
1/ Comparison of Symptoms and RNA Levels in Children and Adults With SARS-CoV-2 Infection in the Community Setting
👉 @JAMAPediatrics paper comparing kids vs adults - most findings are as expected but good to see them confirmed in a large study… 🧵
👉jamanetwork.com/journals/jamap…
👉 @JAMAPediatrics paper comparing kids vs adults - most findings are as expected but good to see them confirmed in a large study… 🧵
👉jamanetwork.com/journals/jamap…
2/ This cross-sectional population-based survey included a convenience sample of 37,000 kids & adults in King County, Washington, who enrolled online for home self-collection of upper respiratory samples for SARS-CoV-2 testing from Mar-Nov 2020 

3/ 37,067 samples were tested & 673 (1.8%) were #sarscov2 positive (1.6% in adults, 3.4% in kids)
Most kids (80%) had a known SARS-CoV-2 +ve contact, & most contacts (68%) were in the same household
But only 41% of SARS-CoV-2 +ve adults (41.4%) reported any known +ve contact
Most kids (80%) had a known SARS-CoV-2 +ve contact, & most contacts (68%) were in the same household
But only 41% of SARS-CoV-2 +ve adults (41.4%) reported any known +ve contact
4/ Among 555 SARS-CoV-2–positive participants, 47/123 (38%) kids were asymptomatic vs 31/432 (7%) adults
Also, asymptomatic children were younger than symptomatic children (mean [SD] age, 6.2 [4.5] years vs 8.3 [5.7] years; P < .001)
👉younger kids less likely to have symptoms
Also, asymptomatic children were younger than symptomatic children (mean [SD] age, 6.2 [4.5] years vs 8.3 [5.7] years; P < .001)
👉younger kids less likely to have symptoms
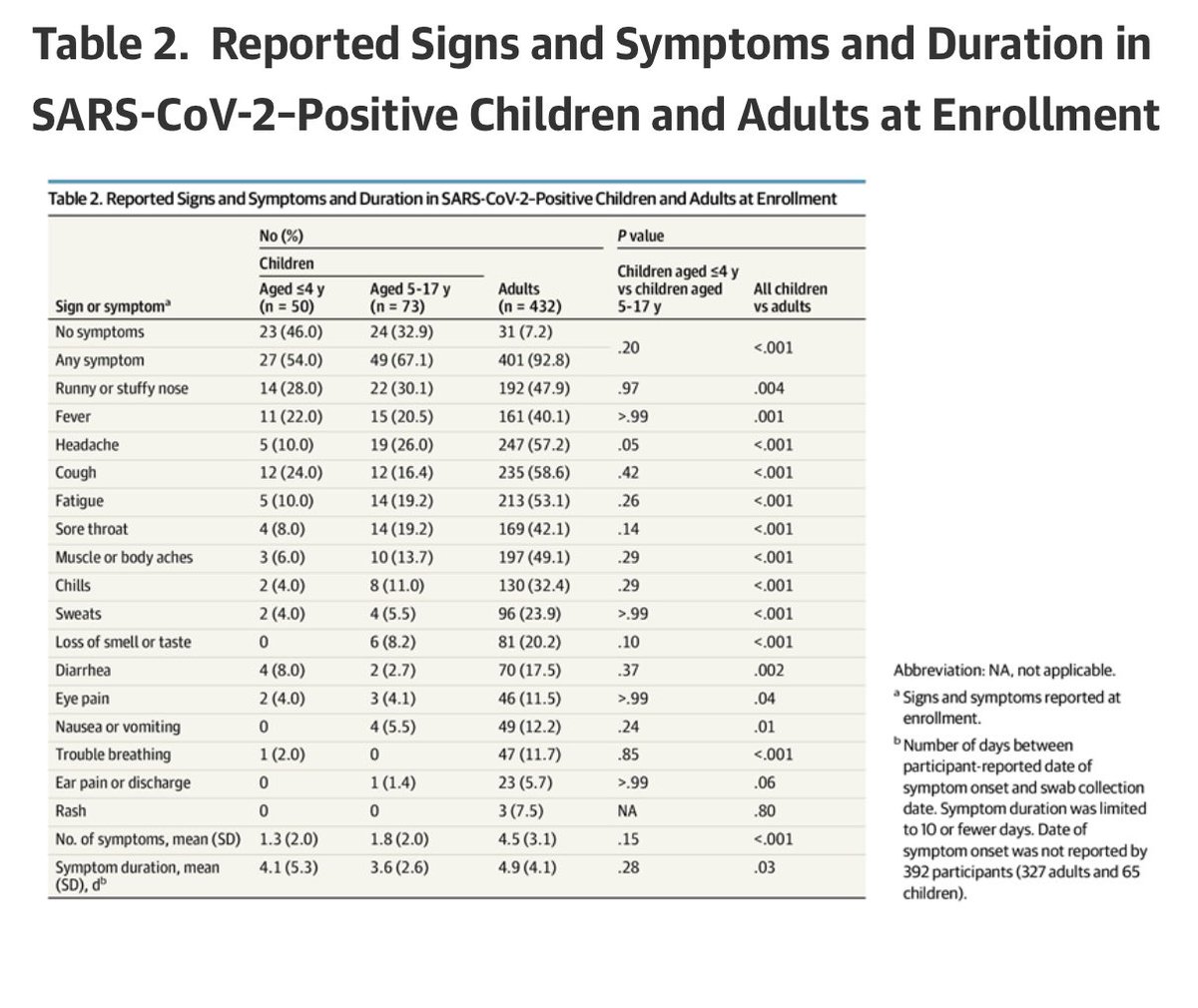
5/ When symptomatic, fewer symptoms were reported in kids vs adults
(mean number of symptoms [SD], 1.6 [2.0] vs 4.5 [3.1])
The duration of symptoms was also shorter in kids than in adults
(mean (SD) of 3.8 (3.8) days of symptoms vs 4.9 (4.1) days in symptomatic adults)
(mean number of symptoms [SD], 1.6 [2.0] vs 4.5 [3.1])
The duration of symptoms was also shorter in kids than in adults
(mean (SD) of 3.8 (3.8) days of symptoms vs 4.9 (4.1) days in symptomatic adults)

