My (preaching to the choir) 🔥 take: digital educational skills -- whether teaching on #MedTwitter, podcasting, or making videos -- are essential #meded skills for the 21st century. And we can teach these to future educators.
A Tweetorial🧵:
A Tweetorial🧵:
Last year, @ShreyaTrivediMD @StaciSaundersMD and I at @iMedEducation started a curriculum to teach digital educational skills to our @BIDMC_IM residents.
We just published this article going over our curriculum and providing tips for you to do it too: pubmed.ncbi.nlm.nih.gov/34013623/
We just published this article going over our curriculum and providing tips for you to do it too: pubmed.ncbi.nlm.nih.gov/34013623/
We ended up integrating our curriculum into a pre-existing one-to-two week Senior Teacher rotation, which had two great benefits:
1⃣MUCH easier to get off the ground
2⃣Stressed that traditional educational principles are transferable for teaching digitally
1⃣MUCH easier to get off the ground
2⃣Stressed that traditional educational principles are transferable for teaching digitally

There is SO MUCH in digital education. What do you teach‽ Shreya and I performed a needs assessment (focus groups) and found that the most commonly-used educational materials were podcasting, Twitter, and infographics.
But this might change, so you have to continuously assess
But this might change, so you have to continuously assess
Because of time limits (podcasting takes⌛️), we focused on infographics and Tweetorials. Residents get a 3 hour skills curriculum then hands-on coaching in drafting, editing, and finally a peer-review process (through us and expert reviewers)
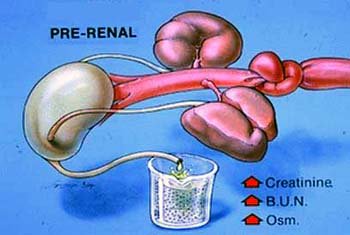
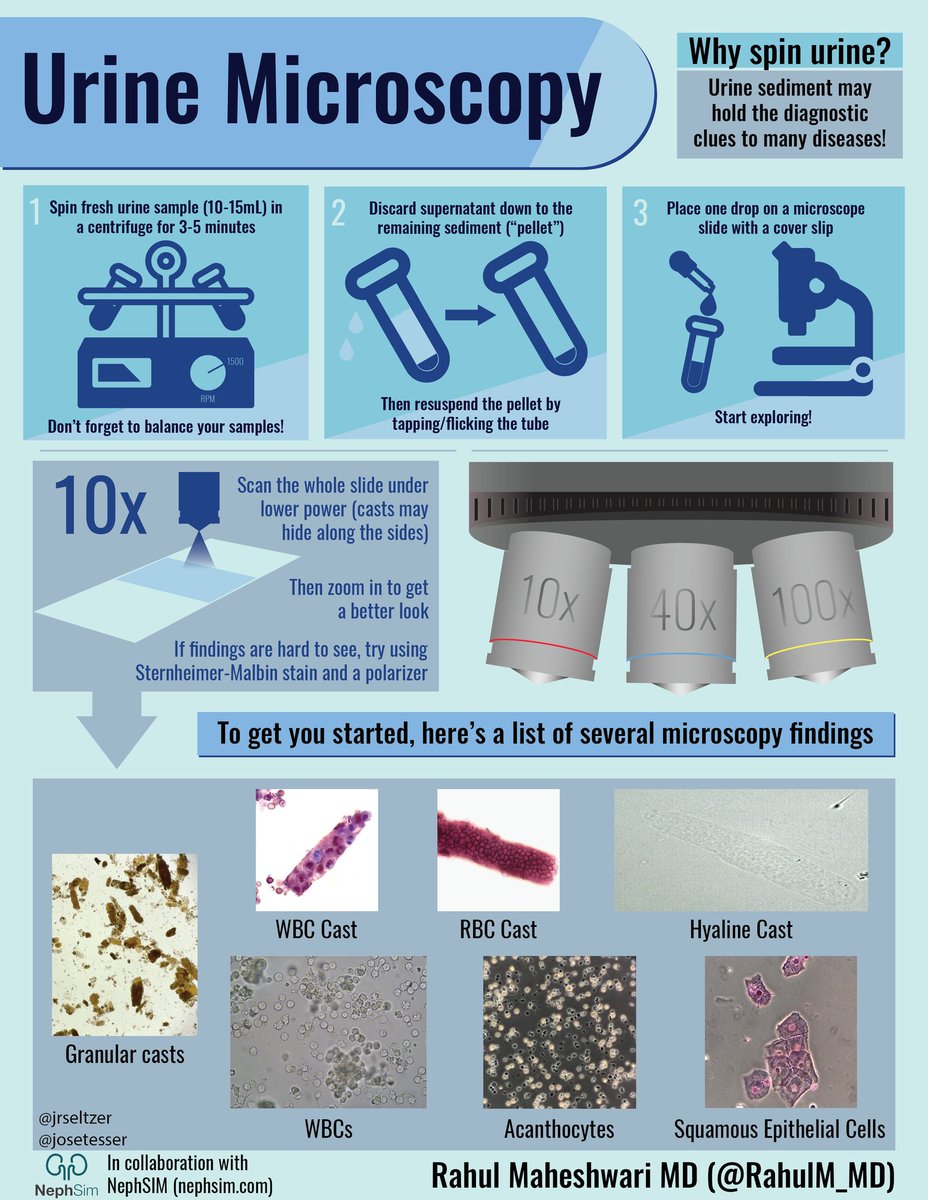
