1) Private Equity and Health Care Delivery by @brianwpowers @WillShrank @AmolNavathe
💯 Agree private equity isn't inherently good or bad "acts to amplify the response to extant financial incentives"
A couple of further points though....
ja.ma/3m6K6FU @JAMA_current
💯 Agree private equity isn't inherently good or bad "acts to amplify the response to extant financial incentives"
A couple of further points though....
ja.ma/3m6K6FU @JAMA_current
2) it's true that good policy can align private profit with public good, but if we are going to rely on that, need tight surveillance and fast response from regulators to close arbitrage opportunities where short-term profit maximizers will gather. c/f surprise billing
3/ if you wait too long, then entrenched profits become normalized, powerful incumbents are formed, and they can, and will, exert political influence to keep the "status quo" in place.
Many health policy examples (facility fees, drug pricing). But also...Medicare Advantage 👀
Many health policy examples (facility fees, drug pricing). But also...Medicare Advantage 👀
4/ It's true that fee for service creates a huge host of opportunities where private profit is not aligned with public good, in over-utilization where items aren't priced appropriately or restricted effectively...
PE rollups of derm practices -> MOHS surgery on the butt
PE rollups of derm practices -> MOHS surgery on the butt
5/ in creating monopolies where market power (or regulatory capture) can lead to higher prices (esp for commercial lives), like air ambulances, or anesthesiologists
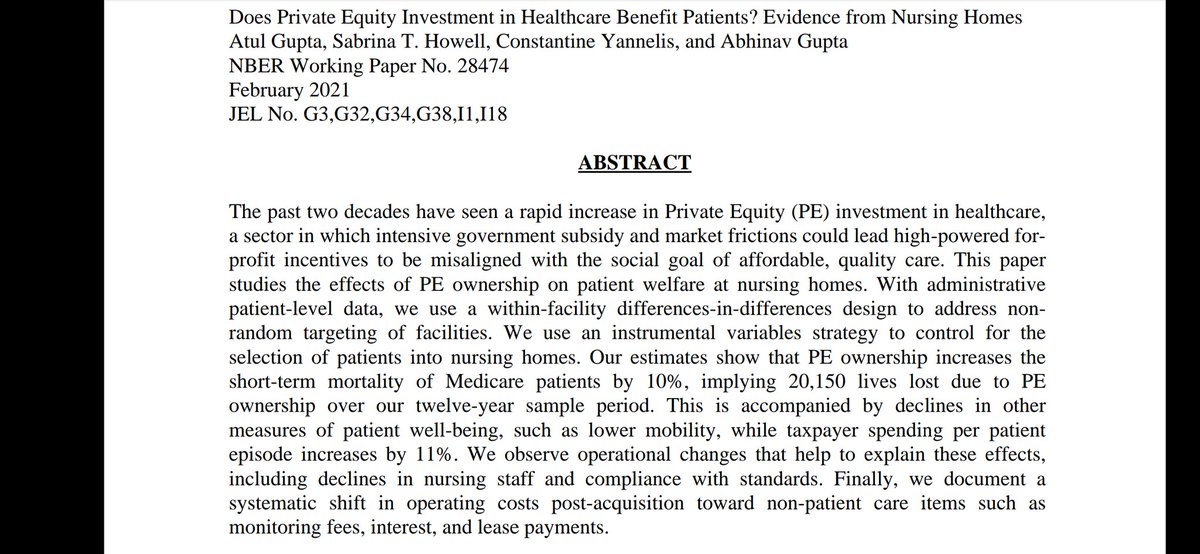
In cutting back on costs in ways that stint on care, harm patients (see nursing home study)
In cutting back on costs in ways that stint on care, harm patients (see nursing home study)
6/ I am a huge believer in value based payment model as a massive force for good in better aligning public good with private profits.
But that doesn't mean that arbitrage opportunities can't creep in there.
Like medicare advantage risk adjustment
But that doesn't mean that arbitrage opportunities can't creep in there.
Like medicare advantage risk adjustment
https://twitter.com/tricia_neuman/status/1367517691108601868?s=19
7/ I'm glad that @BrooksLaSureCMS @LizFowler_ @drmeenasesh vision for advancing value based care includes attention to risk adjustment
It's a tough problem, but when policymakers have tried to address it, barriers have been more political than technical. healthaffairs.org/do/10.1377/hbl…
It's a tough problem, but when policymakers have tried to address it, barriers have been more political than technical. healthaffairs.org/do/10.1377/hbl…
8/ so, YES.
We all benefit when the only capital to grow disruptive models doesn't have to come from today's incumbent giants, who are not interested in disrupting their current comfortable status.
We all benefit when the only capital to grow disruptive models doesn't have to come from today's incumbent giants, who are not interested in disrupting their current comfortable status.
9/ YES. There are long term-oriented PE firms that aren't just about cutting costs, or financial engineering, but rather around creating lasting positive change, in a way that's aligned with social good (if for no other reason that those businesses tend to be more sustainable)
10/ YES. Simplistic PE-bashing is misdiagnosing the problem, ("don't hate the player, hate the game")
Trying to limit their participation in healthcare seems difficult and potentially counter-intuitive
Trying to limit their participation in healthcare seems difficult and potentially counter-intuitive
11/ Policymakers that influence a significant portion of the incentives in the healthcare system have an awesome responsibility to always be on the lookout for emerging arbitrage being applied to any payment model, VBC as well as FFS, and to be constantly and quickly responding
12/ One of @N_Brennan unsung innovations at @CMSGov data unit was setting up an analytic function to track market developments and incentives
Maybe its a cat and mouse game, but that is the nature of life. There is no perfect solution that doesn't need constant attention.
Maybe its a cat and mouse game, but that is the nature of life. There is no perfect solution that doesn't need constant attention.
• • •
Missing some Tweet in this thread? You can try to
force a refresh