Differential growth trajectories of B.1.1.7 (UK variant) in US states.
The rate of increase in frequency of B.1.1.7 varies between different locations that also differ in case trajectories. What is driving this?
Thread
The rate of increase in frequency of B.1.1.7 varies between different locations that also differ in case trajectories. What is driving this?
Thread
We know have clear evidence of variant B.1.1.7 being more 50-100% infectious & ~67% more deadly. It is likely playing an important role in the current surge in cases in Europe.
nature.com/articles/s4158…
doi.org/10.2807/1560-7…
nature.com/articles/s4158…
doi.org/10.2807/1560-7…
B.1.1.7 has also been detected in many US states(helix.com/pages/helix-co…) & is probably present in most states now. In Jan-Feb most expected it to spread rapidly in US to become the dominant variant like it did in UK Nov-Jan, & other EU countries later (nature.com/articles/s4158…)
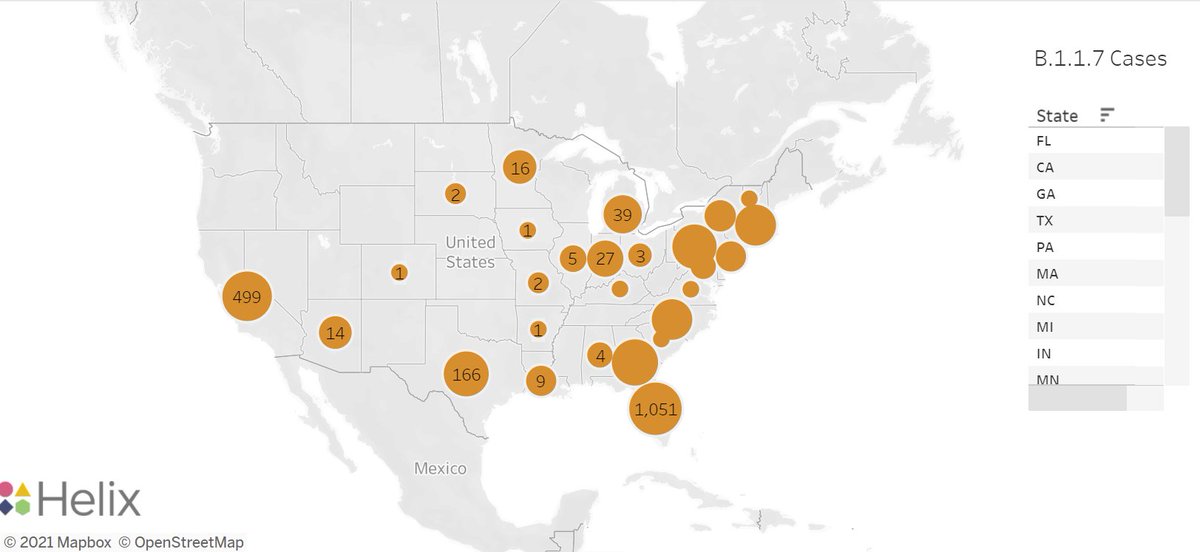
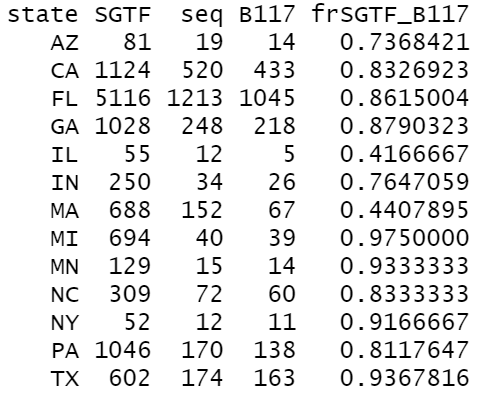
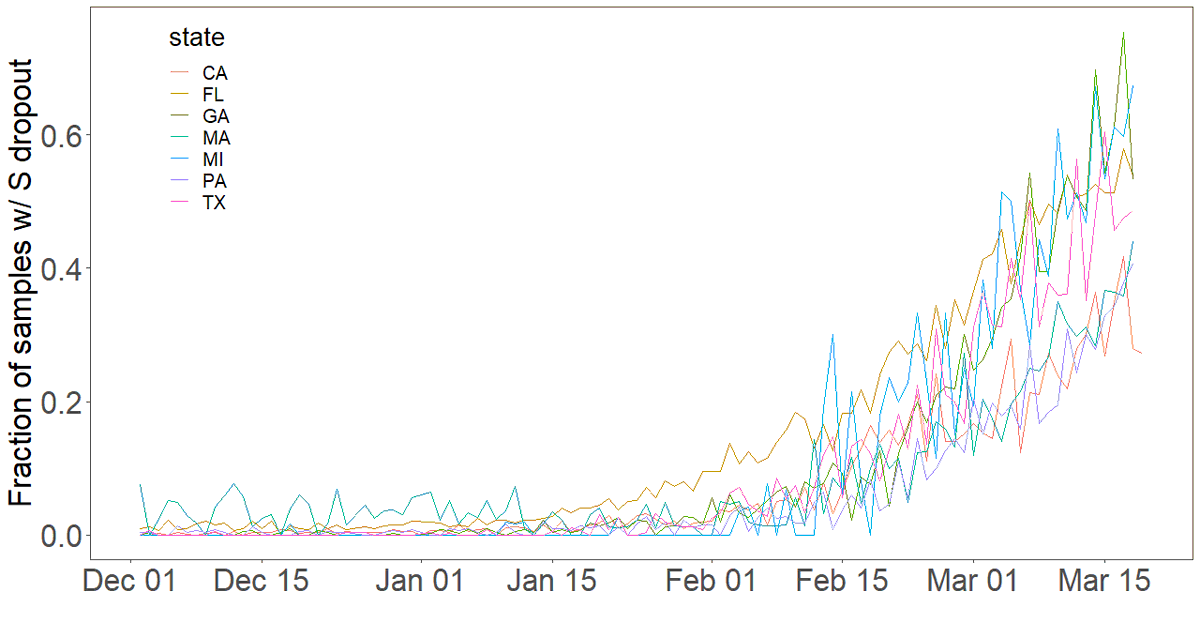
As expected, B.1.1.7 has increased in frequency in many states. 13 states w/ N>50 S-dropout mutation samples from helix.com/pages/helix-co… & in all but MA, most of these are B.1.1.7. But...
