70% [68,72] of England's Total population have now been infected or vaccinated.
Wall of immunity:
13% Infected
44% Vaccinated 1+
13% Both
Usual caveats: time lag after vax, not 100% protective, assumes random vaxxing probability of previously infected etc.
1/
Wall of immunity:
13% Infected
44% Vaccinated 1+
13% Both
Usual caveats: time lag after vax, not 100% protective, assumes random vaxxing probability of previously infected etc.
1/

Estimated numbers of people:
7.0m Infected only
24.7m Vaccinated only
7.5m Infected & vaccinated
17.1m unexposed and susceptible
2/
7.0m Infected only
24.7m Vaccinated only
7.5m Infected & vaccinated
17.1m unexposed and susceptible
2/

The remaining 17.1m unexposed/susceptible population is heavily skewed to younger age groups.
2/3 under 25
1/3 in school age kids 5-14yo
Outbreaks and cases will expectedly be concentrated in these groups now and increasingly <18 after current vax roll out plan completed.
3/
2/3 under 25
1/3 in school age kids 5-14yo
Outbreaks and cases will expectedly be concentrated in these groups now and increasingly <18 after current vax roll out plan completed.
3/

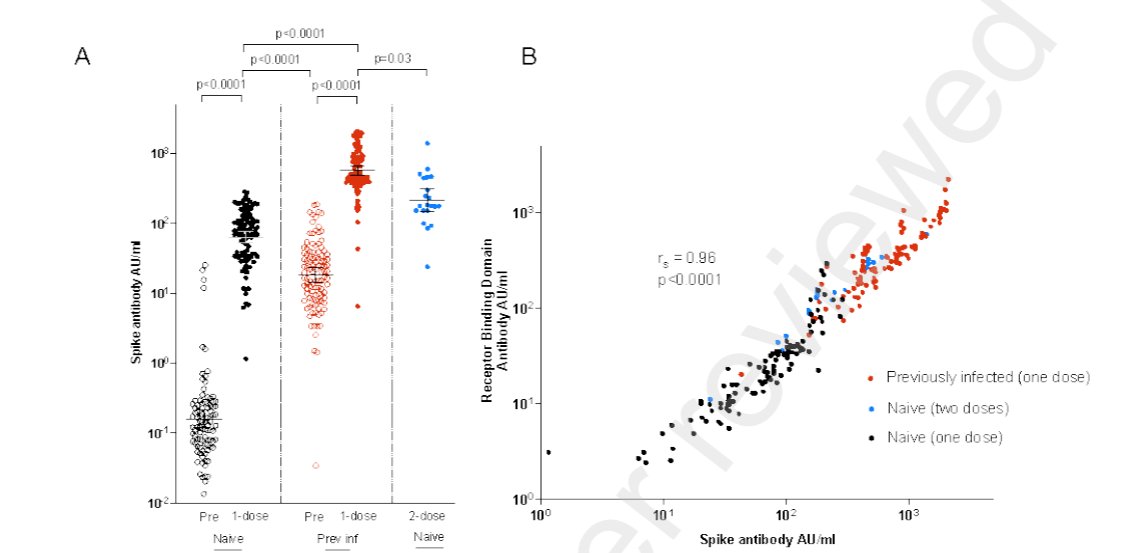
For the 70% people after vax1/2 doses, vax+infxn and previous infxn current weighted population average protection from symptomatic infection is 80-85%.
Protection for severe illness/hospitalization/death higher.
4/
Protection for severe illness/hospitalization/death higher.
4/
The end is in sight!
But as JVT would say it's the 88th minute and we're 3-2 up things can change.
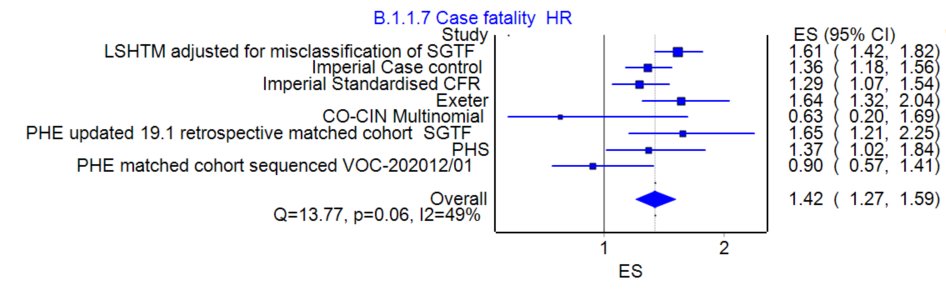
Variants with increased transmissibility or altered effectiveness of vaccines can cause issues depending on degree. @JamesWard73 has excellent analysis.
But as JVT would say it's the 88th minute and we're 3-2 up things can change.
Variants with increased transmissibility or altered effectiveness of vaccines can cause issues depending on degree. @JamesWard73 has excellent analysis.
https://twitter.com/JamesWard73/status/1396615795975798787
• • •
Missing some Tweet in this thread? You can try to
force a refresh