A cool case for #cardiotwitter #neurotwitter -- wondering if others have seen this happen!
A 70 yo W with history of HTN presented with significant IVH from a ruptured AVM.
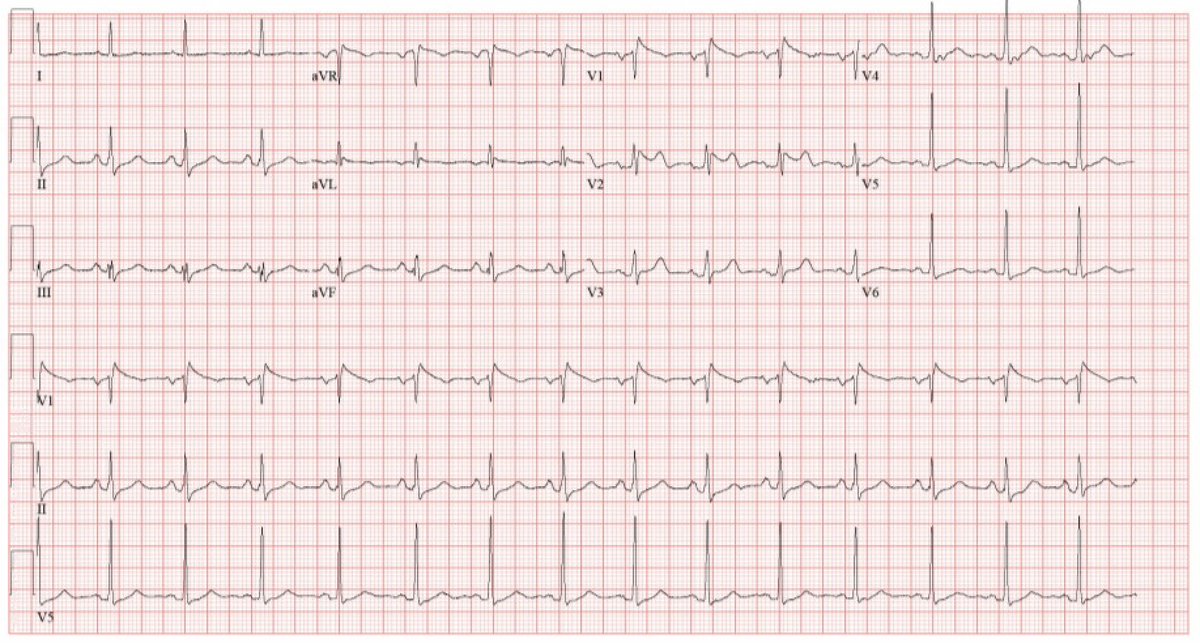
Admission EKG showed this:
A 70 yo W with history of HTN presented with significant IVH from a ruptured AVM.
Admission EKG showed this:

A #brugada pattern. She had no personal or family history of syncope / sudden death. And on admission (time of this EKG) she was not febrile. About 12 hours later we repeated the EKG:

Trops normal and ECHO later in the day demonstrated a normal EF and grade 1 DD, but no wall motion abnormality. No apical ballooning. There was mildly increase LV wall thickness.
Checked another EKG the next AM. Looks about the same.
There were no arrhythmias on tele. She continued to be afebrile.
There were no arrhythmias on tele. She continued to be afebrile.
A few days later (about 6 days out from IVH), she developed a pneumonia and spiked a temperature.
Repeat EKG demonstrated:
Repeat EKG demonstrated:
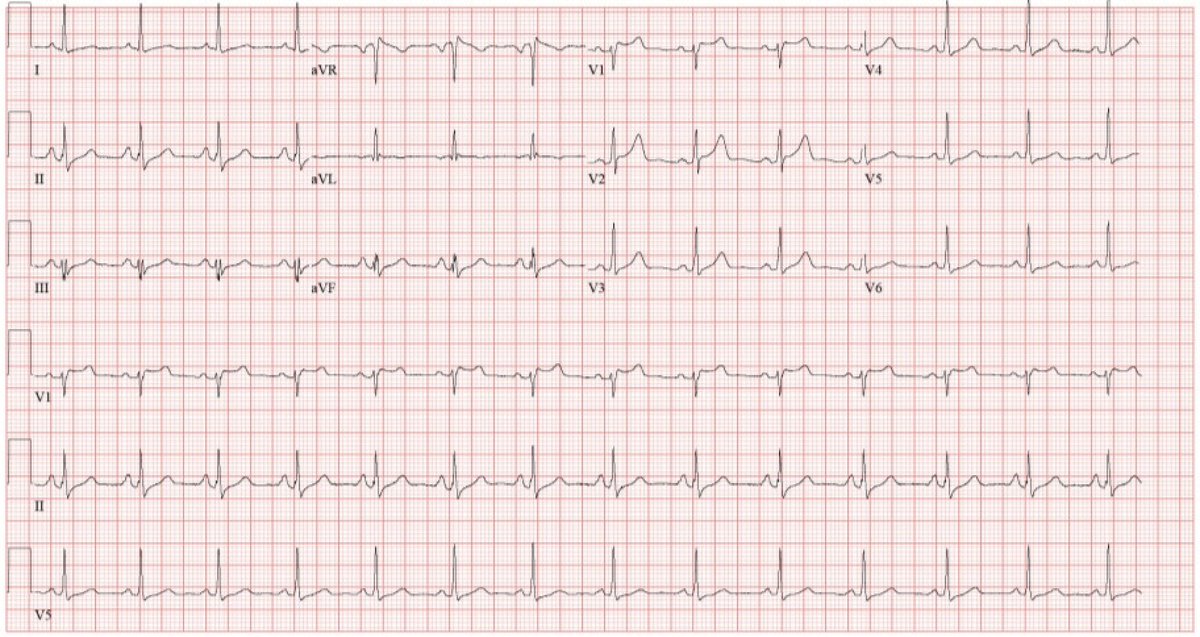
Absent Brugada pattern, despite the fever (1st of her admission).
So, #cardiotwitter, do we just chalk this up to a brain-heart ❤️🧠 connection thing? The stress of IVH? Inflammation? Never personally seen this pattern with neuro patients so I'm curious!
So, #cardiotwitter, do we just chalk this up to a brain-heart ❤️🧠 connection thing? The stress of IVH? Inflammation? Never personally seen this pattern with neuro patients so I'm curious!
And -- Is it likely to return? Or like all the QTc prolongations & other transient arrhythmias we find is this unlikely to reoccur.
Thoughts on why this pattern might be found with neuro injury?
@PPodrid @sgleeMD @guroledip @emoryheart @AaronLBerkowitz @Capt_Ammonia
Thoughts on why this pattern might be found with neuro injury?
@PPodrid @sgleeMD @guroledip @emoryheart @AaronLBerkowitz @Capt_Ammonia
• • •
Missing some Tweet in this thread? You can try to
force a refresh