Should we all get a vaccine booster (3rd dose)?
New preprint w @billy_gardner_ , we examine impact of 3rd doses on key topic: transmission.
medrxiv.org/content/10.110…
tl;dr 3rd dose could significantly reduce Rt & stop some surges, but doses should 1st go to unvaccinated if possible
New preprint w @billy_gardner_ , we examine impact of 3rd doses on key topic: transmission.
medrxiv.org/content/10.110…
tl;dr 3rd dose could significantly reduce Rt & stop some surges, but doses should 1st go to unvaccinated if possible

Background
COVID-19 vaccines are fantastic. Better than we could have imagined. mRNA vaccines had efficacy of ~95% for symptomatic disease & even better for severe disease & death. But there's now strong evidence that protection against mild disease & infection is waning a bit.
COVID-19 vaccines are fantastic. Better than we could have imagined. mRNA vaccines had efficacy of ~95% for symptomatic disease & even better for severe disease & death. But there's now strong evidence that protection against mild disease & infection is waning a bit.

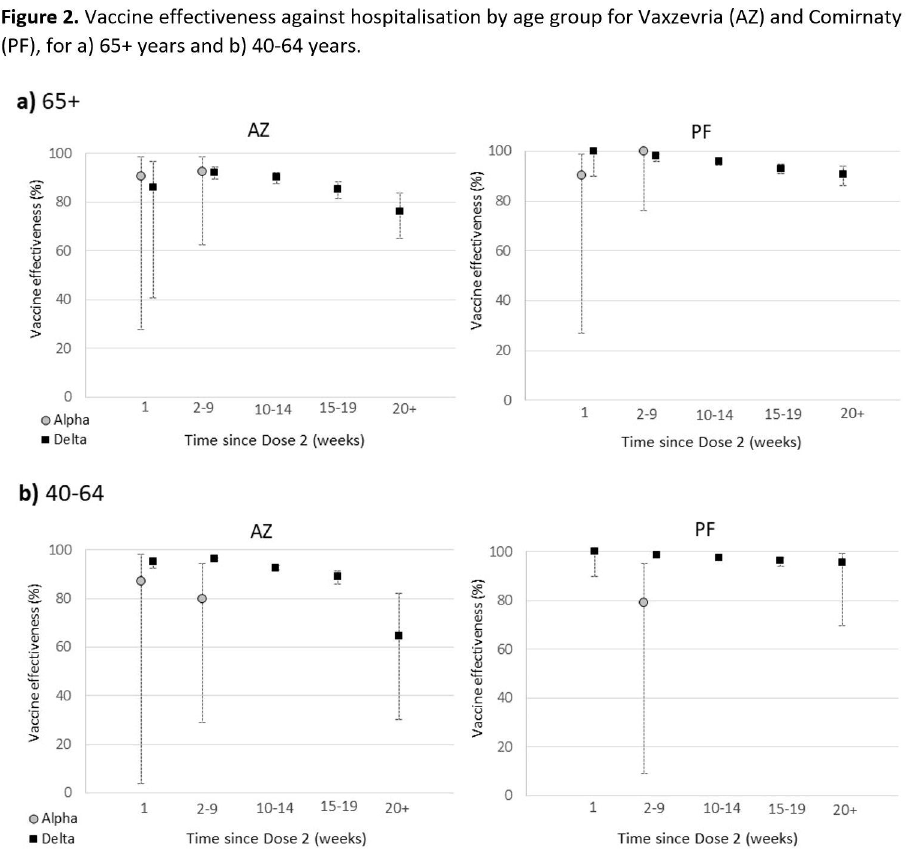
Here's one study from the UK (there are many others) showing a reduction for Pfizer &Astrazeneca.
doi.org/10.1101/2021.0…
doi.org/10.1101/2021.0…
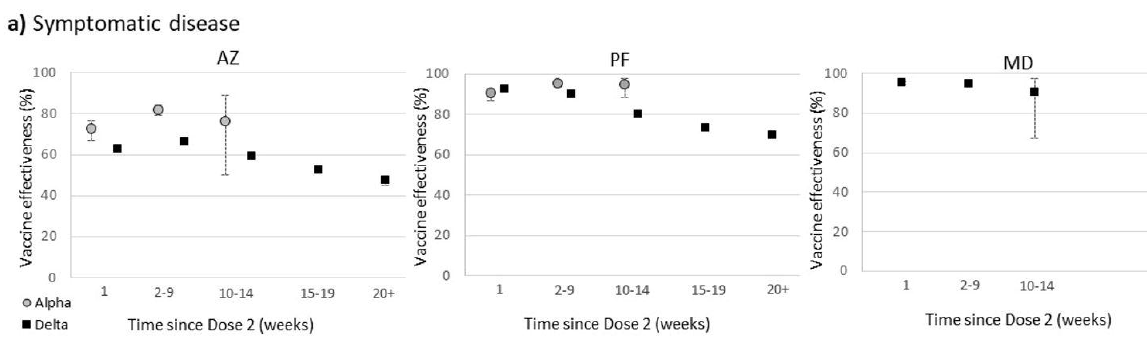
Thankfully, waning of protection against severe disease has been much less. Here's a thread reviewing many studies that show this:
Fig from same paper as above (doi.org/10.1101/2021.0…) shows slight waning but still very high protection.
https://twitter.com/mugecevik/status/1430218372348878860
Fig from same paper as above (doi.org/10.1101/2021.0…) shows slight waning but still very high protection.
