
Vaccine effectiveness DOES NOT decline even after 6 months
Study from Sweden with wrong conclusions of “waning protection” against severe & symptomatic disease (see my annotations on the table)
Also illustrates the fallacy of observational studies
1/16
papers.ssrn.com/sol3/papers.cf…
Study from Sweden with wrong conclusions of “waning protection” against severe & symptomatic disease (see my annotations on the table)
Also illustrates the fallacy of observational studies
1/16
papers.ssrn.com/sol3/papers.cf…

The study looked at vaccinated and and vaccinated people in Sweden and looked at the event rates up to 9 months.
They calculated vaccine effectiveness at regular intervals until past six months. The authors conclude erroneously that vaccine effectiveness drops to (zero).
2/
They calculated vaccine effectiveness at regular intervals until past six months. The authors conclude erroneously that vaccine effectiveness drops to (zero).
2/
The traditional method of calculating effectiveness is to compare the outcomes in the vaccinated & vaccinated groups and see the percentage difference between the two.
Eg. If 10 events happen in the unvax group and only 1 event occurs in the vax group, effectiveness is 90%.
3/
Eg. If 10 events happen in the unvax group and only 1 event occurs in the vax group, effectiveness is 90%.
3/
However in the real world observational studies, we must remember that unvaccinated group also develops immunity as a result of asymptomatic or symptomatic natural infections.
As a result, the event rate in the unvaccinated population drops.
4/
As a result, the event rate in the unvaccinated population drops.
4/
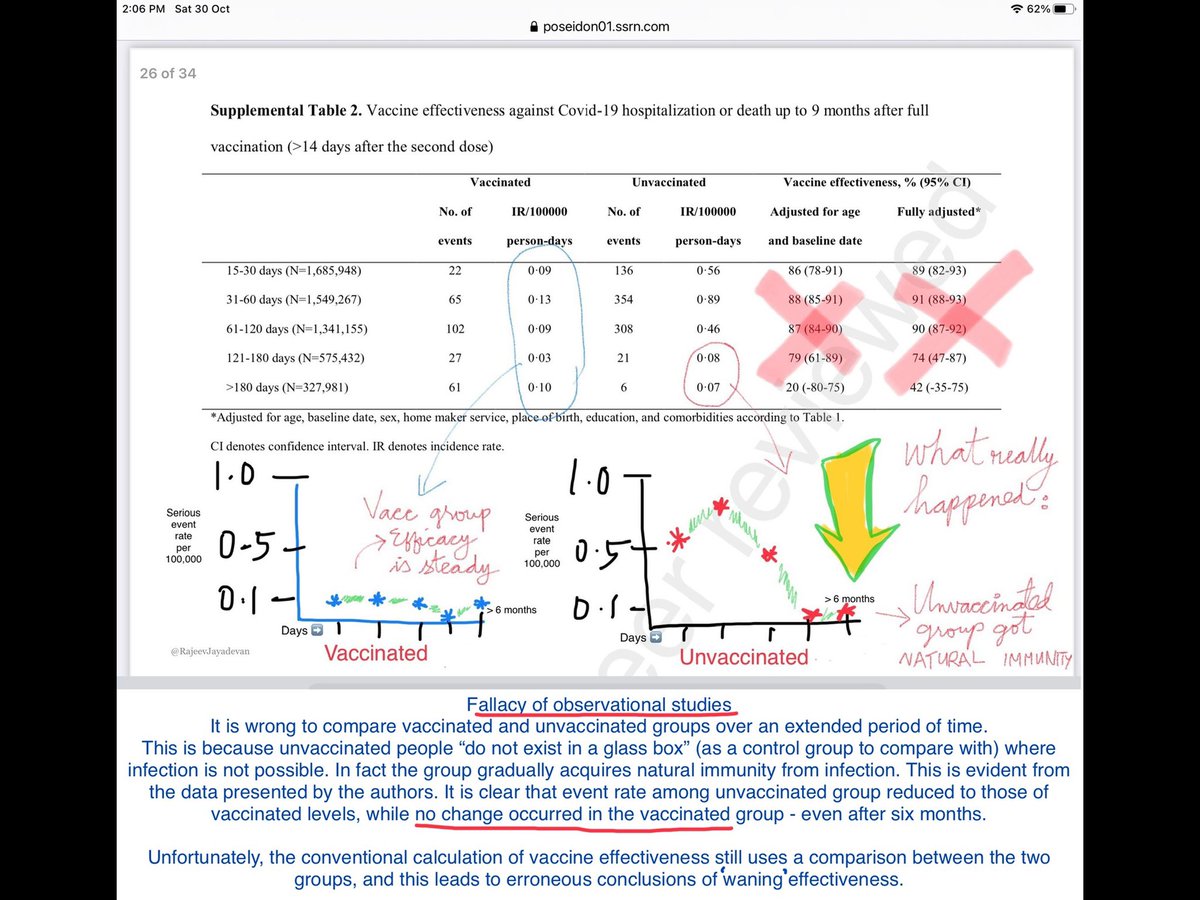
The authors of the paper have helpfully provided event rates over each time period, for each sub-group.
