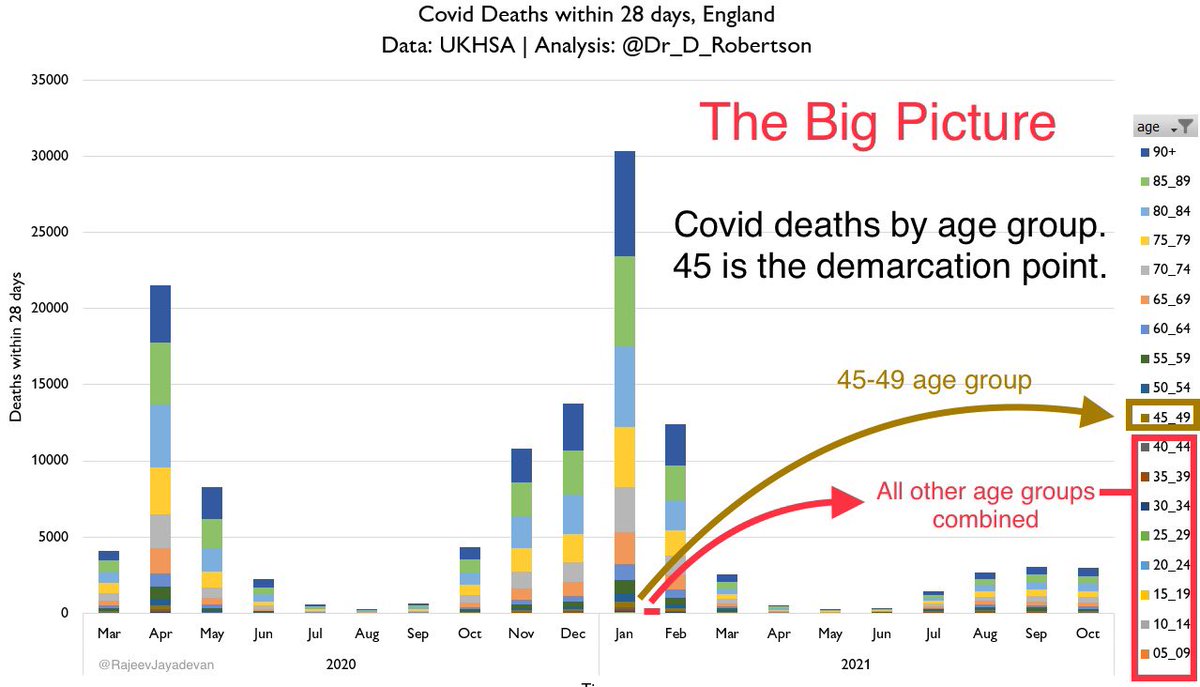
The most powerful graph that I have seen of the pandemic.
This calls for a rethink of vaccination strategy.
Note the sharp demarcation around age 40-45.
Vaccination of this 40+ segment needs priority.
Below that age, it could even be made optional. Here’s why👇
(Thread)
This calls for a rethink of vaccination strategy.
Note the sharp demarcation around age 40-45.
Vaccination of this 40+ segment needs priority.
Below that age, it could even be made optional. Here’s why👇
(Thread)
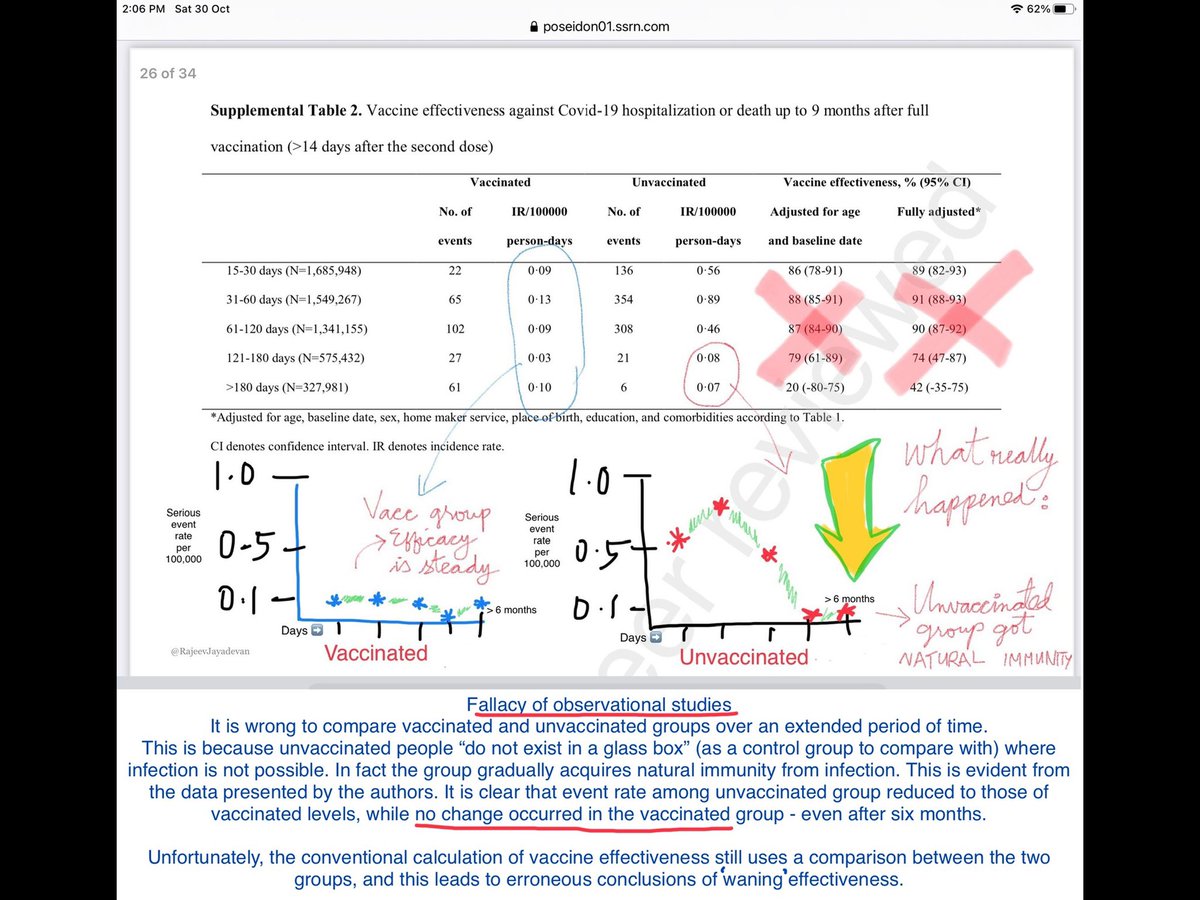
Although vaccines were launched with a hope of stopping transmission and further waves, we have seen that high % vaccination coverage does not stop subsequent waves. This is because they are ineffective in providing mucosal immunity; virus is silently spreading in communities.
2/
2/
At the same time, we have found that vaccines are not 100% benign products as is often suggested by certain academics.
They have failed to acknowledge the small but significant number of serious and fatal outcomes is that occurred - particularly among younger individuals.
3/
They have failed to acknowledge the small but significant number of serious and fatal outcomes is that occurred - particularly among younger individuals.
3/
There has been a clear attempt to downplay the risks, under various guises. Using statistics to trivialise success, and attributing complications to other causes. Families who suffered these complications have been ignored, and have understandably felt cheated by the system.
4/
4/
Before I go on to discuss the merits of vaccines as of today, let me take a moment to state the solemn fact that for a family who suffered death as a result of vaccination, it is NOT trivial.
For the academics who push mandates, they might just be a statistic.
5/