Example from talented @RahulM_MD
Example from talented @RahulM_MD
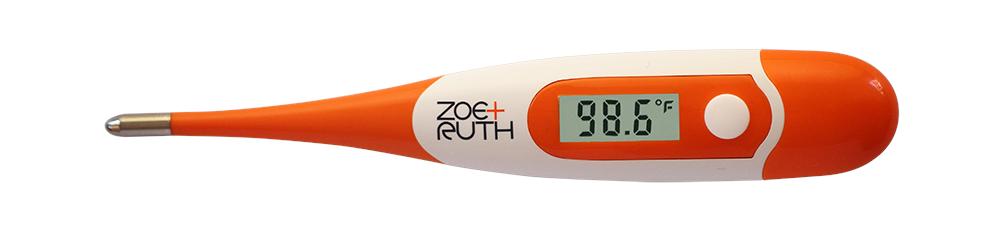
We’ve been shocked at the reach of some of our learners. @JennyShihMD made this amazing Tweetorial on treating fevers (reviewed by @AvrahamCooperMD) which received almost 150k impressions!
https://twitter.com/iMedEducation/status/1362164300916252677
We’ve learned a lot along the way. IMO what makes digital education special is that it takes place in a virtual community. You don’t just “put something out there” -- your teaching is intertwined with the community. Navigating that takes skill, which we’re trying to teach.
We’re also trying to train and recruit faculty experts. In fact, @StaciSaundersMD had never made visuals before this, and now she’s a pro!
This year, we’ve recruited a larger group of digital education experts at BIDMC like @jlberrymd and @swinndong.
This year, we’ve recruited a larger group of digital education experts at BIDMC like @jlberrymd and @swinndong.
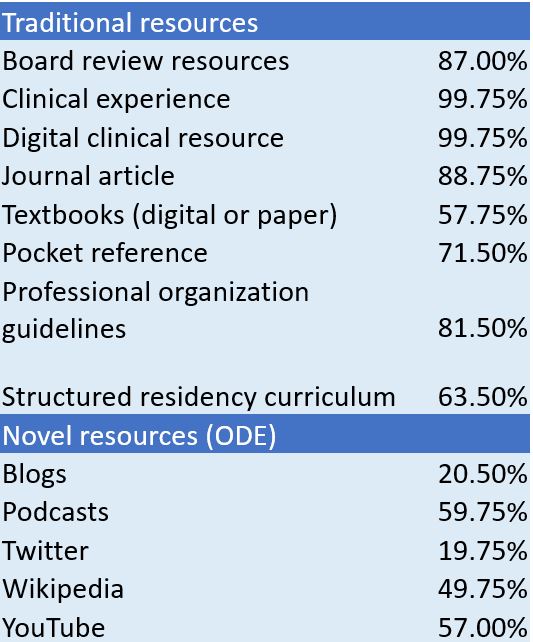
There’s no question that digital education is the future of #meded -- podcasts and videos are already more popular than textbooks for our residents (source: pubmed.ncbi.nlm.nih.gov/33506391/).
We *all* need to learn this stuff.
We *all* need to learn this stuff.
So if you’re interested in launching a digital education curriculum at your own institution, feel free to reach out to any of us! (and the paper’s not open access, so if you need the PDF feel free to DM or e-mail as well).
This is a future I'm excited to build together!
This is a future I'm excited to build together!
• • •
Missing some Tweet in this thread? You can try to
force a refresh