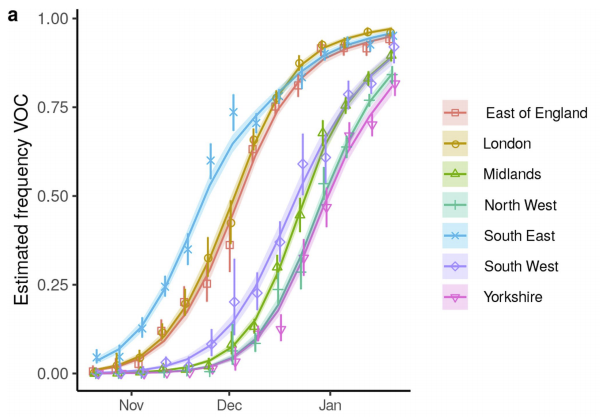
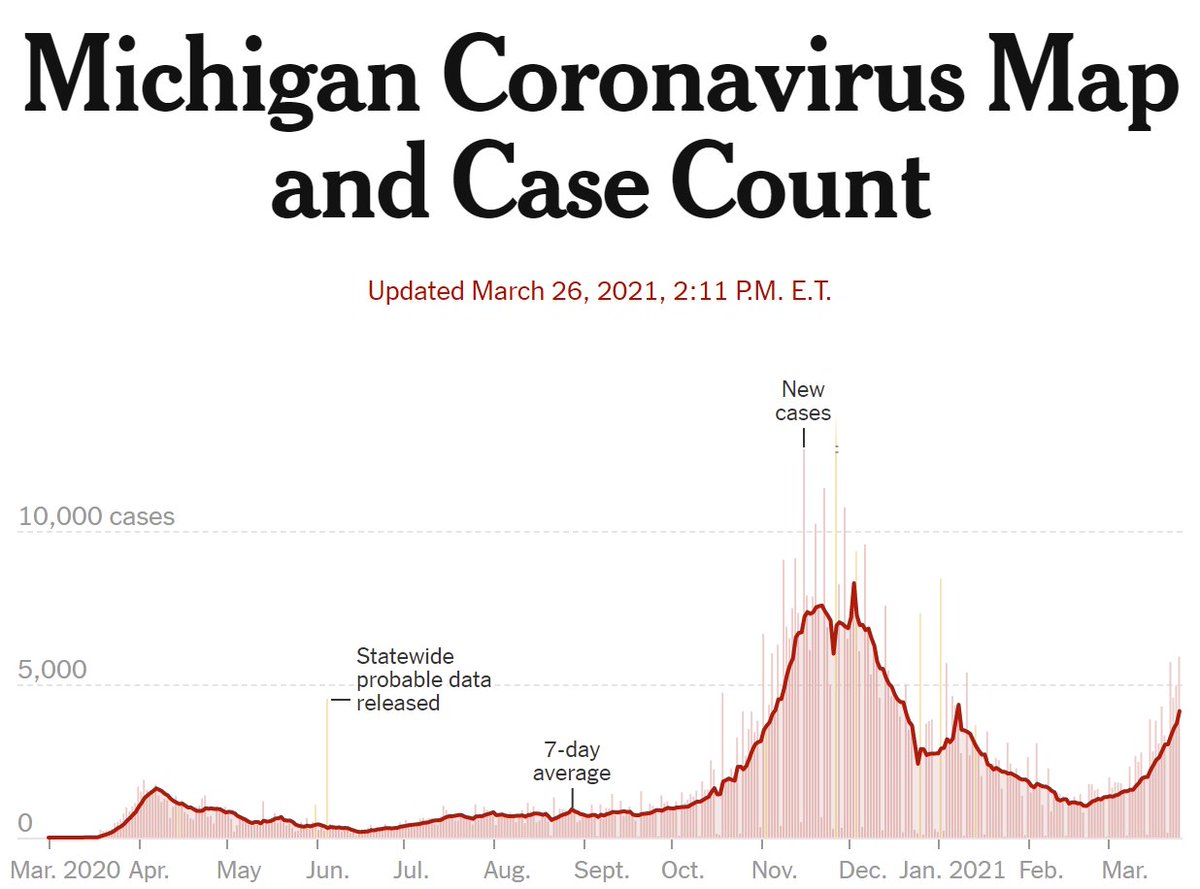
Rate of increase in frequency has differed among states. Plot of Helix data shows freq of S-dropout samples for 7 states with high freq. Some states rose early (FL), others later but caught up (GA, MI, TX). It's not just sampling variability...