6/ The most common signs & symptoms in kids were runny or stuffy nose, fever, headache, and cough, while adults most frequently reported headache, cough, & fatigue
Note that this study was done before the Alpha or Delta variant was circulating in the US
Note that this study was done before the Alpha or Delta variant was circulating in the US

7/ Co-infection with other viruses was rare
Of 555 SARS-CoV-2 +ve swabs, 487 were tested for 24 respiratory pathogens by RT-PCR. Only 3/108 kids (2.8%) had another virus (2 rhinovirus, 1 adenovirus) vs 10/379 adults (2.6%): 7 rhinovirus, 1 adenovirus, 1 enterovirus, 1 influenza
Of 555 SARS-CoV-2 +ve swabs, 487 were tested for 24 respiratory pathogens by RT-PCR. Only 3/108 kids (2.8%) had another virus (2 rhinovirus, 1 adenovirus) vs 10/379 adults (2.6%): 7 rhinovirus, 1 adenovirus, 1 enterovirus, 1 influenza
8/ Symptomatic individuals had lower Ct values (corresponding to higher viral RNA levels) than asymptomatic individuals
Also, Ct values (virus levels) were not significantly different btwn symptomatic kids & symptomatic adults or between asymptomatic kids & asymptomatic adults
Also, Ct values (virus levels) were not significantly different btwn symptomatic kids & symptomatic adults or between asymptomatic kids & asymptomatic adults


9/ Accompanying editorial summarises findings & implications in detail
👉 Take home message: children were less frequently symptomatic, had fewer symptoms & shorter duration of symptoms vs adults - all likely to contribute to lower risk of transmission
👉jamanetwork.com/journals/jamap…
👉 Take home message: children were less frequently symptomatic, had fewer symptoms & shorter duration of symptoms vs adults - all likely to contribute to lower risk of transmission
👉jamanetwork.com/journals/jamap…
• • •
Missing some Tweet in this thread? You can try to
force a refresh








