Having now worked it's way through the @Telegraph system: with @louisemarsha11, our take on the plans for replacing Public Health England. 🧵
tl,dr: we need a more, not less, joined up system if we're serious about health & inequalities
No £-wall🔓
telegraph.co.uk/global-health/…
tl,dr: we need a more, not less, joined up system if we're serious about health & inequalities
No £-wall🔓
telegraph.co.uk/global-health/…
PHE is being split into the UK Health Security Agency (UKHSA which also includes Test&Trace) - focusing on external threats like pandemics
and the Office for Health Promotion - focusing on health improvement and inequalities, such as obesity and tobacco.
gov.uk/government/pub…
and the Office for Health Promotion - focusing on health improvement and inequalities, such as obesity and tobacco.
gov.uk/government/pub…
As we wrote at the time, it's a risky business reorganising public health in the middle of a pandemic.
telegraph.co.uk/global-health/…
telegraph.co.uk/global-health/…
COVID loves inequalities.
The pandemic has exposed and exacerbated the deep rooted differences in health and opportunity across society.
The pandemic has exposed and exacerbated the deep rooted differences in health and opportunity across society.
Levelling up is an issue of social justice.
But it affects everyone *not* just the most vulnerable:
- it will help tackle the pandemic
- it will accelerate the economic recovery
- it will improve national resilience against the next major health or economic shock
But it affects everyone *not* just the most vulnerable:
- it will help tackle the pandemic
- it will accelerate the economic recovery
- it will improve national resilience against the next major health or economic shock
People who are healthier feel better, they are more productive, they play a greater role in their communities.
Health is an asset.
health.org.uk/publications/t…
Health is an asset.
health.org.uk/publications/t…
People living in deprived areas and from minority ethnic communities have not only been more likely to get COVID, but they have had worse outcomes once infected.
gov.uk/government/pub…
gov.uk/government/pub…
These were often people who couldn’t work from home because they are carers/nurses, or keep supermarkets stacked, or deliver our packages.
The very people who kept the country going paid the biggest price.
telegraph.co.uk/global-health/…
The very people who kept the country going paid the biggest price.
telegraph.co.uk/global-health/…
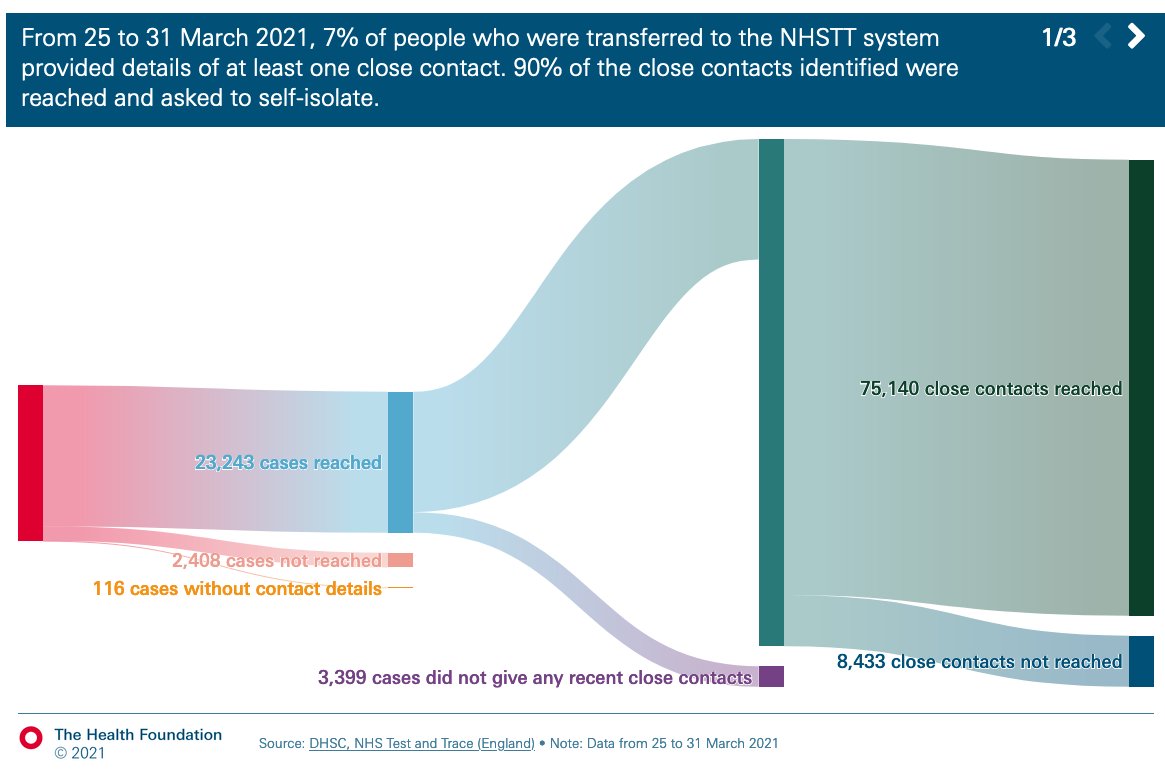
And when infected or identified as a close contact of someone with Covid, these same individuals were the least able to self isolate.
bmj.com/content/372/bm…
bmj.com/content/372/bm…
Around 1 in 3 social care staff are on the national living minimum wage, 1 in 4 are on zero-hours contracts.