So why all the talk about the need for vaccine boosters?
Why did Biden say we'd all get vaccine boosters after 6 months? Why did FDA & CDC recommend them for 65+, underlying medical conditions & those in high risk settings (cdc.gov/coronavirus/20…).
A couple reasons.
Why did Biden say we'd all get vaccine boosters after 6 months? Why did FDA & CDC recommend them for 65+, underlying medical conditions & those in high risk settings (cdc.gov/coronavirus/20…).
A couple reasons.
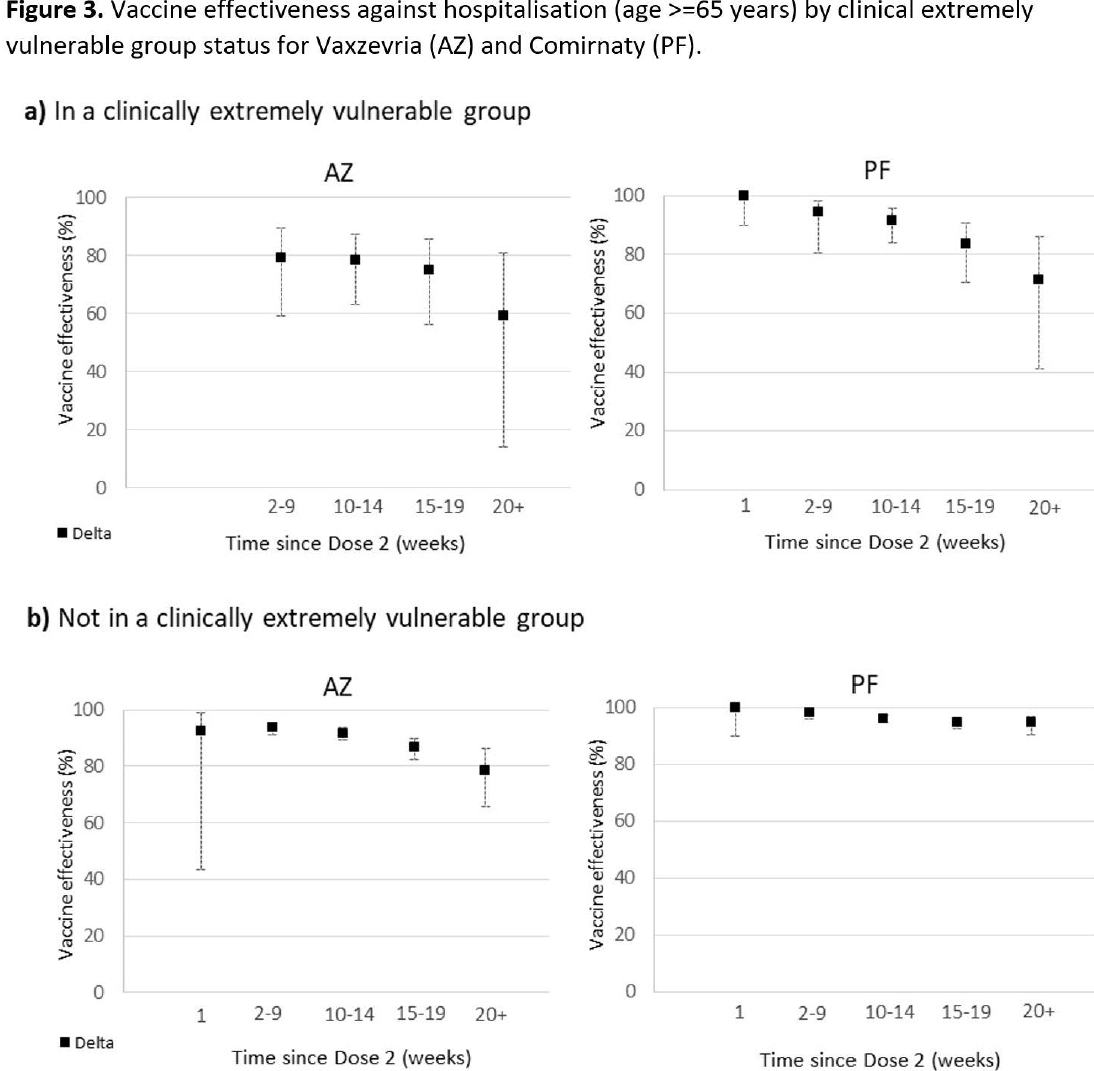
First, there is plenty of evidence that protection, even against severe disease, has waned more in older and ill individuals. e.g.
doi.org/10.1101/2021.0…
doi.org/10.1101/2021.0…
Second, even mild COVID-19 disease may have long-term consequences. #LongCovid, although the frequency & severity of LongCovid cases in vaccinated individuals that get mild infections is still uncertain.
