#Nephrology #POCUS short story:
1/ Simple case, want to remind some pitfalls in routine practice.
There was a patient with orthostatic hypotension. Likely neurogenic secondary to amyloidosis.
Read the thread 🧵below:
#IMPOCUS #MedEd mini #tweetorial
1/ Simple case, want to remind some pitfalls in routine practice.
There was a patient with orthostatic hypotension. Likely neurogenic secondary to amyloidosis.
Read the thread 🧵below:
#IMPOCUS #MedEd mini #tweetorial
2/ Physician A orders IV albumin q 6 hours and keeps continuing because:
1. 'Formal' echo from 4 days ago reported a RAP of 3 mmHg = not high
2. 'Documented' weight showed 3 kg drop since admission
Interestingly, documented cumulative fluid balance is +4 L!
1. 'Formal' echo from 4 days ago reported a RAP of 3 mmHg = not high
2. 'Documented' weight showed 3 kg drop since admission
Interestingly, documented cumulative fluid balance is +4 L!
3/ Physician B comes in and performs physical examination (#POCUS). Supine BP is relatively low (SBP ~103 mmHg) but nothing different compared to patient-reported figures at home. Pt feels OK, on midodrine.
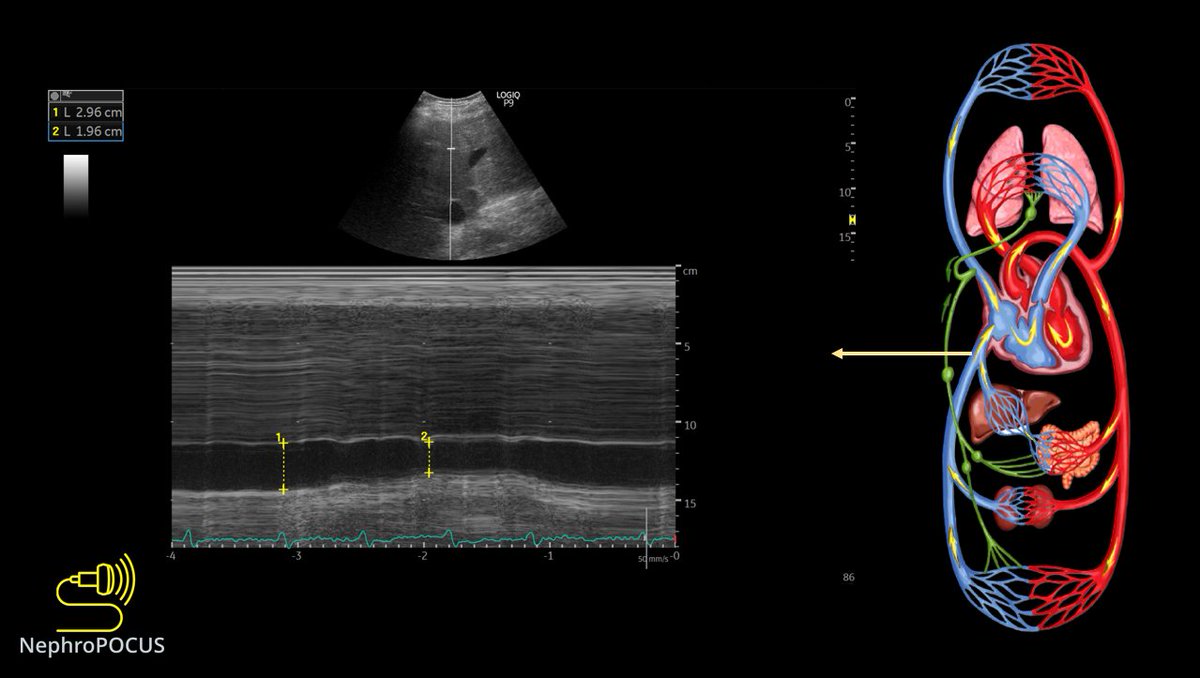
Here is the IVC👇
Here is the IVC👇
4/ 👆It is >2 cm, <50% collapsible. Definitely not consistent with a low right atrial pressure.
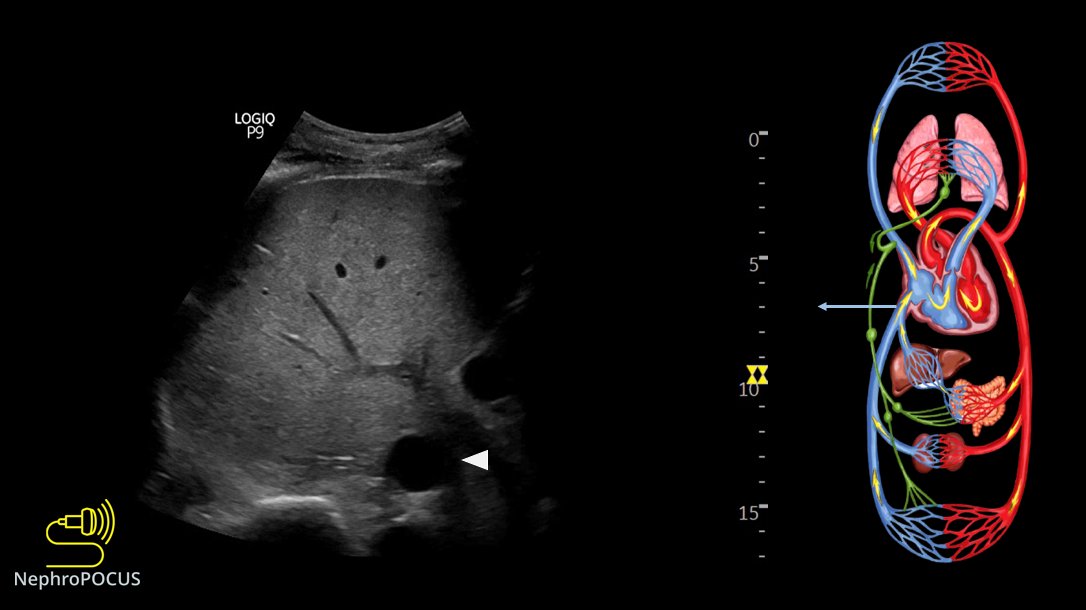
Here is hepatic vein #VExUS 👇
RAP meter shown on the top for beginners.
Here is hepatic vein #VExUS 👇
RAP meter shown on the top for beginners.

