
1. Sorry I had to delete the important thread I just put up as I said "consistent underestimation of the proportion of the population vaccinated" when it should have been "consistent underestimation of the proportion of the population UNVACCINATED". Here is the correct version .
2. Our ongoing analysis of the ONS Nov 1 Deaths by Vacc Status Report is showing consistent underestimation of the proportion of the population unvaccinated. Example: Look at this plot of mortality rate for non-Covid deaths (age category 60-69) during the summer weeks... 
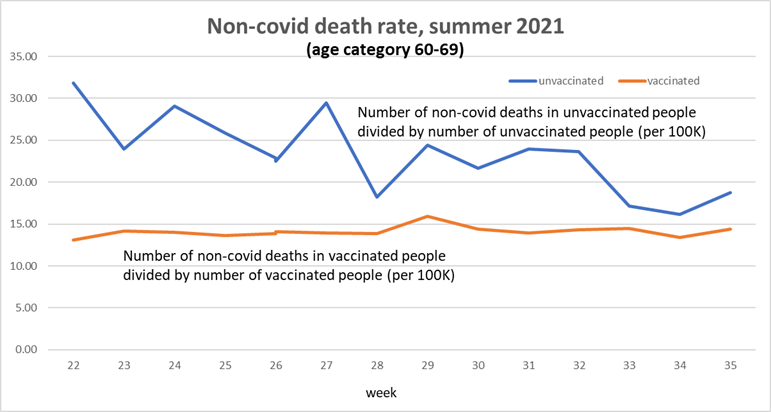
3. The fact the mortality rates for vacced and unvacced are so different makes no sense. Assuming the vacc is doing no harm, these plots should be similar. Only reasonable possible explanation is that the proportion of the population unvaccinated is underestimated.
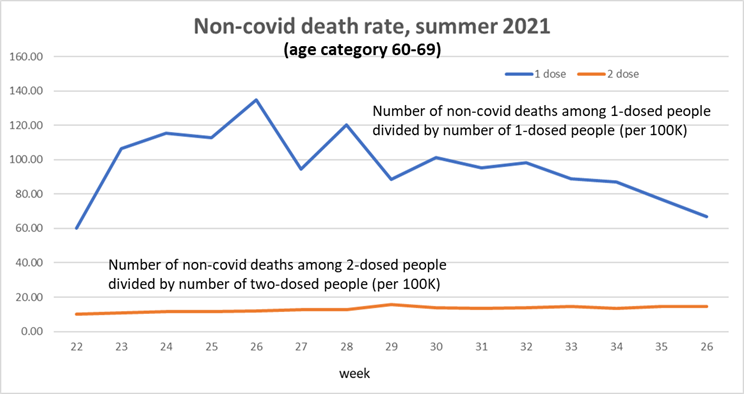
4. And there are also problems in the population estimates of different categories of vaccinated as this plot shows (mortality rate for single dosed up to 10 times higher than double dosed)
4. And there are also problems in the population estimates of different categories of vaccinated as this plot shows (mortality rate for single dosed up to 10 times higher than double dosed)

5. Our report will show these problems are systemic, which means that none of the reported mortality rates (age adjusted or not) can be trusted. The reported all cause mortality rates for unvaccinated are too high, while mortality rates for vaccinated are too low
• • •
Missing some Tweet in this thread? You can try to
force a refresh