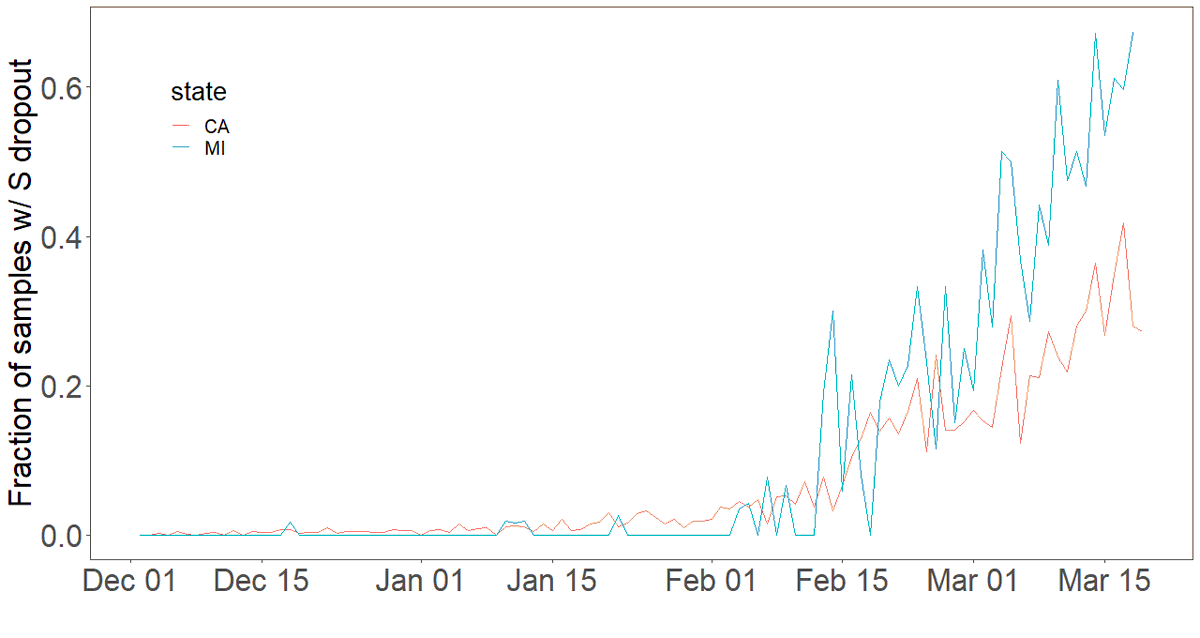
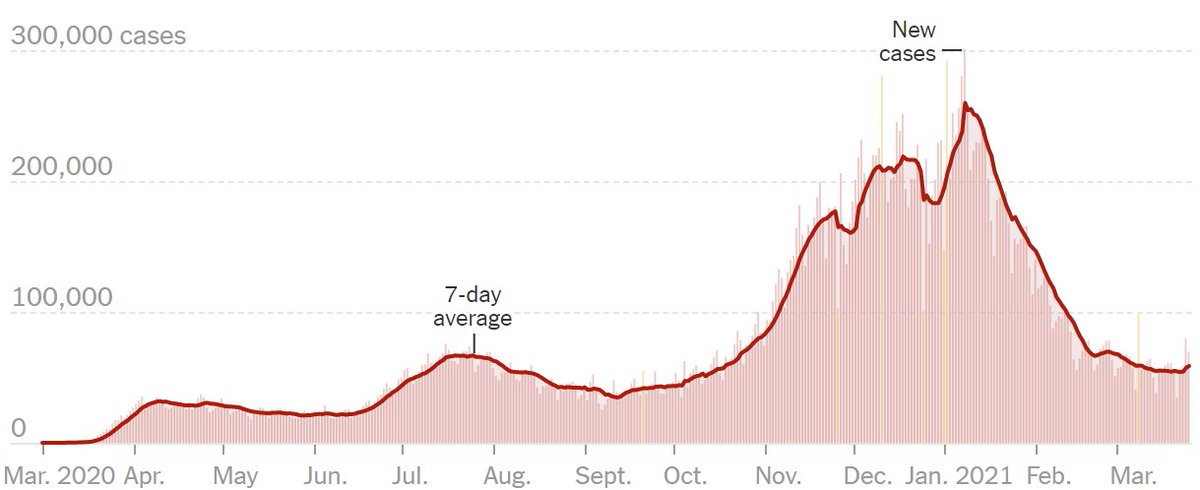
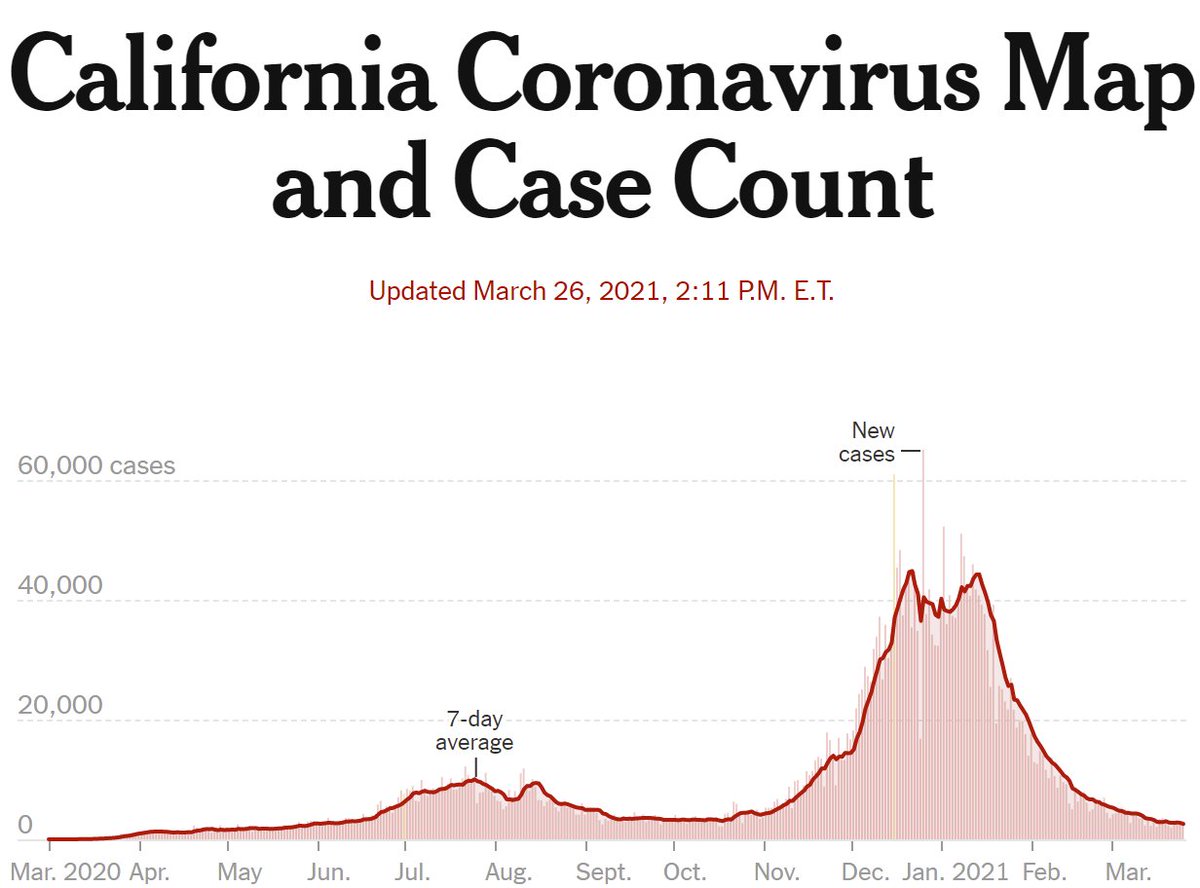
For illustration, we can compare 2 states, MI&CA. Frequencies similar in Feb (when 90%,97% of S dropout were B.1.1.7 in CA,MI), but in Mar MI clearly increases faster. Simple analysis (log reg) indicates rate of increase ~50% higher for MI, despite starting a tiny bit lower.