I used these event rates to plot a graph which I have linked below.
The graph of the vaccinated group (left, in blue) shows steady effectiveness even after six months.
5/16
I used these event rates to plot a graph which I have linked below.
The graph of the vaccinated group (left, in blue) shows steady effectiveness even after six months.
5/16
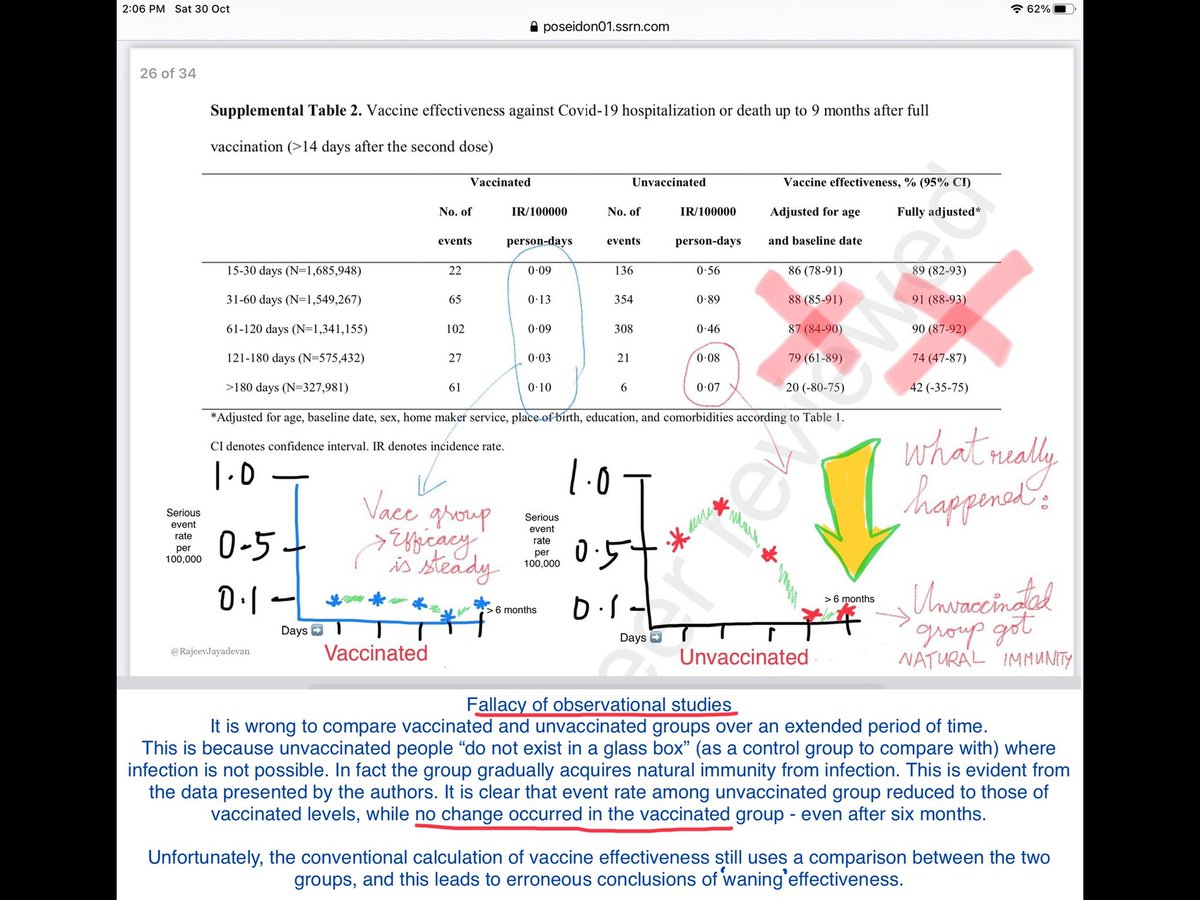
However the graph of the unvaccinated group (right, green) is interesting. It shows a relatively high event rate at the onset of the vaccination programme (when natural infections were few).
