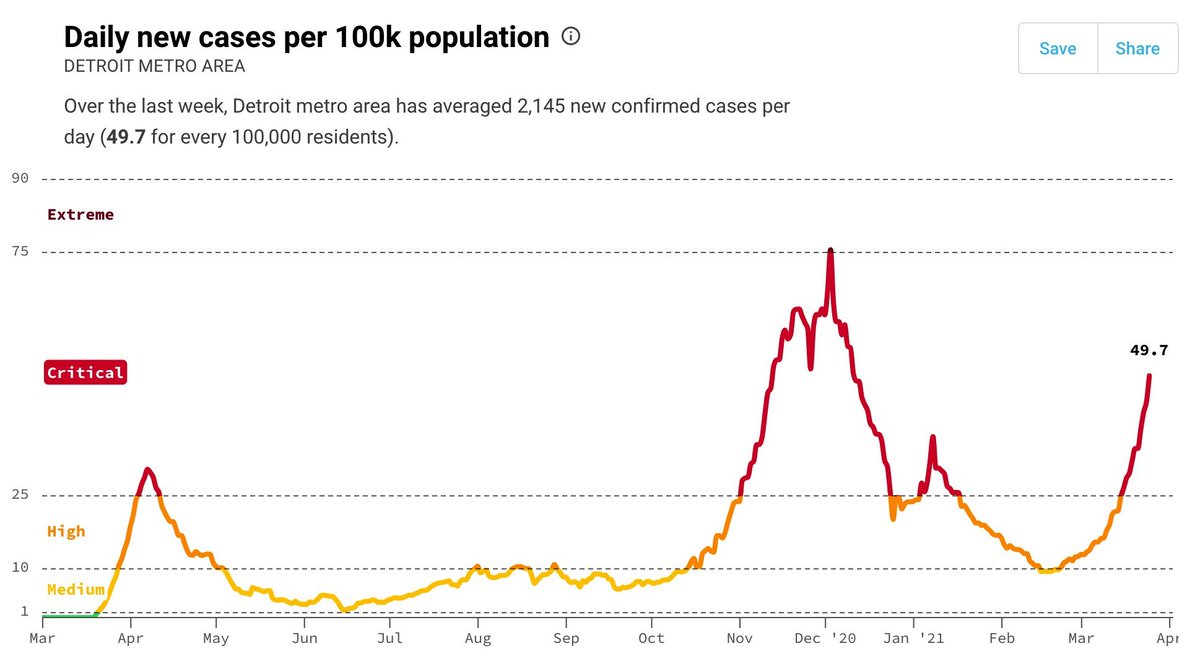
Vaccination can have rapid impacts on transmission & disease & surging vaccines to MI could save many lives.
Comments in NYT article from multiple health officials including @CDCDirector @celinegounder are surprisingly at odds w/ data. 1-2 wks not 6. nytimes.com/2021/04/12/us/…
Comments in NYT article from multiple health officials including @CDCDirector @celinegounder are surprisingly at odds w/ data. 1-2 wks not 6. nytimes.com/2021/04/12/us/…
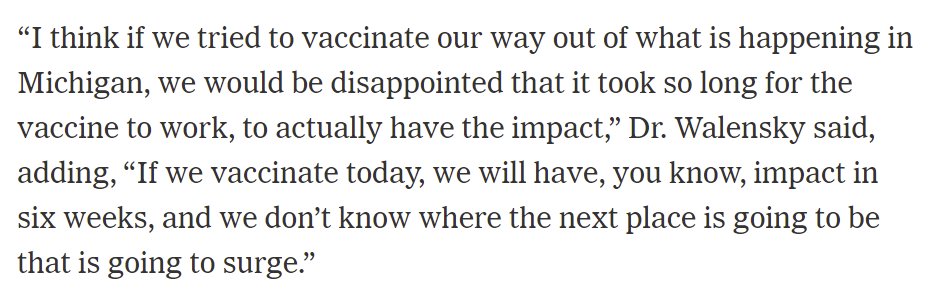
@CDCDirector argues increasing vaccine supply to MI would take 6 weeks to take effect.
