
1/ Like many others, I've been frustrated that we haven't seen the data behind the CDC's new recommendations. Parsing exact wording in transcripts is🤦
We're told there will be a release tomorrow but thanks to the @washingtonpost there's an internal CDC document to parse tonight
We're told there will be a release tomorrow but thanks to the @washingtonpost there's an internal CDC document to parse tonight

2/ The article by @yabutaleb7 @carolynyjohnson @JoelAchenbach is here:
washingtonpost.com/health/2021/07…
TY @bijans for spotting the "full pdf" download button.
washingtonpost.com/health/2021/07…
TY @bijans for spotting the "full pdf" download button.
3/ what do we learn?
The mysterious "other data" for high viral load in breakthrough cases came from a 4th of July outbreak in Provincetown (Barnstable, Mass) where the “vast majority” of the new cases were among fully vaccinated individuals
cc @zeynep
thehill.com/homenews/state…
The mysterious "other data" for high viral load in breakthrough cases came from a 4th of July outbreak in Provincetown (Barnstable, Mass) where the “vast majority” of the new cases were among fully vaccinated individuals
cc @zeynep
thehill.com/homenews/state…

4/ Based on @CDCDirector statement, I would assume that there was documented transmission from vaccinated to vaccinated in that outbreak.
I guess we always knew it *could* happen, but seeing it in real life must feel different
I guess we always knew it *could* happen, but seeing it in real life must feel different
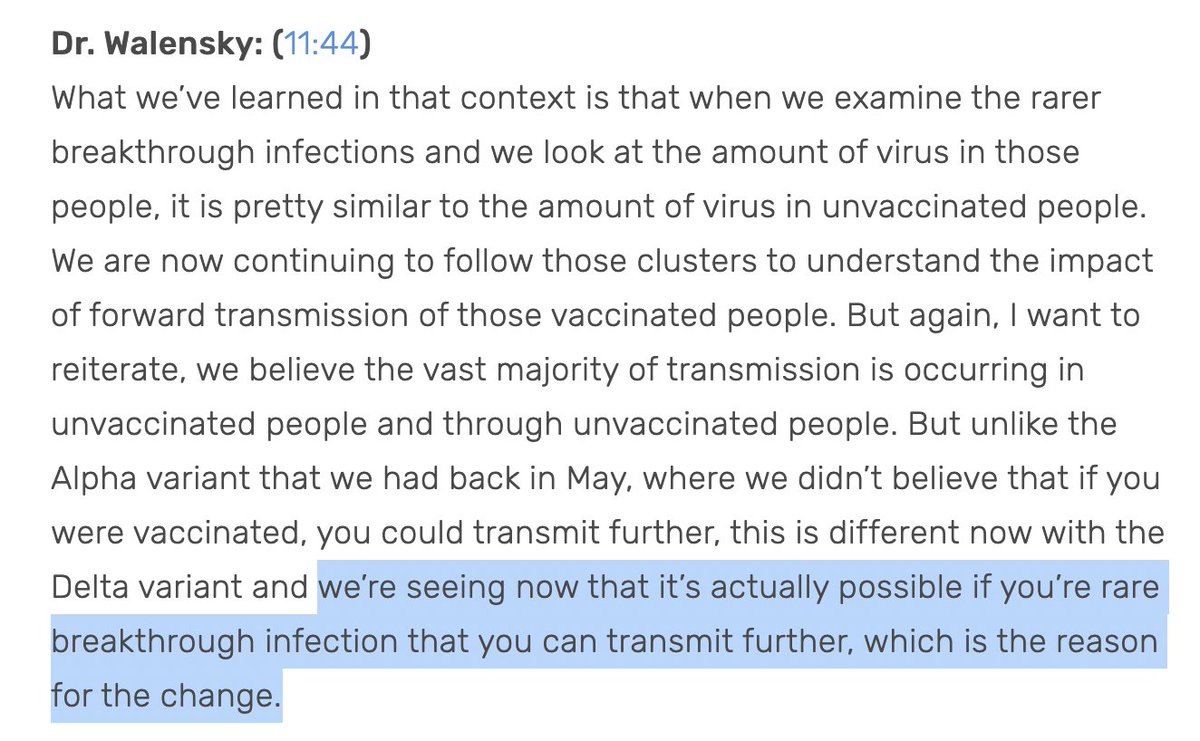
5/ here's a key data point that has NOT changed (which wasn't clear to me from the press conference)
IF a vaccinated person is infected, then yes, they have higher viral loads with delta.
But vaccination is still strongly protective against infection.
CDC estimates ~75-85%
IF a vaccinated person is infected, then yes, they have higher viral loads with delta.
But vaccination is still strongly protective against infection.
CDC estimates ~75-85%