Possibly reasons for differential growth among "states":
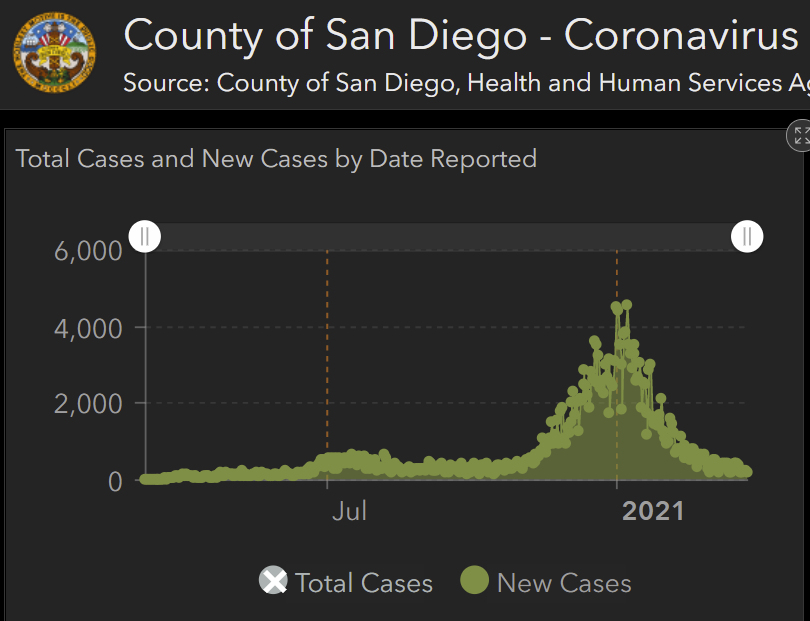
-Helix data aren't random sample of state's cases. In some states they come from small area (e.g. CA are mostly San Diego). Shift in locations of samples over time could skew rate of increase.
-Helix data aren't random sample of state's cases. In some states they come from small area (e.g. CA are mostly San Diego). Shift in locations of samples over time could skew rate of increase.
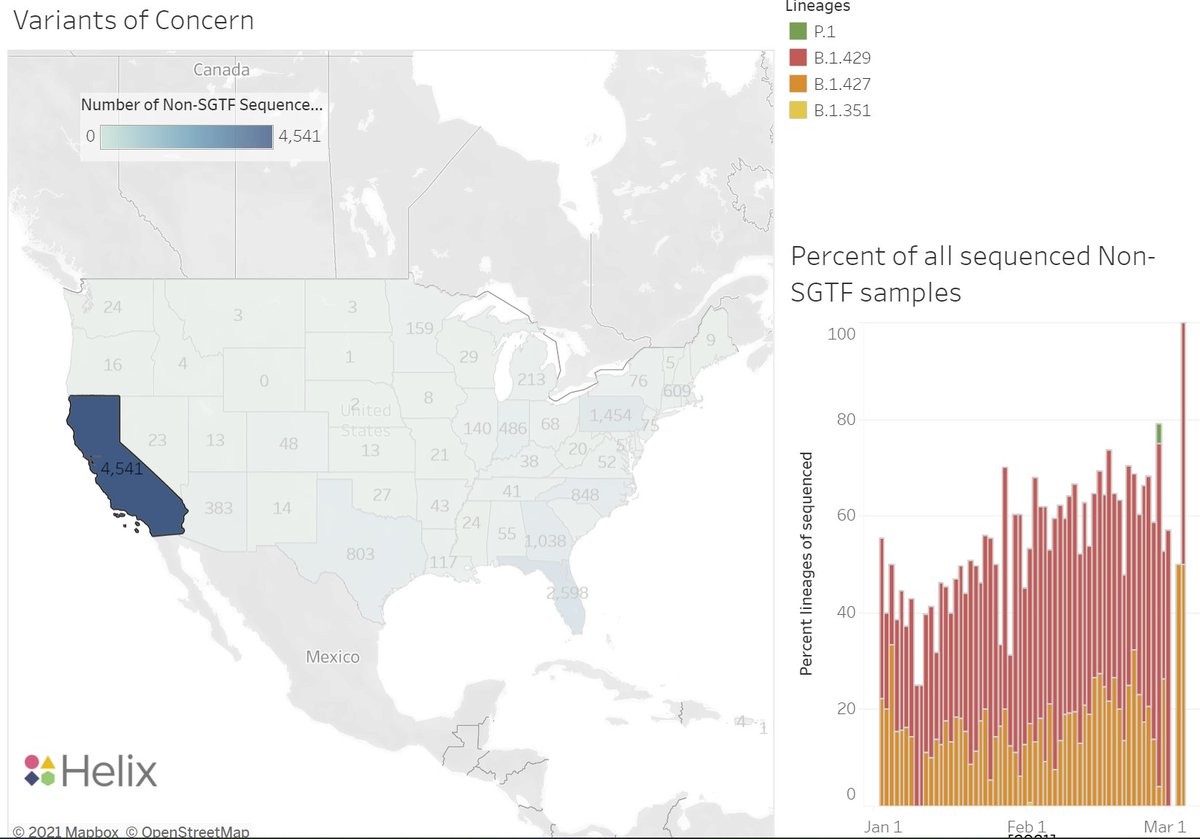
-Differential advantage of B.1.1.7 vs local variants. CA has B.1.427, B.1.429 which had a 29% higher household attack rate doi.org/10.1101/2021.0…. If B.1.1.7 Rt is 54-89% higher than D614G nature.com/articles/s4158…, then advantage over B.1.427/9 would be 19-47%