Insecure jobs and casual work can mean the appalling choice of staying at home to protect colleagues and limit spread, or going to work to be able to pay the rent.
Insecure jobs and casual work can mean the appalling choice of staying at home to protect colleagues and limit spread, or going to work to be able to pay the rent.
Even at home, cramped housing often means people can't effectively isolate from family members/housemates, further increasing risk of transmission.
Until the underlying factors driving ongoing high case rates - like housing and employment - are addressed, we will keep experiencing outbreaks with the potential for new and more virulent viral variants to emerge.
And further local lockdowns will simply mean that those places most in need of economic recovery suffer yet further.
@chrischirp wrote this excellent summary of COVID and inequalities.
blogs.bmj.com/bmj/2021/04/09…
@chrischirp wrote this excellent summary of COVID and inequalities.
blogs.bmj.com/bmj/2021/04/09…
Add to this, conditions like diabetes and heart disease are more common in deprived areas (and lead to worse Covid outcomes).
They are also largely preventable through health promotion measures like creating more green space, cleaner air, healthier food.
telegraph.co.uk/global-health/…
They are also largely preventable through health promotion measures like creating more green space, cleaner air, healthier food.
telegraph.co.uk/global-health/…
And this is why separating health protection from the rest of public health is a false dichotomy.
The reforms have the potential to create a more, rather than less, fragmented public health system.
The reforms have the potential to create a more, rather than less, fragmented public health system.
Some bits are welcome, like a new ministerial board to co-ordinate cross-government action on prevention, but there's still no independent scrutiny of gov actions on health and inequals.
There's also recognition of the importance of local gov & Directors of Public Health
But the public health grant – for local services on obesity, smoking, alcohol, sexual health etc – has had a real terms cut of 24% per head over the last five years
health.org.uk/news-and-comme…
But the public health grant – for local services on obesity, smoking, alcohol, sexual health etc – has had a real terms cut of 24% per head over the last five years
health.org.uk/news-and-comme…
Any organisational upheaval also leads to workforce attrition.
Over the past 12 months, public health professionals across the country have worked night and day to keep the nation safe.
Over the past 12 months, public health professionals across the country have worked night and day to keep the nation safe.
They’ve tracked how the virus spreads & led research; managed cases/outbreaks in the most complex settings; they lead the ID of new potentially dangerous viral variants to limit their spread.
They have done this & more+++ with huge dedication & often little recognition.
They have done this & more+++ with huge dedication & often little recognition.
They are physically and mentally exhausted, and there is a risk that many highly skilled professionals will leave during the transition unless staff wellbeing and workforce planning are taken seriously.
bma.org.uk/news-and-opini…
bma.org.uk/news-and-opini…
As health secretary Matt Hancock said in his announcement, “levelling up health is the most important levelling up of all”.
To do this, the government needs a public health system that can work more closely across health security, health promotion, and inequalities.
To do this, the government needs a public health system that can work more closely across health security, health promotion, and inequalities.
The new structures may threaten this close working, but as with any new system bedding in, there is still the opportunity to shape things for the better.
Including respond to the current consultation, closing 26th April.
consultations.dhsc.gov.uk/PublicHealthSy…
Including respond to the current consultation, closing 26th April.
consultations.dhsc.gov.uk/PublicHealthSy…
The pandemic has highlighted the outstanding work of public health individuals, teams, & orgs.
But it's also exposed the scale of the task ahead.
I'm v optimistic our public health leaders will be making the case for a stronger system. I just hope someone's listening.
But it's also exposed the scale of the task ahead.
I'm v optimistic our public health leaders will be making the case for a stronger system. I just hope someone's listening.
Our new Telegraph piece on the new PH system in Eng. @felly500 @trishgreenhalgh @deb_cohen @martinmckee @chrischirp @mgtmccartney
@ADPHUK @Jeanelleuk @fascinatorfun @profchrisham @petermbenglish @HPIAndyCowper @Davewwest @HSJEditor @KateAlvanley @IndependentSage @nedwards_1
@ADPHUK @Jeanelleuk @fascinatorfun @profchrisham @petermbenglish @HPIAndyCowper @Davewwest @HSJEditor @KateAlvanley @IndependentSage @nedwards_1
• • •
Missing some Tweet in this thread? You can try to
force a refresh