Two doses of vaccine generate long-lived and stable Memory T cells.
The longevity of immune response to SARS-CoV2 virus depends on the presence and stability of memory cells of the B & T genre.
This is a landmark paper from Rome by Guerrera et al.
1/
science.org/doi/10.1126/sc…
The longevity of immune response to SARS-CoV2 virus depends on the presence and stability of memory cells of the B & T genre.
This is a landmark paper from Rome by Guerrera et al.
1/
science.org/doi/10.1126/sc…
The presence of long lived memory B cells had previously been established in several papers, see my tweets. This paper focuses on memory T cells in response to 2 doses of mRNA vaccine.
I will discuss some basic immunology first, to help understand the context of this paper.
2/
I will discuss some basic immunology first, to help understand the context of this paper.
2/
Following the innate response, the adaptive immulogical response to a virus infection is basically two pronged.
The two arms are T cells and B cells.
B cells make antibodies which work like security guards OUTSIDE our gate, preventing the thief from entering the premises.
3/
The two arms are T cells and B cells.
B cells make antibodies which work like security guards OUTSIDE our gate, preventing the thief from entering the premises.
3/
However once the thief enters the premises (metaphor for entry into cell), we absolutely need the T cells to detect and destroy the infected cells. (As antibodies can’t enter cells).
This is the chief method of stopping FURTHER spread in the body, and to limit organ damage.
4/
This is the chief method of stopping FURTHER spread in the body, and to limit organ damage.
4/
T cells come in different genres. Effector T cells are the policemen that search & destroy infected cells. These are active after vaccination or after natural infection. This is the reason why people who are vaccinated or had past natural infection survive the next infection.
5/
5/
Memory T cells belong to 3 types: central memory (also called T stem cell memory cells), effector memory cells and tissue resident memory cells (TRM). These three types have different roles.
These are the cells that remain long term after “immune contraction”.
6/
These are the cells that remain long term after “immune contraction”.
6/
“Immune contraction” is the natural down-shifting of our immune response AFTER we get rid of the initial infection or vaccine.
This is because there is no need for a continuous active immune response AFTER the enemy has been defeated.
However a “memory file” is essential.