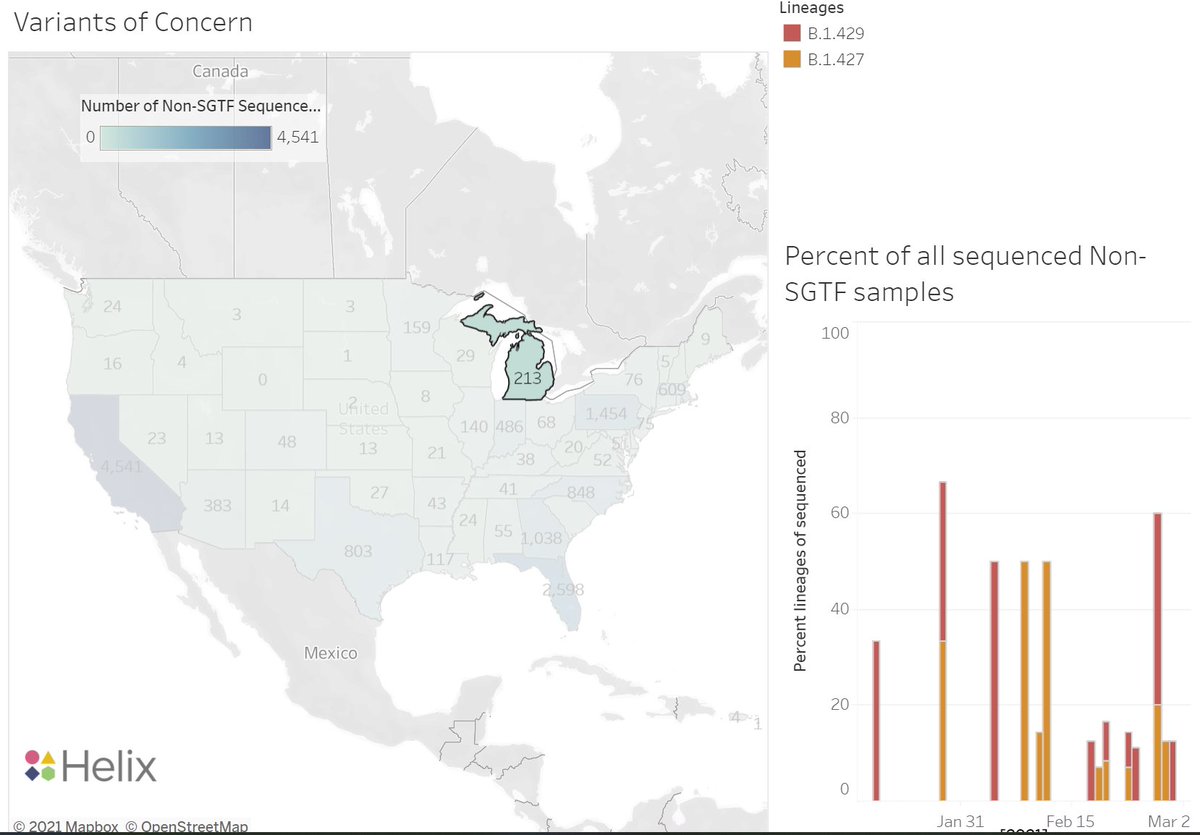
It appears B.1.427/9 are lower freq in MI, so possible that slower rise in B.1.1.7 freq in CA vs MI is due to competition in CA b/w B.1.1.7 & B.1.427/9, but this is speculative at this point & MI might also have more transmissible lineages than D614G.
-Another speculative possibility is recent paper @SarahDRasmussen doi.org/10.1101/2021.0… suggesting B.1.1.7 might have age-specific diffs in transmission advantage (i.e. kids transmit B.1.1.7 more than adults) & states might differ in school transmission. Highly speculative!

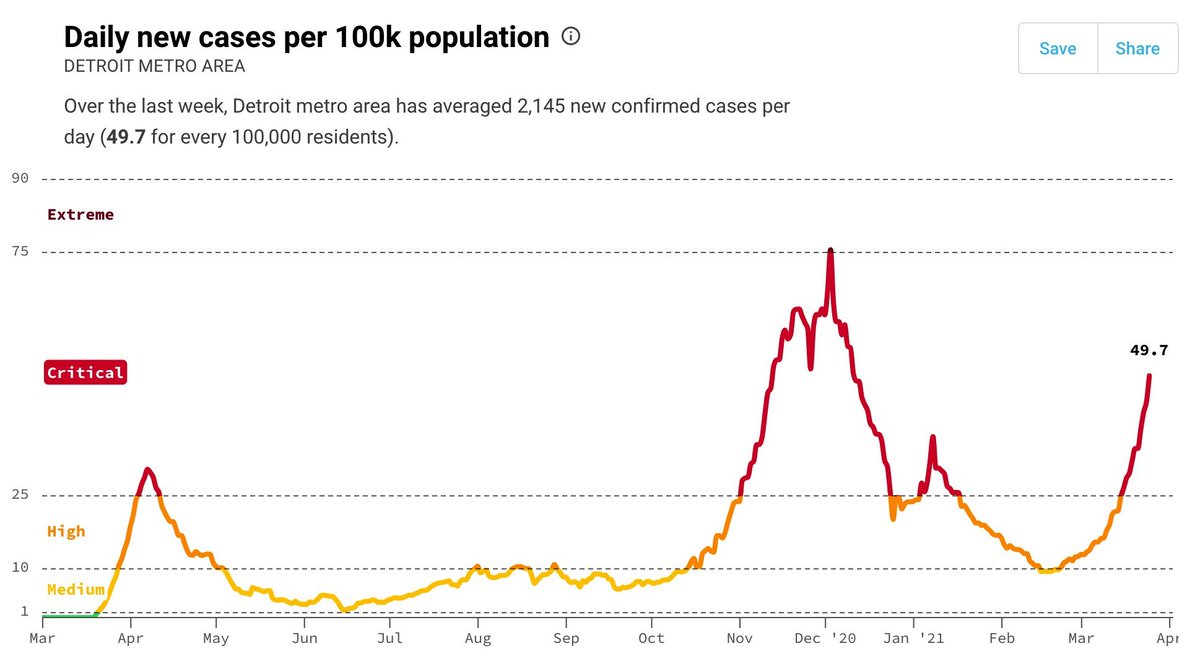
Why does the differential growth in frequency of B.1.1.7 among locations matter? b/c in much of the US cases were falling rapidly in Jan-Feb, but have started rising again in some places (rapidly in MI).
