
1/9. In England, #SARSCoV2 infection rates in school-aged kids & #COVID19 outbreaks have both ⬆️ in recent weeks (latest data 4 July) but that does not change the narrative on kids & their role in infection/transmission in school
Here’s why … 🧵
👉 assets.publishing.service.gov.uk/government/upl…
Here’s why … 🧵
👉 assets.publishing.service.gov.uk/government/upl…
2/9. No one has claimed that kids don’t get infected or don’t transmit #SARSCoV2 to others. But the data suggest that lower risk with kids than adults. Eg. We don’t see two-thirds of staff/students infected in a single outbreak as we do in care homes 👉 thelancet.com/journals/eclin…
3/9. We & others have shown that #SARSCoV2 cases & outbreaks reflect community infection rates. Cases in kids generally follow adults *unless* adults are in lockdown & kids continue to go to school. This happened in Nov/Dec 2020 & Mar/Apr 2021. See👇👇
👉 journalofinfection.com/article/S0163-…
👉 journalofinfection.com/article/S0163-…


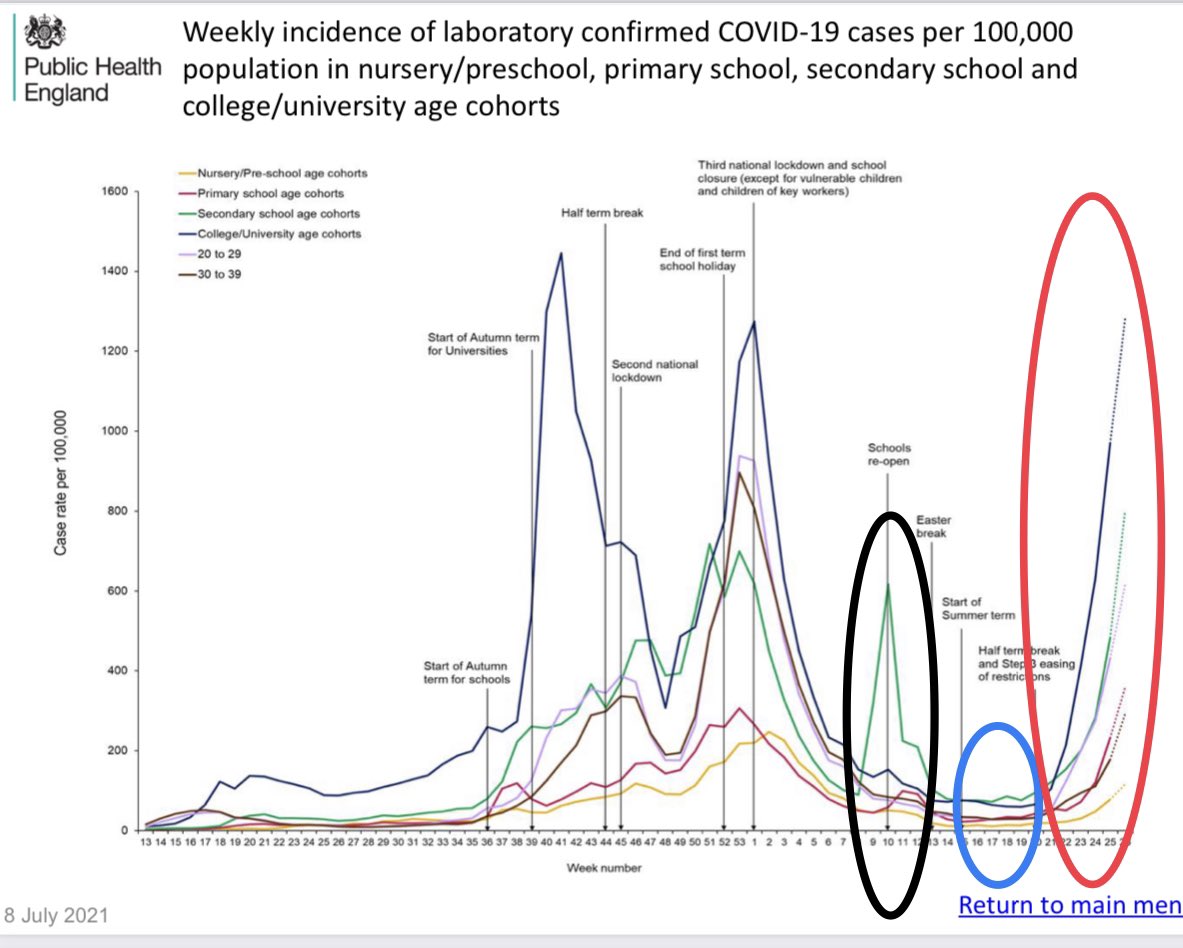
4/9. After the Jan 2021 lockdown, schools opened on 08 March for 3 weeks (black circle). Cases were highest in secondary school children when mass LFD testing was implemented before they were allowed back in school, but then declined & remained low (they also wore masks in class)