For the academics who push mandates, they might just be a statistic.
5/
One can argue that a “small %” of deaths & complications are “acceptable”, but we must never forget that for the family who lost a loved one, it is always a 100%. For those who are left with a deficit, it is a 100%.
This does not mean that vaccines are ineffective products.
6/
This does not mean that vaccines are ineffective products.
6/
Published data of such adverse outcomes will invariably undercount/underestimate these risks, simply because it is impossible “prove” that the event was caused by vaccine.
I recall writing about reinfections last year & being ridiculed that “it was impossible” as “no proof”
7/
I recall writing about reinfections last year & being ridiculed that “it was impossible” as “no proof”
7/
“Proof” is a curtain behind which it is easy to hide. When many of us reported reinfection, they asked us for peer reviewed publication. A peer reviewed complication was not possible because genomic sequences needed to be done in both instances - which is next to impossible.
8/
8/
Thus, reinfections, though common, were ignored; this led to an impression that immunity against this virus was the sterilising type.
Absence of proof is not proof of absence.
This fit the vaccine narrative that it was possible to “vaccinate our way out of the pandemic”.
9/
Absence of proof is not proof of absence.
This fit the vaccine narrative that it was possible to “vaccinate our way out of the pandemic”.
9/
After the vaccines were launched, in the initial months, infections were few; this led to a false sense of security. This was from high level of Antibody lasting ~3 months.
Some nations decided to discard all other precautions, claiming that they “conquered the pandemic”.
10/
Some nations decided to discard all other precautions, claiming that they “conquered the pandemic”.