6/ And there is almost no drop-off in efficacy of vaccine against hospitalization or death with Delta.
As more people are vaccinated, we will see higher proportion of hospitalized be vaccinated, but even those are concentrated among the immunosuppressed (44% vs 2% gen pop)
As more people are vaccinated, we will see higher proportion of hospitalized be vaccinated, but even those are concentrated among the immunosuppressed (44% vs 2% gen pop)
7/ So what leads to the new recommendation?
Modeling?
Here's the money slide. In case you didn't get it the first time, they helpfully add a red box alert
Let's break down what the analysis shows-
At diff levels of vaccine + natural immunity, what's prob of outbreak growing?
Modeling?
Here's the money slide. In case you didn't get it the first time, they helpfully add a red box alert
Let's break down what the analysis shows-
At diff levels of vaccine + natural immunity, what's prob of outbreak growing?


8/ The model assumptions alone are cool to see in black and white.
Masks prevent 40-60% of cases if worn by an infected person, and 20-30% effective at preventing inbound infections
~35% of population infected already (could be higher)
~60% vaccinated (dotted line)
(both?)
Masks prevent 40-60% of cases if worn by an infected person, and 20-30% effective at preventing inbound infections
~35% of population infected already (could be higher)
~60% vaccinated (dotted line)
(both?)
9/ Under these assumptions, with OG, even if no masking only a 20% probability that an outbreak would grow, while with delta, it's over 95% likely to grow
[Expressing results of modeling studies is hard, but I don't love this prob(increase) outcome. The extent of growth matters]
[Expressing results of modeling studies is hard, but I don't love this prob(increase) outcome. The extent of growth matters]
10/ The masking recommendation comes down to the lower right panel (not the highlighted one)
If unvaccinated adopt 100% masking, then 50% probability that outbreak would grow (at least until "natural immunity"+vacc rise higher)
But under universal masking wouldn't grow
maybe?
If unvaccinated adopt 100% masking, then 50% probability that outbreak would grow (at least until "natural immunity"+vacc rise higher)
But under universal masking wouldn't grow
maybe?


11/ Look, I'm not a professional modeler, but I've worked with some good ones.
(@SalomonJA @ambilinski and I wrote "Modeling Contact Tracing Strategies for COVID-19" jamanetwork.com/journals/jaman…)
They're tools for simplifying & understanding the world- not a magic 8 ball for policy
(@SalomonJA @ambilinski and I wrote "Modeling Contact Tracing Strategies for COVID-19" jamanetwork.com/journals/jaman…)
They're tools for simplifying & understanding the world- not a magic 8 ball for policy
12/ what is the masking policy switch? not what's in the model
In outbreak hotspots like Arkansas, politicians have literally outlawed masking requirements.
In Maryland, we are obsessing over whether all of our fully vaccinated staff need to mask if one person comes in from DC
In outbreak hotspots like Arkansas, politicians have literally outlawed masking requirements.
In Maryland, we are obsessing over whether all of our fully vaccinated staff need to mask if one person comes in from DC
13/ Universal masking is not a policy option that's actually available to us, especially where it's needed most.
And serial transmission among fully vaccinated IS REALLY UNLIKELY (even if it's possible).
If vaccine 80% protective, then Rt<1 among fully vaxxed, even for delta
And serial transmission among fully vaccinated IS REALLY UNLIKELY (even if it's possible).
If vaccine 80% protective, then Rt<1 among fully vaxxed, even for delta
14/ If fully vaccinated, not much has changed for me based on this new data.
I will follow all guidance & ordinances, but I'm still not a likely vector of spread
I'm still less likely to get it, and if not immunosuppressed, almost assured of protection against serious illness.
I will follow all guidance & ordinances, but I'm still not a likely vector of spread
I'm still less likely to get it, and if not immunosuppressed, almost assured of protection against serious illness.
15/ As the administration has been saying the most powerful thing we can do is to increase vaccination, and it's encouraging to see that trend happen during this latest surge, and for businesses to be encouraging or mandating vaccination among their workers
vaccines (still) work
vaccines (still) work
16/ I think the most trenchant analysis of the new CDC guidance is from @DrLeanaWen - it's not actually about the vaccinated.
"The CDC needs to make clear: The problem is the unvaccinated "
washingtonpost.com/opinions/2021/…
"The CDC needs to make clear: The problem is the unvaccinated "
washingtonpost.com/opinions/2021/…

• • •
Missing some Tweet in this thread? You can try to
force a refresh