Reason for fall in Jan-Feb is likely combination of acquired immunity from surge in Nov-Dec plus subsequent restrictions. Now restrictions are being lifted and surges are occurring in some places (MI) but not others (CA).
Whether B.1.1.7 will cause new surge in cases as it rises in frequency will depend on differential advantage over local variants, current transmission rates Rt (which reflect immunity & social interactions). If Rt=0.66 w/out B.1.1.7 & advantage is <50%, Rt<1 & no surge, (cont)
assuming behavioral changes don't increase Rt. But if Rt=0.66 & B.1.1.7 advantage is 75%, then then Rt=1.16 & cases will increase 16% every 6d w/ B.1.1.7 dominant. Is this why MI is increasing & CA decreasing?
Thus, determining reason for differential growth of B.1.1.7 will inform whether additional restrictions will be needed to keep cases in check as it increases in freq or not. This is very important as people are planning for next 3 months.
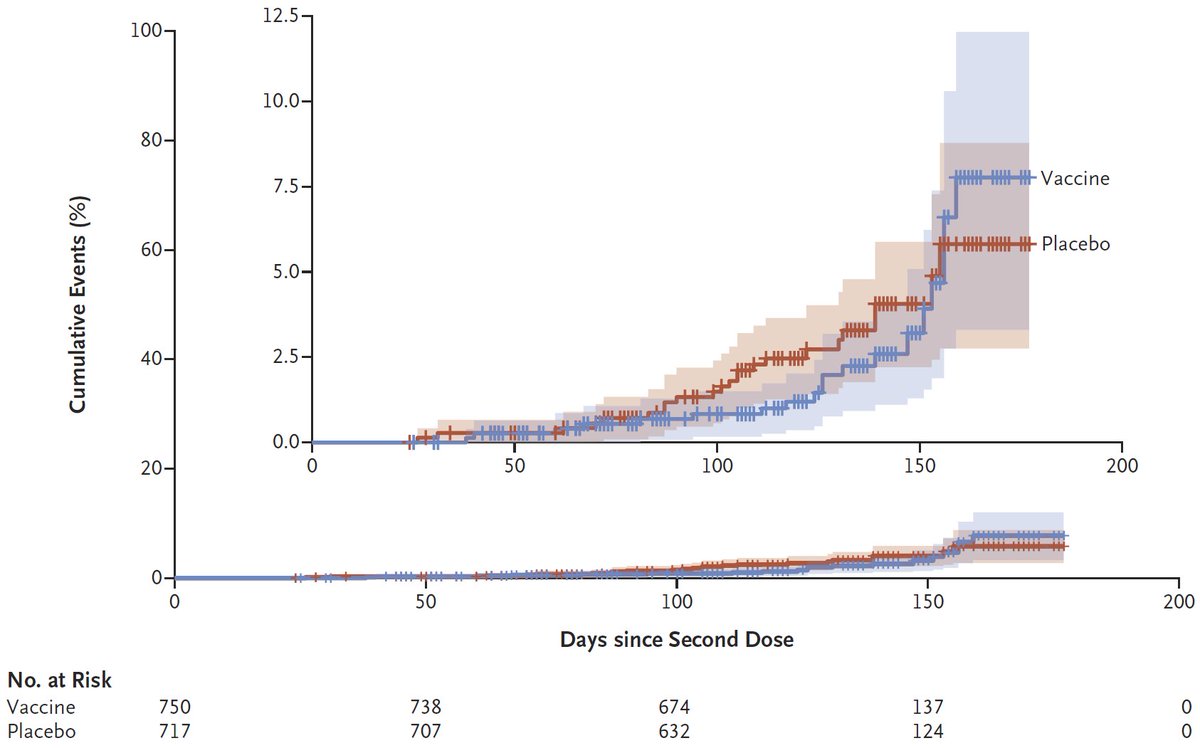
A big ace up our sleeve is vaccination! If we can quickly vaccinate population before B.1.1.7 increases in frequency, we can push Rt well below 1. Vaccines are very effective against B.1.1.7 so far (i.e. w/out E484K mutation, so I hope we can pull this off!