At about 4 months, we can see the rate drops to equal that of the vaccinated group.
6/
At about 4 months, we can see the rate drops to equal that of the vaccinated group.
6/

This decline in event rate is clearly the result of immunity brought about by natural infection.
Unfortunately, when we apply the traditional formula of effectiveness, this gets erroneously interpreted as a “decline in vaccine effectiveness to zero”.
Example 👇
7/
Unfortunately, when we apply the traditional formula of effectiveness, this gets erroneously interpreted as a “decline in vaccine effectiveness to zero”.
Example 👇
7/
To explain the fallacy, let me use an example.
Imagine that we are seated in a moving train. As we look to the left, there is another train on the next track, but moving at a slower speed. When we look at that train, we get a sense of our speed. But is that the right method?
8/
Imagine that we are seated in a moving train. As we look to the left, there is another train on the next track, but moving at a slower speed. When we look at that train, we get a sense of our speed. But is that the right method?
8/
Looking at the train on the parallel track is exactly how vaccine effectiveness is being presently calculated.
Unfortunately this assumes that the other train will continue to move at the same speed throughout the journey.
9/
Unfortunately this assumes that the other train will continue to move at the same speed throughout the journey.
9/
What we don’t take into account is that the other train could pick up speed, and this will affect our calculation about our own speed - that is if we continue to use this technique.
This is how vaccine effectiveness is commonly being calculated, including in this paper.
10/
This is how vaccine effectiveness is commonly being calculated, including in this paper.
10/
Now imagine that the next train picks up speed and is moving as fast as ours. As we look to the left, we may think that our train is not moving at all. We may conclude that our train has stopped moving. This is the erroneous conclusion of lack of effectiveness at six months.
11/
11/
What is the right method then?
What should be done is to look to the right -at stationary objects. If we did that from the beginning, we would know that our train has been moving at a steady speed right from the outset.
We realise there is no decline in our train’s speed.
12/
What should be done is to look to the right -at stationary objects. If we did that from the beginning, we would know that our train has been moving at a steady speed right from the outset.
We realise there is no decline in our train’s speed.
12/
The above fallacy is just one of the problems that occur with observational studies. While such studies are important, there are limitations.
Other limitations include variation in behaviour, testing rate, comorbidity and risk tolerance in between groups.
13/
Other limitations include variation in behaviour, testing rate, comorbidity and risk tolerance in between groups.
13/
It is important to look out for any real decline in protection from severe disease & death. We believe this protection is long-term because of memory cells, which continuously improve over time, through affinity maturation, somatic hypermutation and antibody class switch.
14/
14/
In the real world, natural infection may act as natural boosters of immunity, in both vaccinated & unvaccinated people. Recent data have shown that breakthrough infections induce anamnestic response.
This however does not mean that people should seek out such opportunities.
15/
This however does not mean that people should seek out such opportunities.
15/
Looking at the data presented by the the Swedish paper, it appears that the two populations (vax and unvax) are finally reaching a level ground - at approximately six months - when the event rates (per 100,000 person days) appear to be equalising.
16/16
16/16


@doctorsoumya @celinegounder @drbabukv @AnuragAgrawalMD @profvrr @ProfSomashekhar @docraviw @jayalal10 @IMAIndiaOrg @JeremyFarrar
Fallacy of observational studies
See thread above 👆 for context
Fallacy of observational studies
See thread above 👆 for context
@threadreaderapp please unroll
Vaccine protection from hospitalisation/death by age >80 & <80, over about 9 months. No decline seen in protection.
On the other hand, event rates in the unvaccinated group start dropping past 2 months, approximating the vaccine group from 4 months onwards.
see thread above👆
On the other hand, event rates in the unvaccinated group start dropping past 2 months, approximating the vaccine group from 4 months onwards.
see thread above👆

Although it is not advisable to “actively seek” a breakthrough infection, this is pertinent and realistic information for the future.
https://twitter.com/rajeevjayadevan/status/1453960339356143625
• • •
Missing some Tweet in this thread? You can try to
force a refresh







