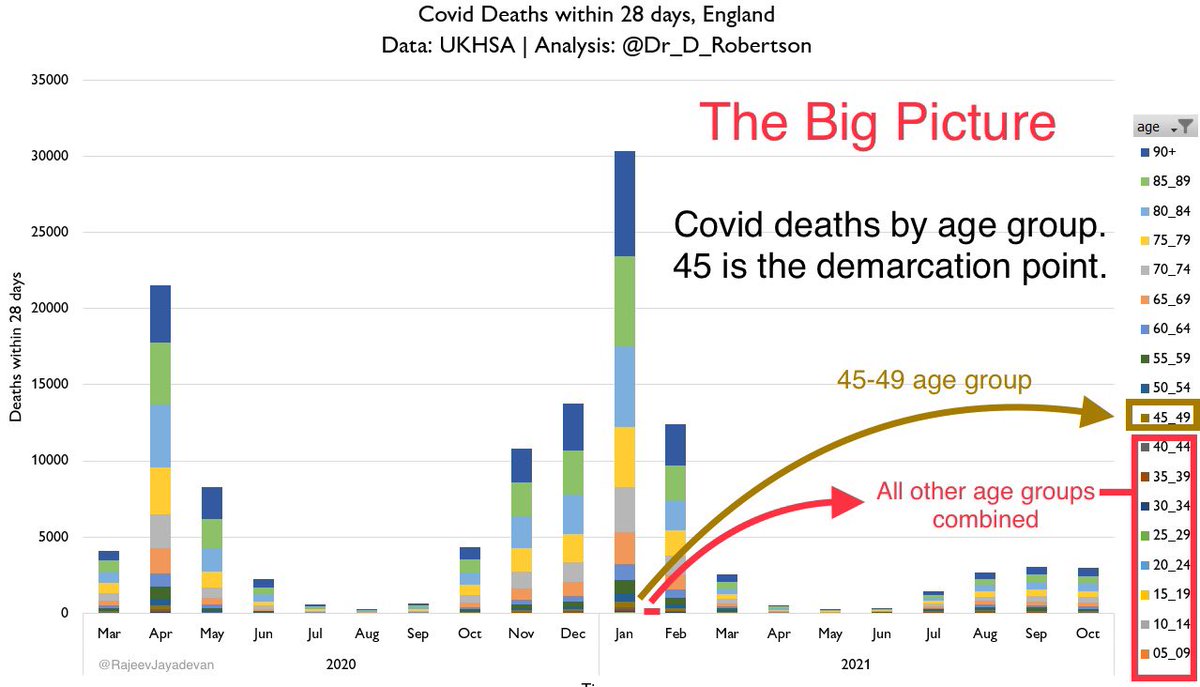
No decline in real world effectiveness of vaccine against death & hospitalisation. Graphs are drawn from Minnesota data.
I have used a ratio of event rates among unvaccinated : vaccinated population. The graphs show death & hospitalisation rates.
1/5
health.state.mn.us/diseases/coron…
I have used a ratio of event rates among unvaccinated : vaccinated population. The graphs show death & hospitalisation rates.
1/5
health.state.mn.us/diseases/coron…




The ratios are based on vaccination % prevailing 30 days prior to each data point, so that it reflects the true effect of vaccination.
It must also be kept in mind that the vaccinated segment by default are older, more likely to fall sick and have serious outcomes.
2/
It must also be kept in mind that the vaccinated segment by default are older, more likely to fall sick and have serious outcomes.
2/
This implies that the ratios are an underestimate of the true protection offered by vaccines.
In other words, we are not comparing groups of equal health status when we do a ratio of the unvaccinated and vaccinated.
The true protection will be larger.
3/
In other words, we are not comparing groups of equal health status when we do a ratio of the unvaccinated and vaccinated.
The true protection will be larger.
