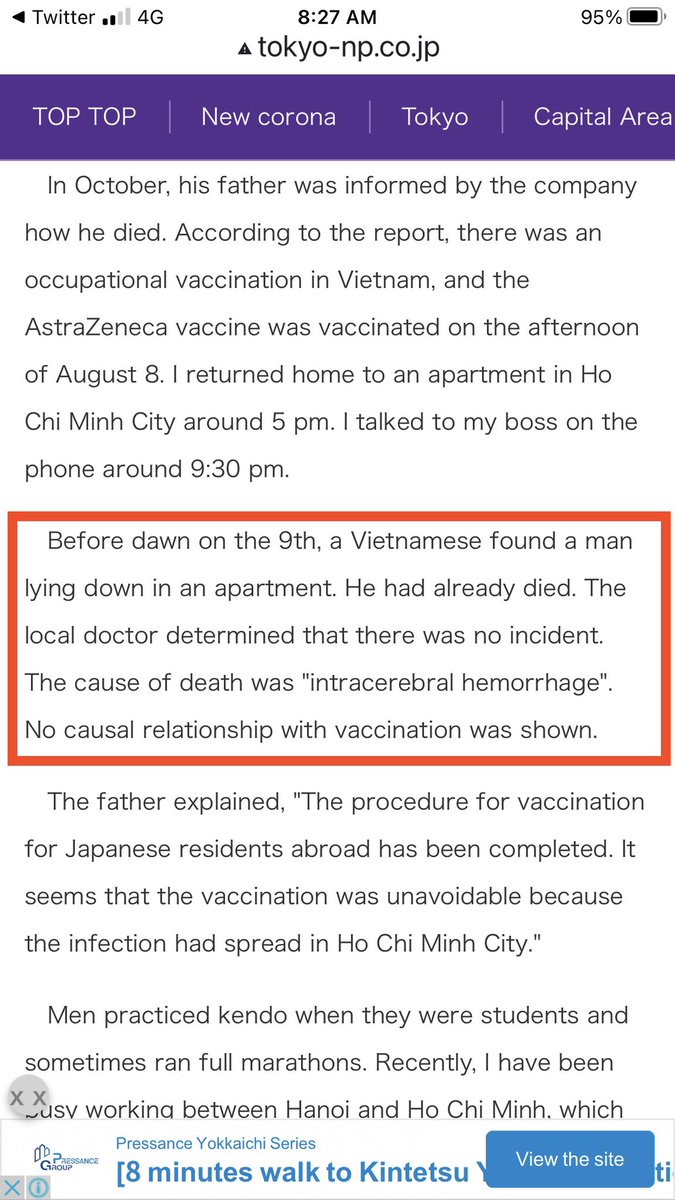
The pain of a father who lost his son following vaccination.
There is no doubt a trend to deny such deaths for “lack of proof”
Rare. But these are the hidden casualties.
Article shared by a Japanese doctor.
Unfortunately, talking about the downside of vaccination is taboo.
There is no doubt a trend to deny such deaths for “lack of proof”
Rare. But these are the hidden casualties.
Article shared by a Japanese doctor.
Unfortunately, talking about the downside of vaccination is taboo.
https://twitter.com/mph_for_doctors/status/1462970900093931524


Talking of the adverse outcomes following vaccination is not the same as “anti vaxx”
In fact, denying downsides by hiding behind the heavy curtains of “proof” is unscientific.
Most medical interventions have downsides. And not everyone has the same risk tolerance.
2/
In fact, denying downsides by hiding behind the heavy curtains of “proof” is unscientific.
Most medical interventions have downsides. And not everyone has the same risk tolerance.
2/
Ridiculing those who are reluctant to vaccinate is a trend in the west.
Can’t agree with that.
There are people who are afraid to fly, despite knowing that flights are safer than driving. No one ridicules them. At least I don’t.
3/
Can’t agree with that.
There are people who are afraid to fly, despite knowing that flights are safer than driving. No one ridicules them. At least I don’t.
3/
If someone close to us had a bad outcome after chemotherapy, it is natural for us to feel that it is dangerous. The same holds for all interventions.
If someone is afraid to vaccinate, it is important to talk with them with respect and interest, without looking down at them.
4/
If someone is afraid to vaccinate, it is important to talk with them with respect and interest, without looking down at them.
4/
If after hearing the facts they won’t change their mind, it is unfair and plain wrong to call them “loonies” or other such derogatory terms.
A few others deliberately plot against all public health measures, often with a motive to sell unproven “remedies” to make a profit.
5/
A few others deliberately plot against all public health measures, often with a motive to sell unproven “remedies” to make a profit.
5/
That is the section that must be called out as unscientific.
Knowingly or otherwise, they generate big profits for magic remedy (snake oil) sellers. Such sellers exist in every country. They often cite abstract sources to back up their own claim of ‘conspiracies’.
6/
Knowingly or otherwise, they generate big profits for magic remedy (snake oil) sellers. Such sellers exist in every country. They often cite abstract sources to back up their own claim of ‘conspiracies’.
6/
I have noticed that doctors are often “afraid” to acknowledge that vaccination can rarely cause serious complications.
I don’t understand why; because the ethics of a doctor is to explain ALL aspects of disease and treatment to patients and to society, and help them decide.
7/
I don’t understand why; because the ethics of a doctor is to explain ALL aspects of disease and treatment to patients and to society, and help them decide.
7/
If doctors start being “one-sided”, to deny that treatments have downsides, ridicule those who ask questions, fail to communicate openly, then in the long run that will erode public trust.
Bottom line:
Vaccination is one of the proven tools to control the pandemic.
8/
Bottom line:
Vaccination is one of the proven tools to control the pandemic.
8/
But vaccination alone is not going to control it.
Depending on vaccination alone is like sitting on a chair with one leg, ignoring the other 3 legs.
1. Improving room ventilation
2. Avoiding indoor gatherings
3. Wearing masks appropriate for the setting
9/
Depending on vaccination alone is like sitting on a chair with one leg, ignoring the other 3 legs.
1. Improving room ventilation
2. Avoiding indoor gatherings
3. Wearing masks appropriate for the setting
9/
In any society, there will be a few individuals who have a different risk perception as mentioned above.
But with sincere efforts, vaccine hesitancy can be kept low.
In Kerala, vaccine acceptance is over 97%.
That’s from honest, transparent, respectful communication.
10/10
But with sincere efforts, vaccine hesitancy can be kept low.
In Kerala, vaccine acceptance is over 97%.
That’s from honest, transparent, respectful communication.
10/10
• • •
Missing some Tweet in this thread? You can try to
force a refresh