7/
This is because there is no need for a continuous active immune response AFTER the enemy has been defeated.
However a “memory file” is essential.
7/
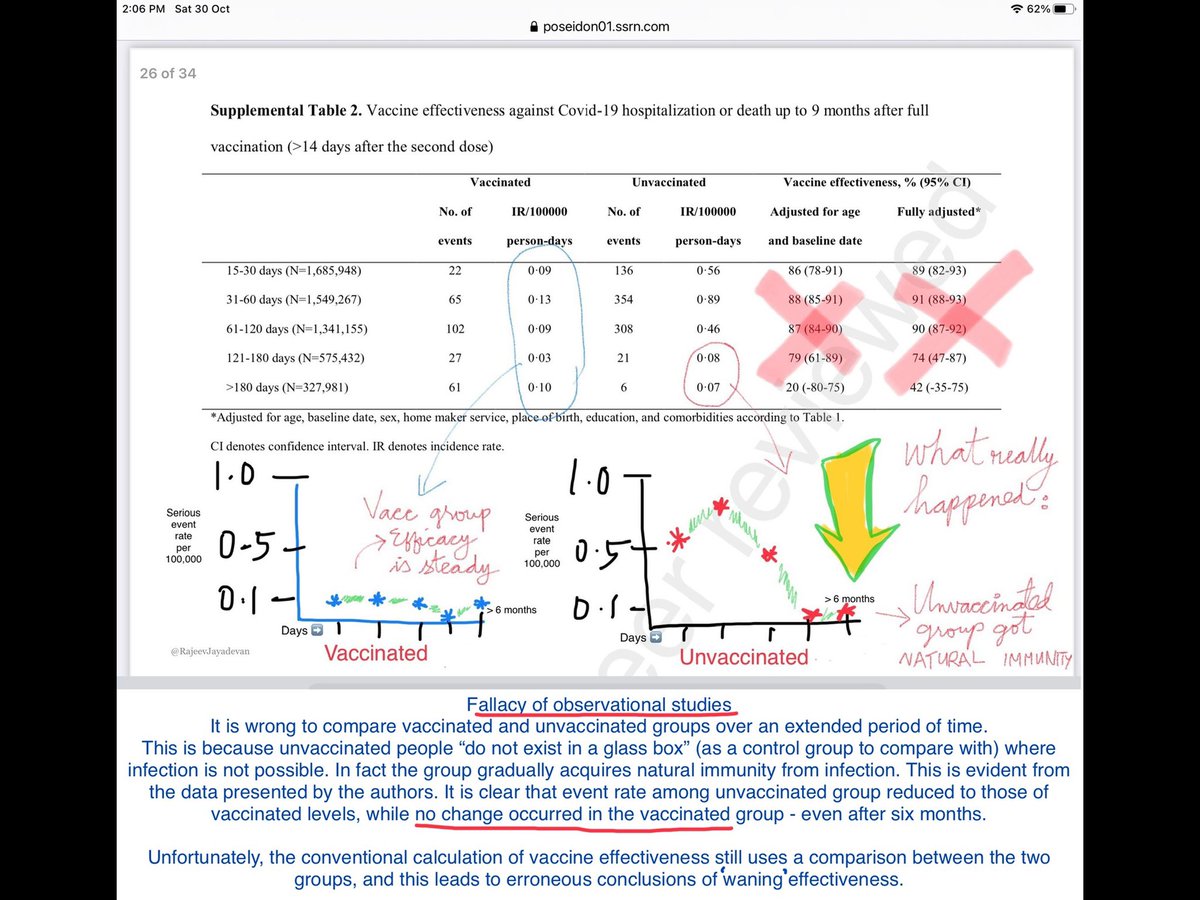
As part of this “immune contraction”, total antibody levels will fall to a low baseline - after about 3 months, when plasmablasts disappear.
This however has been widely mis-interpreted as “waning” and “failure of immune response”.
8/
This however has been widely mis-interpreted as “waning” and “failure of immune response”.
8/
The high circulating antibody levels during these initial few months naturally reduce the chance of another infection by the same virus.
This can be compared to a temporary “immediate shield” as the authors state in the paper. As they decline, breakthrough infections occur.
9/
This can be compared to a temporary “immediate shield” as the authors state in the paper. As they decline, breakthrough infections occur.
9/
The reason why the body should not continuously be in “immunological overdrive” (that is, persistently high antibody levels and immune cells patrolling) is because it can generate its own complications, such as chronic autoimmune disease.
10/
10/
The authors monitored the T-cell memory cells among 71 individuals who received two doses of Pfizer vaccine.
They found long-lasting CD4+ and CD8+ T-SCM, (T-stem cell memory) which were stable throughout the 6-month period of this study.
This is good news.
11/
They found long-lasting CD4+ and CD8+ T-SCM, (T-stem cell memory) which were stable throughout the 6-month period of this study.
This is good news.
11/
TSCM cells provide a memory reservoir with multipotent capacity, and have been shown to persist for decades.
The authors write:
“The detection of TSCM in vaccinated individuals is thus suggestive of the establishment of long-lived immunity”.
12/
The authors write:
“The detection of TSCM in vaccinated individuals is thus suggestive of the establishment of long-lived immunity”.
12/
“The number of TSCM induced after priming predicted future T cell responses, and the stability of this memory population may point in the direction of durable immunity against SARS-CoV2”
13/
13/
In summary, this proves that 2 doses of (mRNA) vaccine generate not only long lived B cell memory, but also long lived T-cell memory response with poly-functionality; providing the ability to prevent organ damage if & when subsequent infections of SARS-CoV2 virus occur.
14/14
14/14
• • •
Missing some Tweet in this thread? You can try to
force a refresh