5/9. After the Easter holidays, too, infection rates remained low in all school-aged children for *6 weeks* since mid-April (blue circle), when most of the adults were still in national lockdown & despite the emergence of the Delta variant in England - outbreaks too were limited
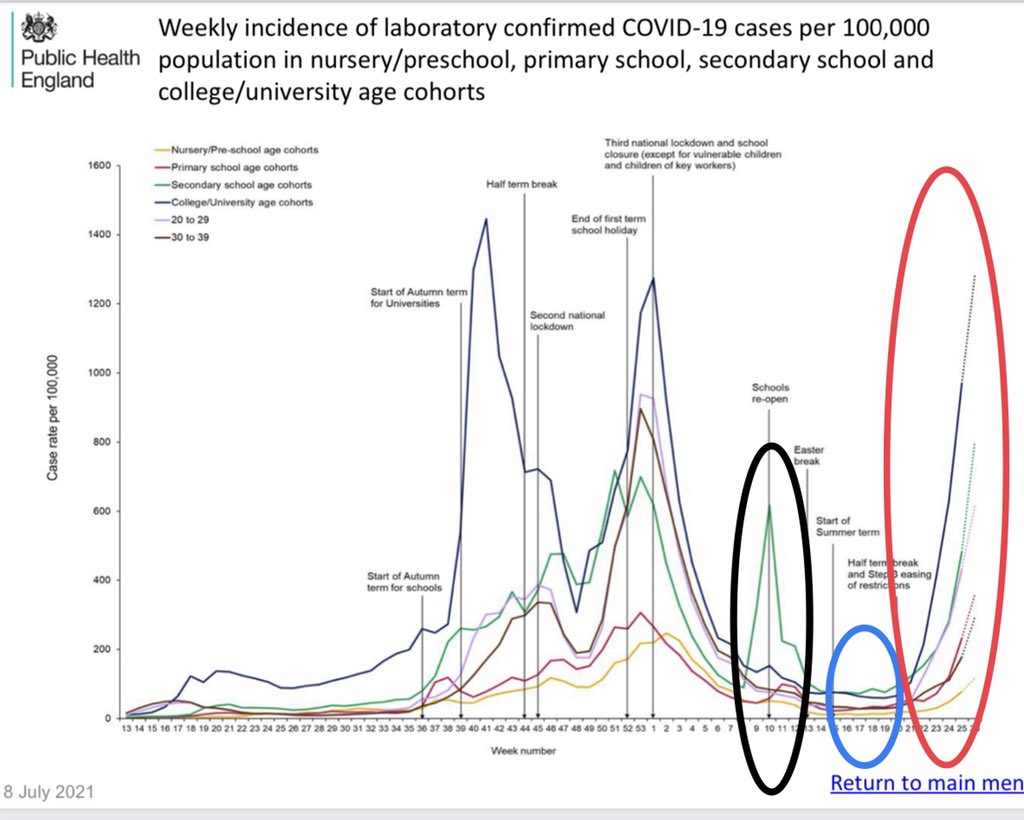

6/9. From 17 May (week 20), we eased into step 3 of opening lockdown & cases ⬆️ rapidly in all ages, esp 20-29 & 10-19 year-olds. Only 1 of these groups was in school.
Opening lockdown likely increased contacts & transmission chains outside schools
👉 assets.publishing.service.gov.uk/government/upl…
Opening lockdown likely increased contacts & transmission chains outside schools
👉 assets.publishing.service.gov.uk/government/upl…