Article by @noahweiland @MitchKSmith tries to explain this by stating that time for full protection w/ mRNA vaccines. But we know 1 dose offers substantial protection vs disease AND infection.
Article by @noahweiland @MitchKSmith tries to explain this by stating that time for full protection w/ mRNA vaccines. But we know 1 dose offers substantial protection vs disease AND infection.
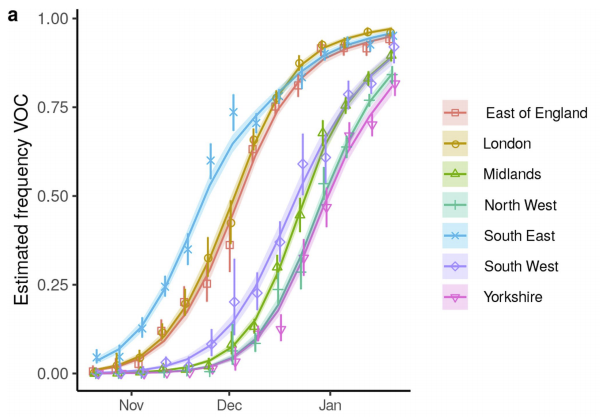
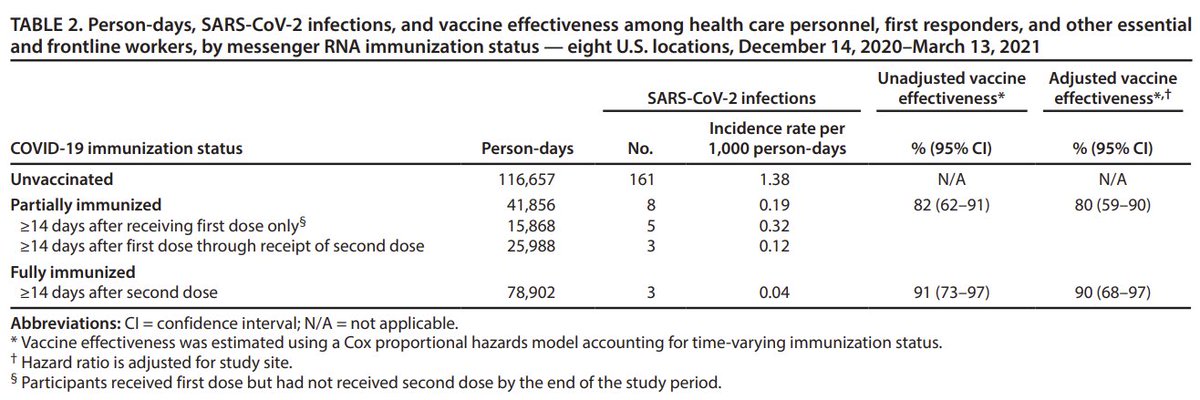
Paper published in CDC's own journal MMWR showed protection against INFECTION (not symptoms) is 80% 2 wks after 1st dose. Thus, vaccinating people could reduce transmission much more quickly than 6 wks.