10/
At the same time, reports of adverse outcomes from vaccines came in, most of which were crushed claiming “lack of proof”. Academics where afraid to admit this, claiming that it will ‘fuel vaccine hesitancy’. A good no. of these were indeed spurious (incidental) associations.
11/
11/
As the publications finally came in, it was clear that a very small no. of individuals did have serious complications, some of which were fatal.
This is not to state that vaccines should not be given, but that they must be treated on the same platform as other medications.
12/
This is not to state that vaccines should not be given, but that they must be treated on the same platform as other medications.
12/
All medical interventions have their share of side effects, for instance antibiotics, painkillers, surgeries, general anaesthesia, CT scans, chemotherapy.
In fact it is unscientific to claim or suggest that adverse outcomes do not happen, or to misrepresent the numbers.
13/
In fact it is unscientific to claim or suggest that adverse outcomes do not happen, or to misrepresent the numbers.
13/
Now is the time to put all the facts on the table.
Which include:
1. Vaccines are effective at preventing deaths
2. Vaccines are not very effective at preventing infections or spread
3. Deaths do not occur equally at all ages
4. Serious outcomes occur, but are very rare
14/
Which include:
1. Vaccines are effective at preventing deaths
2. Vaccines are not very effective at preventing infections or spread
3. Deaths do not occur equally at all ages
4. Serious outcomes occur, but are very rare
14/

5. Certain serious vaccine related outcomes are disproportionately seen among younger age groups, who are by default at the lowest risk of mortality from COVID-19, see graph above.
The following revisions may be considered to existing strategies, in view of the above facts.
15/
The following revisions may be considered to existing strategies, in view of the above facts.
15/
1. Vaccination must be prioritised for older adults- particularly those above 40.
2. Two doses are necessary to generate sufficient protection against severe disease and death
3. Among those who had prior infection, one dose will suffice.
16/
2. Two doses are necessary to generate sufficient protection against severe disease and death
3. Among those who had prior infection, one dose will suffice.
16/
4. Among people under 40, greater emphasis on non-pharmaceutical interventions will result in lower spread of virus.
This can (and must) be done without compromising livelihood.
17/
This can (and must) be done without compromising livelihood.
17/
5. Among younger people, vaccination can be even made optional, with emphasis for people who are at greater risk of either exposure, or for developing complications because they have a significant medical condition. Forcing people to take vaccines is not acceptable anymore.
18/
18/
The reason is that beyond the initial few months, vaccines are ineffective at preventing transmission - regardless of what the “blind proponents” continue to say.
We have seen that in countless outbreaks around the world that occurred among fully vaccinated individuals.
19/
We have seen that in countless outbreaks around the world that occurred among fully vaccinated individuals.
19/
Vaccines, as I have written many months ago, function effectively like a helmet ⛑
Helmets do not prevent accidents; but in the event of an accident, they improve one’s chance of survival.
Now let’s look at the helmet at analogy in three contexts.
20/
Helmets do not prevent accidents; but in the event of an accident, they improve one’s chance of survival.
Now let’s look at the helmet at analogy in three contexts.
20/
If we look at the road, the people who need the helmet the most are the two wheeler riders.
They are at greatest risk of dying - because they fall at a high speed.
They definitely need a helmet; ignoring this recommendation puts them at great peril.
21/
They are at greatest risk of dying - because they fall at a high speed.
They definitely need a helmet; ignoring this recommendation puts them at great peril.
21/
The next level of risk will be the cyclists, but they fall at a lower speed and are at lower risk of death. While helmets are definitely recommended, we see many cyclists choosing not to wear them.
The decision to wear or not can be left to the individual or while racing.
22/
The decision to wear or not can be left to the individual or while racing.
22/
The third level are pedestrians. Theoretically, they can also fall by tripping on a pavement or a banana peel. If they were wearing a helmet, yes - they are less likely to die from that fall.
But do pedestrians really need to wear a helmet expecting to take a fall?
23/
But do pedestrians really need to wear a helmet expecting to take a fall?
23/
In the above metaphor, people over 40 represents two wheeler riders, young adults are the cyclists and children are the pedestrians.
I am aware that this yes contrary to many recommendations but it is time that we started thinking in this direction.
24/
I am aware that this yes contrary to many recommendations but it is time that we started thinking in this direction.
24/
Why? Because this pandemic is not going away, reinfections & breakthrough infections will continue to occur, we need to prioritise those who are likely to develop bad outcomes.
Risk benefit analysis is not the same for all age groups. It is time we acknowledged that.
25/25
Risk benefit analysis is not the same for all age groups. It is time we acknowledged that.
25/25
*peer reviewed publication
*trivialise risks
*optional/voluntary is the implied meaning
• • •
Missing some Tweet in this thread? You can try to
force a refresh