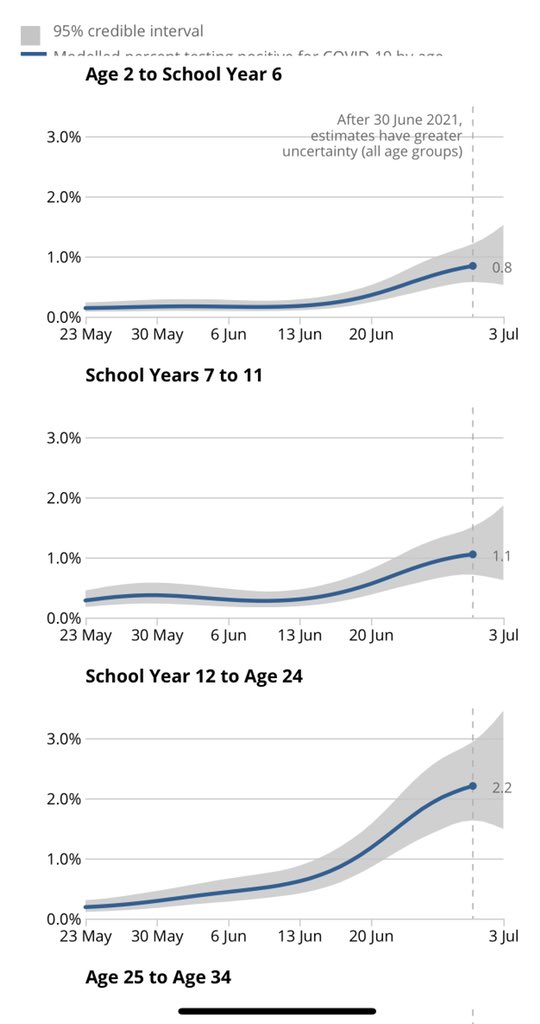
7/9. Interestingly, infections by age are better seen in ONS Survey (community testing, random households). Infections in primary & secondary school-aged kids remained low & only started ⬆️ after cases started increasing in year 12 to age 24 (~mid-June) 👉ons.gov.uk/peoplepopulati…
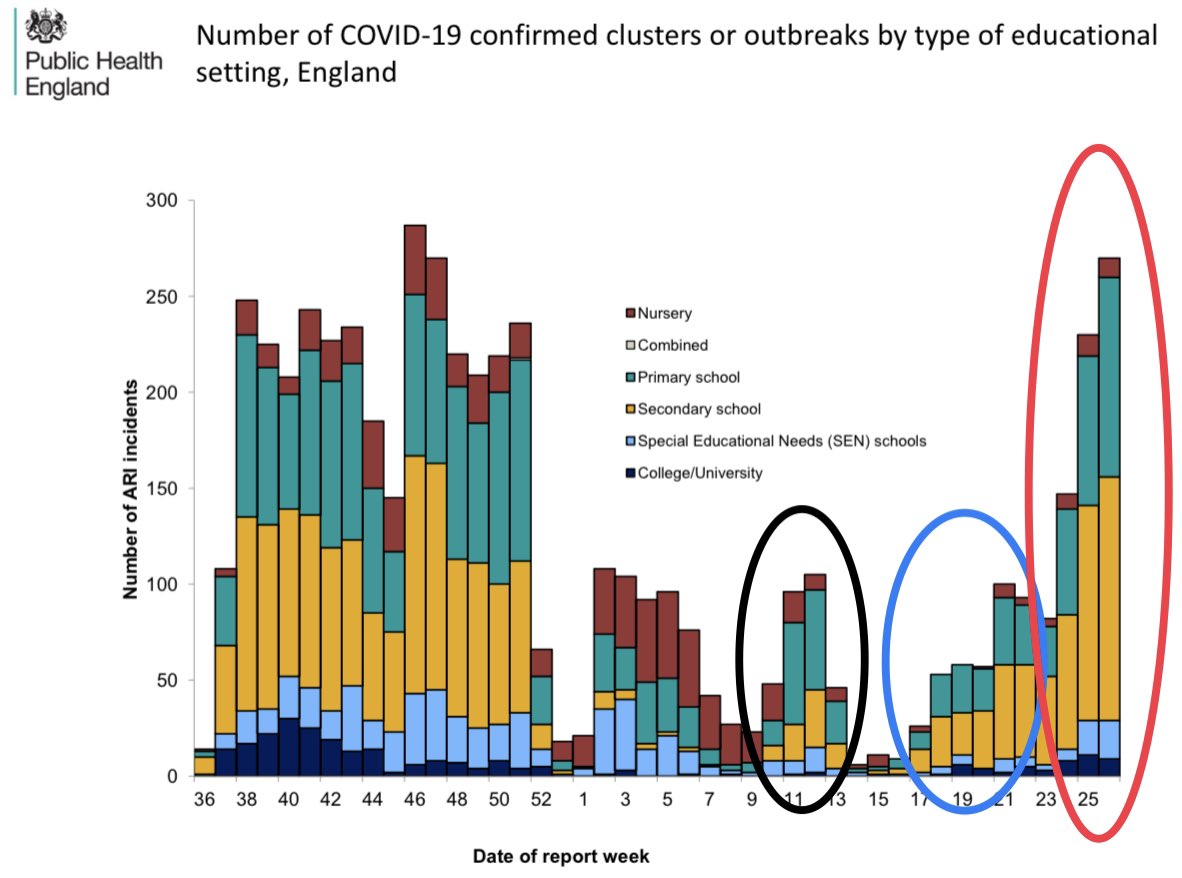
8/9. School outbreaks have also increased, especially after 17 May (red circle), although important to remember there are ~24,000 schools & <300 outbreaks (1-2% of schools). Also, outbreaks are defined as 2+ cases but these cases don’t have to be linked or infected in school 👇

9/9. In conclusion, #SARSCoV2 cases/outbreaks in schools remained ⬇️ when adults were in lockdown. This changed when lockdown eased (17 May). Vaccines will help keep community infection ⬇️ but we need more evidence-based mitigations in schools not just 4 #SARSCoV2 but all viruses
• • •
Missing some Tweet in this thread? You can try to
force a refresh