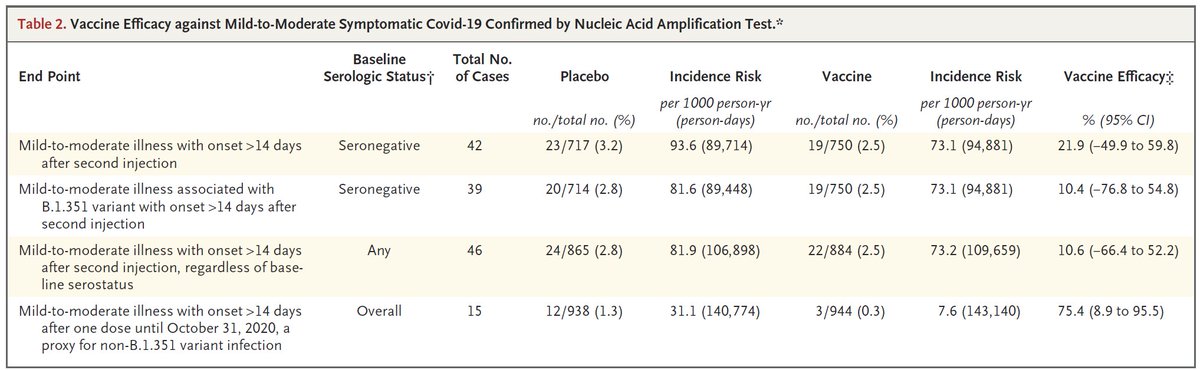
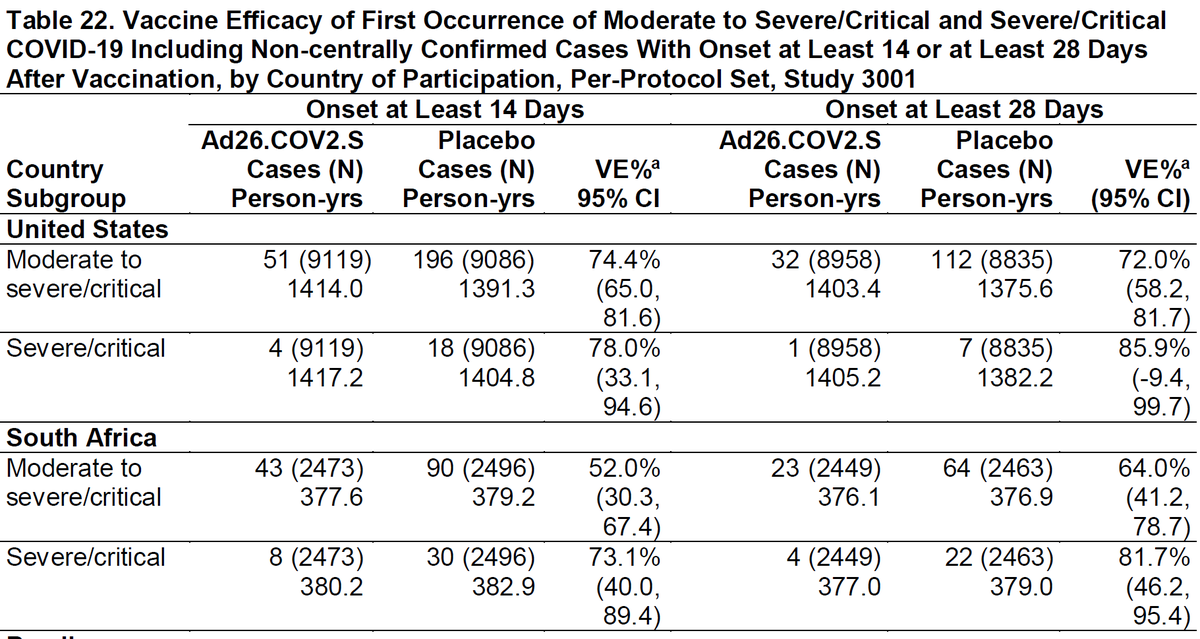
Obvious lurking concern is whether immune escape variants (e.g. B.1.351) will spread in partly (& later more fully) vaccinated populations. I hope the answer is poorly, but no hard data to know yet.
Clarification: All plots here show the FREQUENCY of B.1.1.7, so they show changes RELATIVE to other variants. Factors that increase Rt (e.g. less restrictions, social behavior) wouldn't affect rate of frequency increase unless they affect the variants differently.
• • •
Missing some Tweet in this thread? You can try to
force a refresh