5/ 👆 Shows D-only pattern consistent with severe congestion.
There is not a lot of TR👇 Apical 4C shows bi-atrial enlargement (amyloidosis)
There is not a lot of TR👇 Apical 4C shows bi-atrial enlargement (amyloidosis)

7/ Intra-renal #VExUS 👇
D-only pattern consistent with severe congestion. Color flow is great but not a happy kidney!
D-only pattern consistent with severe congestion. Color flow is great but not a happy kidney!

8/ Management: Strongly recommend to stop all the fluids (colloids/crystalloids). Hypotension is not due to hypovolemia. Consider drugs such as Droxidopa/pyridostigmine and maybe neurology consultation.
Take-home points:
Take-home points:

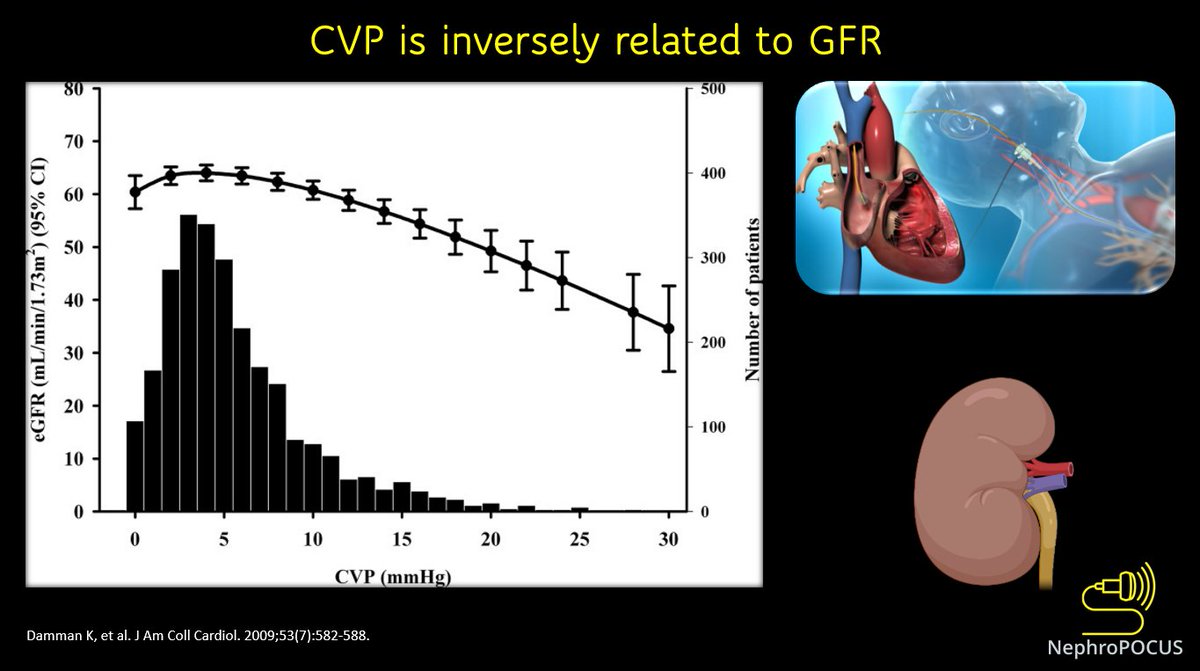
9/ Interesting to be able to 'visualize' what iatrogenic fluid overload does to the circulation! #VExUS #POCUS
Cc @ThinkingCC @khaycock2 @curromir @ArgaizR @DrBaudy @Scottiedoc1 @RJonesSonoEM @katiewiskar @tulunsokit @Wilkinsonjonny
Cc @ThinkingCC @khaycock2 @curromir @ArgaizR @DrBaudy @Scottiedoc1 @RJonesSonoEM @katiewiskar @tulunsokit @Wilkinsonjonny
• • •
Missing some Tweet in this thread? You can try to
force a refresh