Myocarditis with mRNA vaccine.
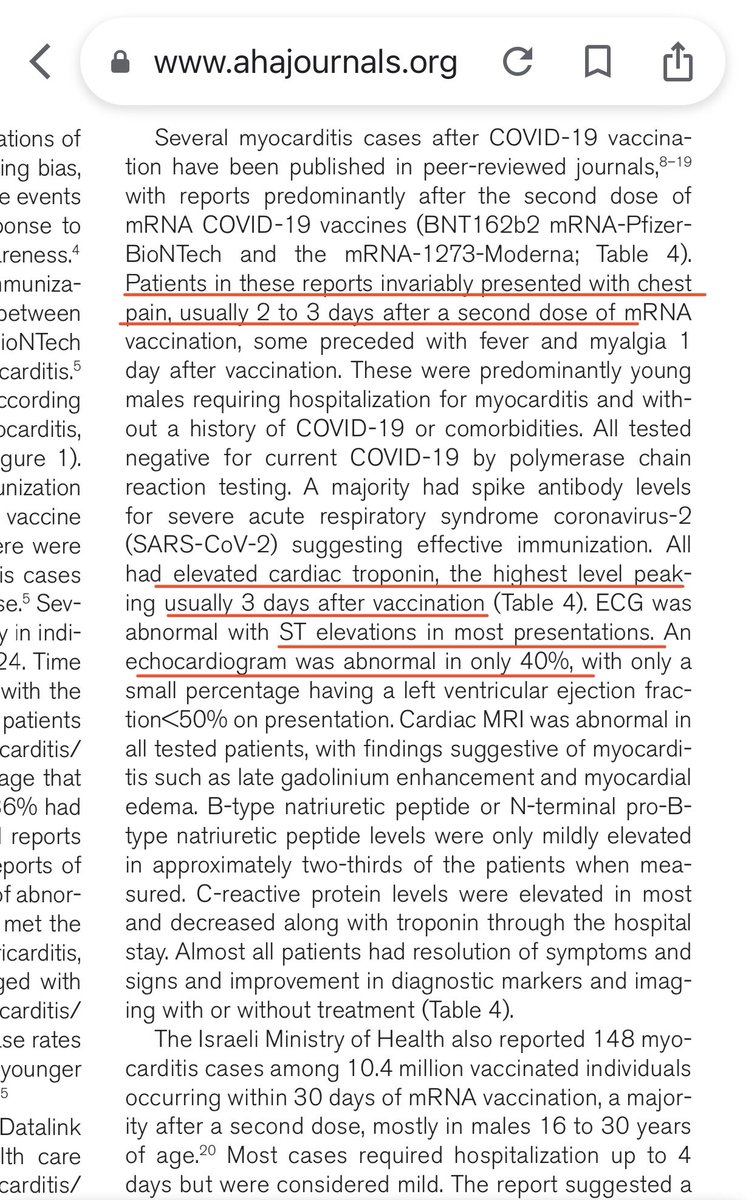
“Patients invariably had chest pain” is a misleading statement.
It is more like “In all REPORTED cases of myocarditis, chest pain was present”
Note myocarditis need not cause chest pain, hence not all patients will seek medical attention.
1/
“Patients invariably had chest pain” is a misleading statement.
It is more like “In all REPORTED cases of myocarditis, chest pain was present”
Note myocarditis need not cause chest pain, hence not all patients will seek medical attention.
1/

The diagnostic criteria of “myocarditis” are given below.
However, patients are more likely to notice chest pain than other symptoms. Hence these people get diagnosed, (and reported).
Chest pain is more likely in those who ALSO have PERICARDITIS.
2/
ahajournals.org/doi/pdf/10.116…
However, patients are more likely to notice chest pain than other symptoms. Hence these people get diagnosed, (and reported).
Chest pain is more likely in those who ALSO have PERICARDITIS.
2/
ahajournals.org/doi/pdf/10.116…


Myocarditis can occur with other symptoms like palpitations, shortness of breath or may not cause overt symptoms.
Myocarditis might only cause ECG or ECHO cardiogram abnormalities or isolated elevation in cardiac enzymes like Troponin.
This means we could be missing cases.
3/
Myocarditis might only cause ECG or ECHO cardiogram abnormalities or isolated elevation in cardiac enzymes like Troponin.
This means we could be missing cases.
3/
Thus, it is possible that isolated myocarditis - that is without accompanying pericarditis - might not always be detected.
Note: pericarditis is inflammation of the membrane covering the heart, which is a painful condition. Hence it is more likely to get attention.
4/
Note: pericarditis is inflammation of the membrane covering the heart, which is a painful condition. Hence it is more likely to get attention.
4/
Without doing “routine” cardiac tests on all people the true number of cardiac side-effects cannot be determined. It is perhaps not feasible to check cardiac tests in a million people.
Why not? Because these events occur in about 130 per million young males (published rate).
5/
Why not? Because these events occur in about 130 per million young males (published rate).
5/
This means that the reported cases of myocarditis is by default an underestimation.
It is only based on those who develop and report chest pain.
The true number is unknown.
We also know that the higher the dose of vaccine used, the greater the incidence of myocarditis.
6/
It is only based on those who develop and report chest pain.
The true number is unknown.
We also know that the higher the dose of vaccine used, the greater the incidence of myocarditis.
6/
For instance, Moderna (100 mcg) has higher incidence than Pfizer (30 mcg).
This suggests that the condition might be dose-related.
Early reports on myocarditis after boosters indicate that the risk is lower by about 2-fold in the young male subgroup.
7/
This suggests that the condition might be dose-related.
Early reports on myocarditis after boosters indicate that the risk is lower by about 2-fold in the young male subgroup.
7/
About dose of vaccine and myocarditis, thanks @Alexander_Tin
see thread above👆 for context
see thread above👆 for context
https://twitter.com/alexander_tin/status/1463585854614609921
• • •
Missing some Tweet in this thread? You can try to
force a refresh