As someone who broke the news to Israeli leaders on Sweden’s handling of COVID-19 in Mar. 2020, I am so distressed to be reading this now m.ynet.co.il/articles/hj30k…
When will Homo Sapiens realize that we can never stop a tiny virus & re-engineer human biology by force not smarts?
When will Homo Sapiens realize that we can never stop a tiny virus & re-engineer human biology by force not smarts?


Please note that the two translation are automatic. I give independent results from Microsoft and Google. The original is in Hebrew.
Taking this opportunity to rejoice in machine translation. It it so worthwhile to get used to its quirks.
Taking this opportunity to rejoice in machine translation. It it so worthwhile to get used to its quirks.

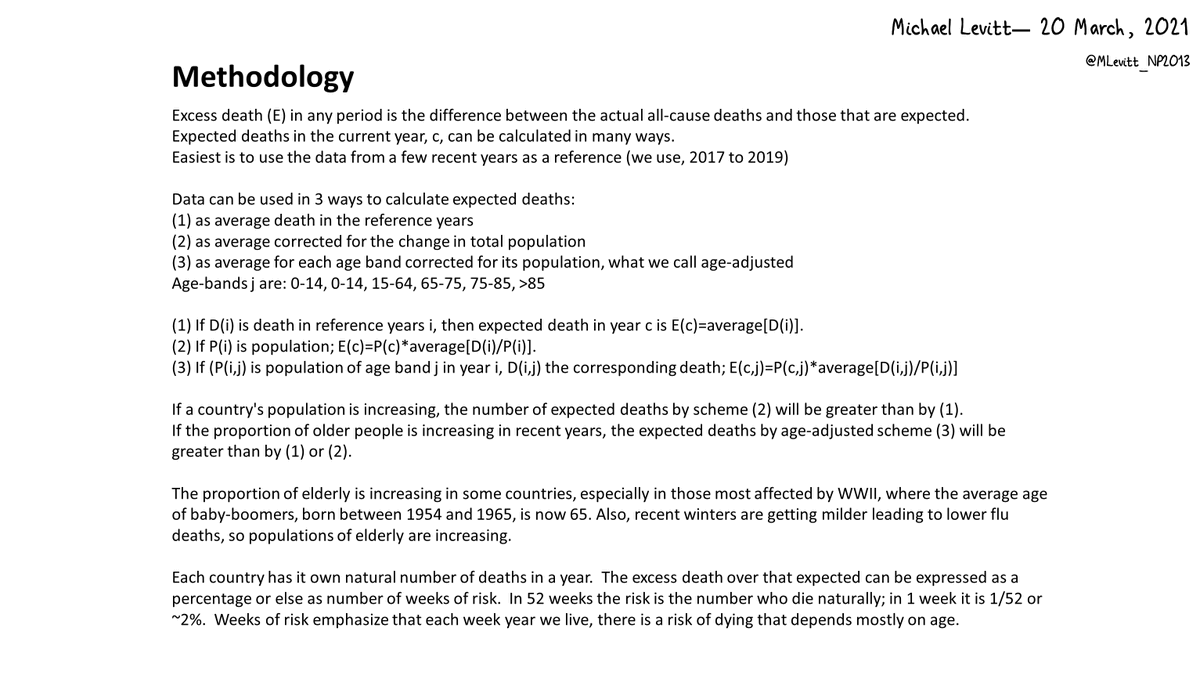
Fortunately age-adjusted excess death in Israel for the 75 weeks from 1-Jan-20 to 6-Jun-21 is almost as small as that in Sweden (<2% of natural death in 75 weeks)
Economic, social, medical & educational cost to Israel likely higher than to Sweden.
Does anyone have good data?
Economic, social, medical & educational cost to Israel likely higher than to Sweden.
Does anyone have good data?



Involved with Israel & Sweden since Mar-20, I add comparison of vaccination.
Both are now highly vaccinated, IL with Pfizer (mRNA), SE with AstraZeneca (Adenovirus DNA).
IL over 60% level 90 days earlier.
Should we worry SE has Delta wave ahead?
Is Pfizer == AstraZeneca?
Both are now highly vaccinated, IL with Pfizer (mRNA), SE with AstraZeneca (Adenovirus DNA).
IL over 60% level 90 days earlier.
Should we worry SE has Delta wave ahead?
Is Pfizer == AstraZeneca?




Thanks for clarification that Sweden is mostly Pfizer mRNA. I was lazy in looking it up.
Still, if vaccination patterns are so similar, do we expect a Swedish Delta Wave 90 days after Israel’s Delta Wave.
Nice Deltoid muscle joke.
Delta certainly is a catchy Greek letter.
Still, if vaccination patterns are so similar, do we expect a Swedish Delta Wave 90 days after Israel’s Delta Wave.
Nice Deltoid muscle joke.
Delta certainly is a catchy Greek letter.
• • •
Missing some Tweet in this thread? You can try to
force a refresh