3/
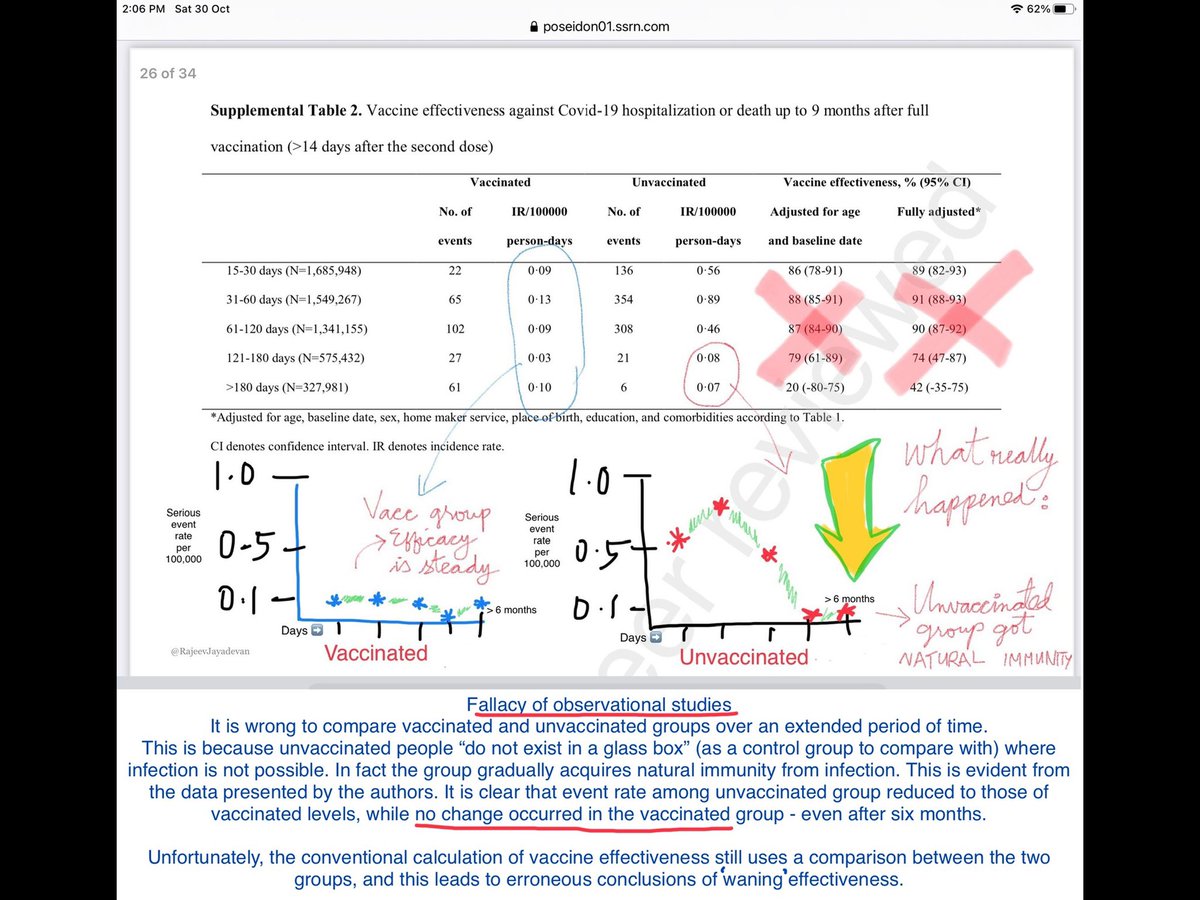
We must also factor in the “parallel immunisation process” that occurs in the unvaccinated group - on account of their picking up immunity due to asymptomatic and symptomatic natural infections.
This will eventually be reflected in their event rates in subsequent months.
4/
This will eventually be reflected in their event rates in subsequent months.
4/
A similar trend was observed in Oregon, I had tweeted earlier on the event rates, and the ratio remained consistently at around 2.8.
Obviously real-world effectiveness studies have their limitations, but these are state-reported data and probably the most reliable.
5/5
Obviously real-world effectiveness studies have their limitations, but these are state-reported data and probably the most reliable.
5/5
• • •
Missing some Tweet in this thread? You can try to
force a refresh