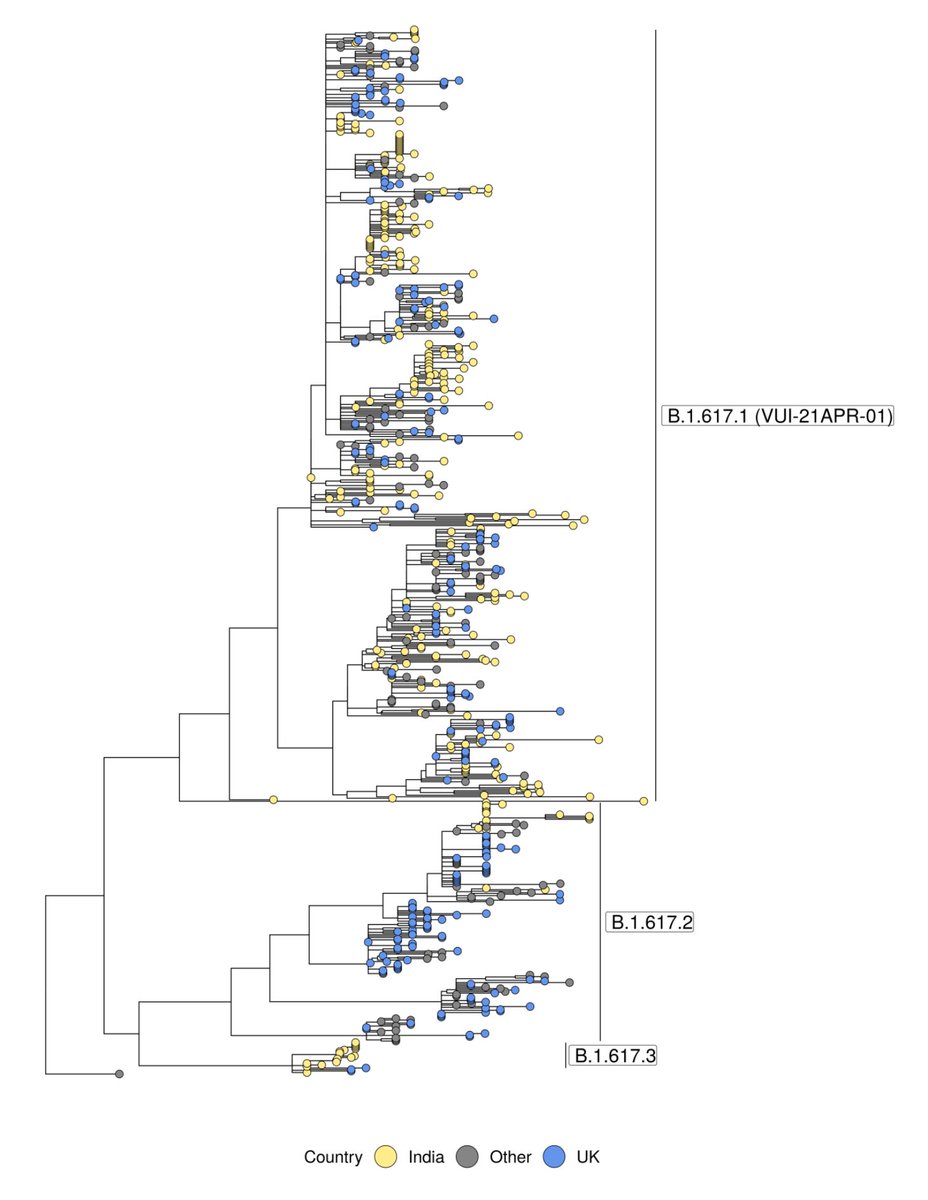
Last week @PHE_uk designated B.1.617.2 a VOC (excellent summary from @kallmemeg below). Today we released another week's worth of surveillance genomes at covid19.sanger.ac.uk, and I'd like to walk through some of the features & findings. 🧵
https://twitter.com/kallmemeg/status/1390670671139774467?s=20
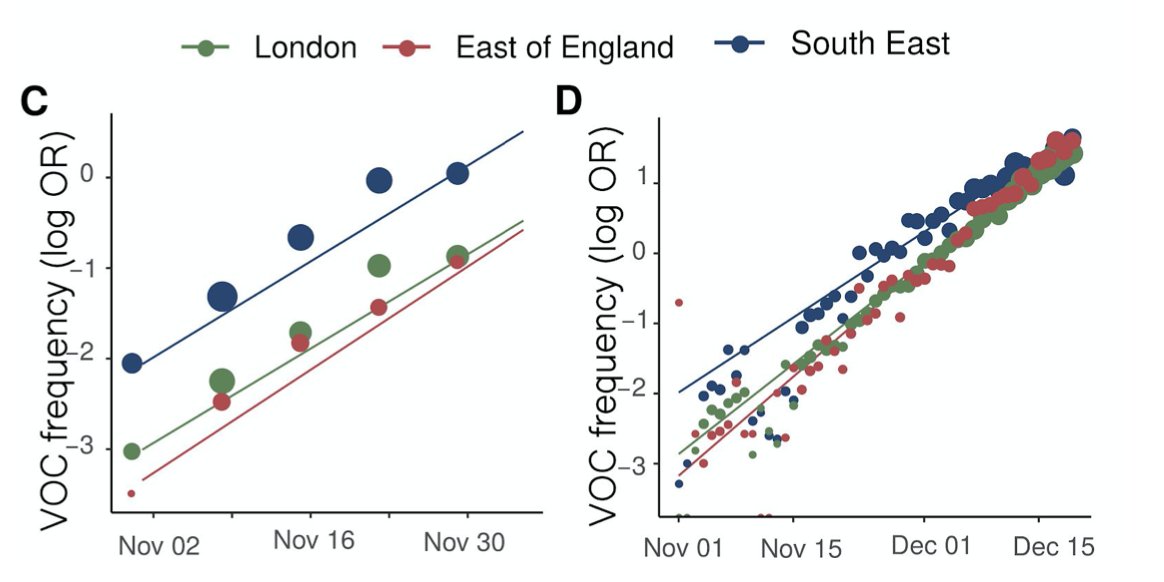
First, headline result, as reported by others, is that B.1.617.2 has hit 6% in England in our 2-week rolling average (>10% in the most recent week). Other VOCs & VUIs steady. 

It is hard to know exactly what this means for transmissibility. There were hundreds of imported cases in a short span, and while those are not counted here, they arrived in both a quantity and at a moment of loosening restriction that we have not seen before for other variants.
That mix makes it inevitable that there will be hotspots of community transmission (e.g. Bolton). Low case numbers more broadly can make it look alarming, and it certainly is something that should be monitored, and against which public health measures should be deployed.
For those using our data, please take care around local authorities with low numbers. For instance, South Northamptonshire looks scary with 80% B.1.617.2, but that's based on a handful of sequences, so might be noise.

The fundamental question is how well vaccines work against this variant, and I know that lots of excellent scientists are working around the clock on that question. There's evidence on other variants that the effect is likely modest, so I'm cautiously optimistic.
Finally, while more evidence is accumulated, the plan remains the same: vaccinate as widely and quickly as possible; behave responsibly, even as restrictions are loosened.
• • •
Missing some Tweet in this thread? You can try to
force a refresh