This is good news.
The longer it takes to statistically tell difference between vax effectiveness against variants the smaller the actual dip (if any) in protection will be.
1/
The longer it takes to statistically tell difference between vax effectiveness against variants the smaller the actual dip (if any) in protection will be.
1/
https://twitter.com/jburnmurdoch/status/1396015155872509953
In randomised control trials we can be confident in vax effect after only 100+ infections because selection bias and confounding variables between the vaxxed and unvaxxed comparison populations are (e)limited by the randomisation process.
2/
2/
This is not the case when we do retrospective observational studies - like vax effectiveness against variants in the field.
The statistical analysis is more challenging. There are biases in who is vaxxed or infected, living, working, mixing patterns, medical health/immunity.
3/
The statistical analysis is more challenging. There are biases in who is vaxxed or infected, living, working, mixing patterns, medical health/immunity.
3/
To account for these need to do matching/case-control or logistic regression to find true odds ratio between infxn risk of vaxxed vs unvaxxed.
cf RCT where Chi-squared or T test test could do.
4/
cf RCT where Chi-squared or T test test could do.
4/
NB I still do simple short cuts for twitter analysis with point estimates of field vax effectiveness...
But if we're being proper clinical scientists trying to get robust publishable/usable data we should have higher standards!
5/
But if we're being proper clinical scientists trying to get robust publishable/usable data we should have higher standards!
5/
For proper analysis the retrospective cohorts have to be much larger with many events (infections). ~10X or more vs RCT.
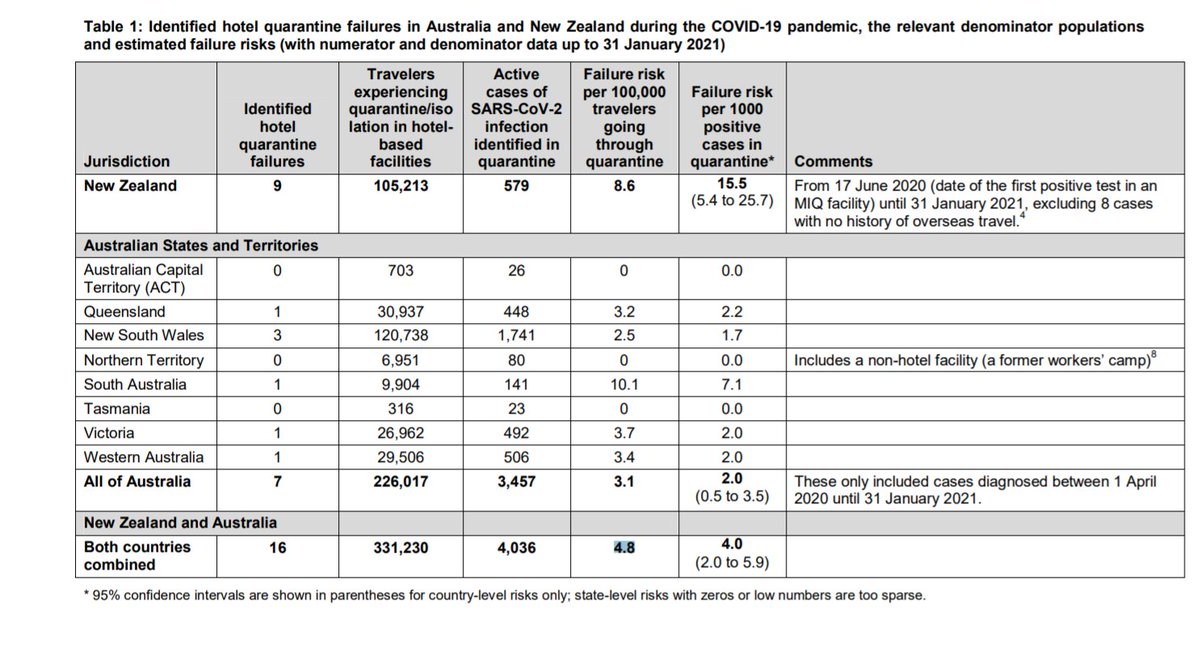
So far there have only been 3.4k B1.617.2 cases identified. Predominantly in unvaxxed young people - so the vaxxed v unvaxxed groups will be v unbalanced.
6/
So far there have only been 3.4k B1.617.2 cases identified. Predominantly in unvaxxed young people - so the vaxxed v unvaxxed groups will be v unbalanced.
6/
To get to a point when confidence intervals no longer overlap it will take many more weeks if there is a small difference.
Applies to 1 dose only effectiveness too which is even more challenging due to differing time windows of population in that state/community infxn rate.
Applies to 1 dose only effectiveness too which is even more challenging due to differing time windows of population in that state/community infxn rate.
• • •
Missing some Tweet in this thread? You can try to
force a refresh