cdc.gov/mmwr/volumes/7…
cdc.gov/mmwr/volumes/7…
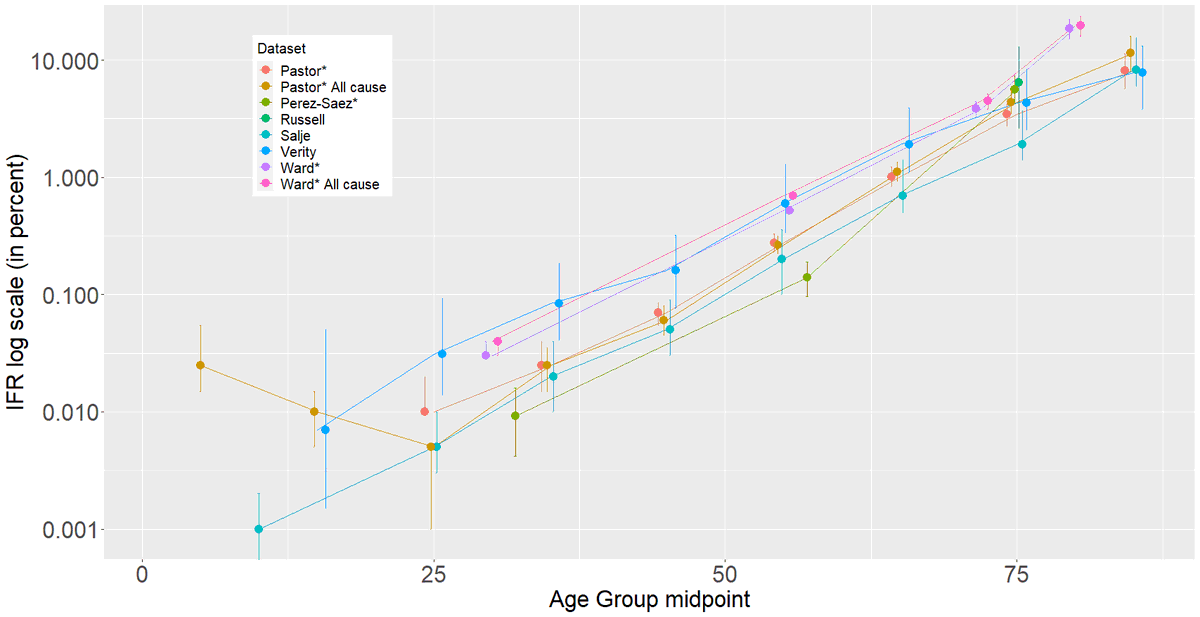
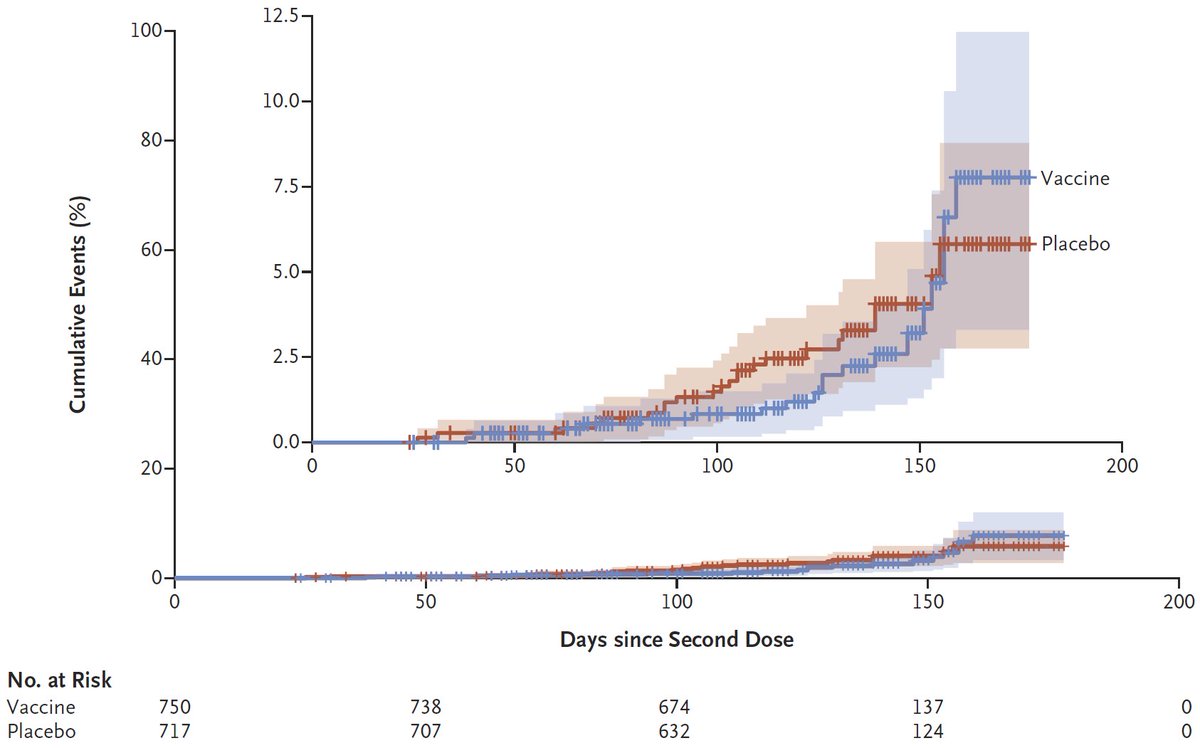
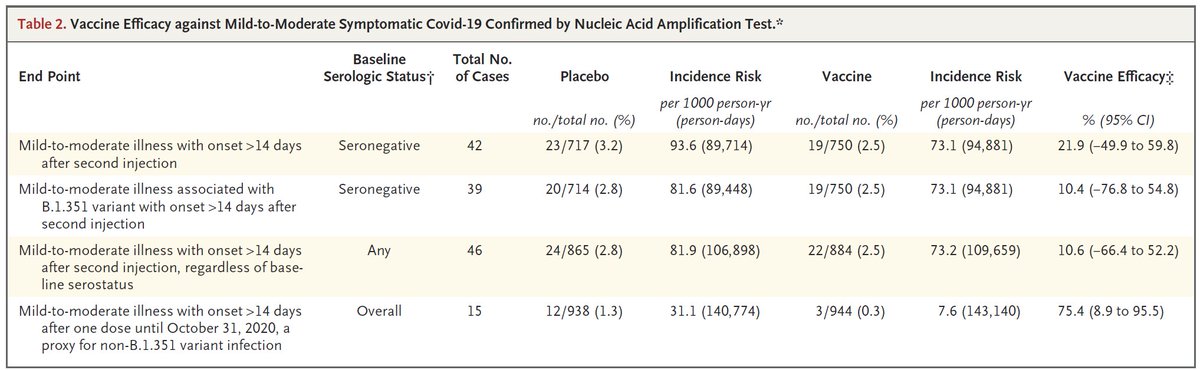
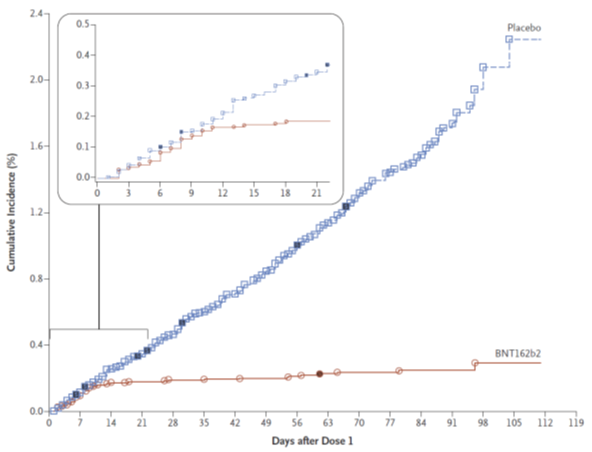
Similarly, direct protection against illness happens much more quickly. Data from trials show separation in symptomatic cases starts @ day 10-12 & since dates of symptom onset are shown (which occur 5-6 d after infection) protection is even earlier.
DOI: 10.1056/NEJMoa2034577
DOI: 10.1056/NEJMoa2034577
Thus, while its true that other interventions could be quicker (e.g. closing businesses) those are difficult to enact & state already has mask mandate. Sending vaccines to where they are needed most would save more lives.
In case anyone thinks I have a special fondness for MI, I don't. I think this strategy should be employed to any state where cases are surging. Targeted vaccination could save many more lives than simply allocating them on a per capita basis.
• • •
Missing some Tweet in this thread? You can try to
force a refresh