Regardless, this means protection against even mild disease is important.
Regardless, this means protection against even mild disease is important.
So why is there pushback against vaccine boosters? Recent article @apoorva_nyc: some MDs aren't as supportive of boosters as broad recent CDC recommendations.
nytimes.com/2021/10/25/hea…
nytimes.com/2021/10/25/hea…
Two big reasons:
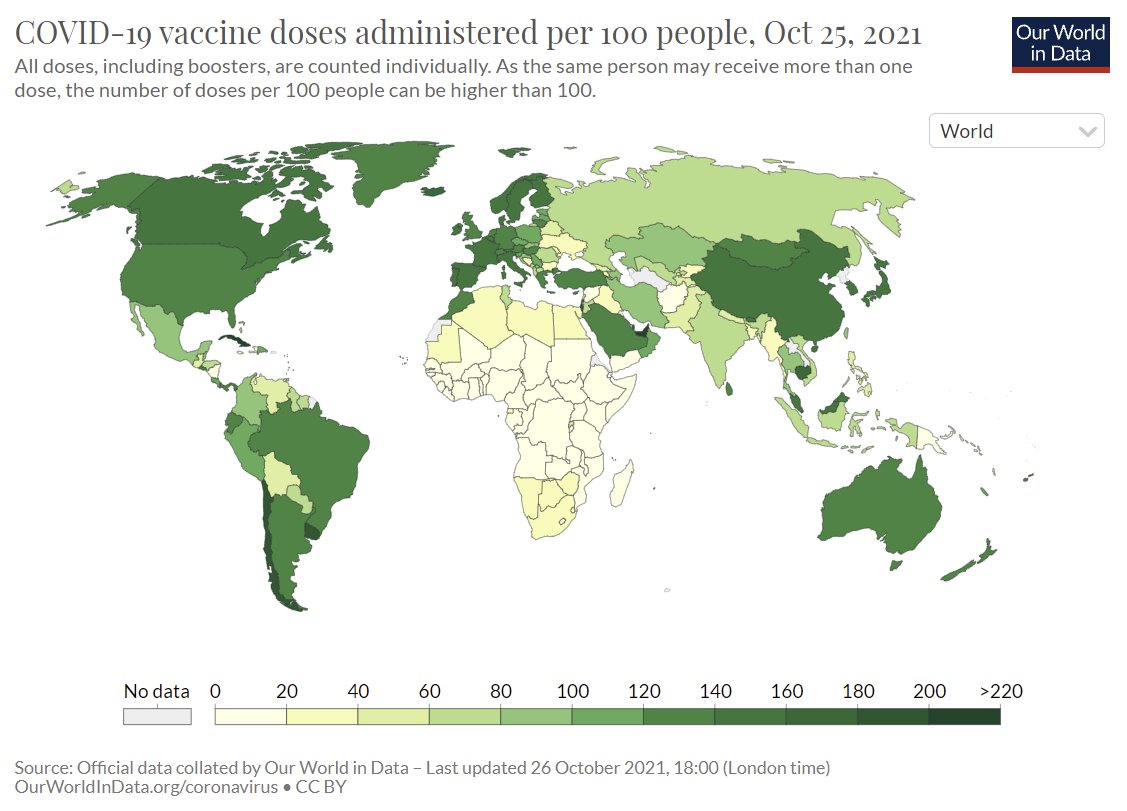
1) Global vaccine equity: Many populations, especially in Africa, have received no vaccines, so boosting protection a little in rich countries, while millions have no protection is morally wrong.
2) Recommending boosters could reduce confidence in vaccines.
1) Global vaccine equity: Many populations, especially in Africa, have received no vaccines, so boosting protection a little in rich countries, while millions have no protection is morally wrong.
2) Recommending boosters could reduce confidence in vaccines.
I'm a strong supporter of vaccine equity & COVAX (who.int/initiatives/ac…) & I'd bet almost 100% of epidemiologists (including me) would prefer to give doses to unvaccinated before giving boosters.
However, if sufficient doses were available, a very important question is: what would the impact of boosters be on transmission of SARS-CoV-2? Could boosters reduce transmission enough to prevent a winter surge? That's the Q our paper addresses.
To do so, we had to estimate vaccine protection against against all infections & transmission with waning & boosting. The data to do so directly don't yet exist.
However, early paper showed antibody titers predict protection v disease.
doi.org/10.1038/s41591…
However, early paper showed antibody titers predict protection v disease.
doi.org/10.1038/s41591…
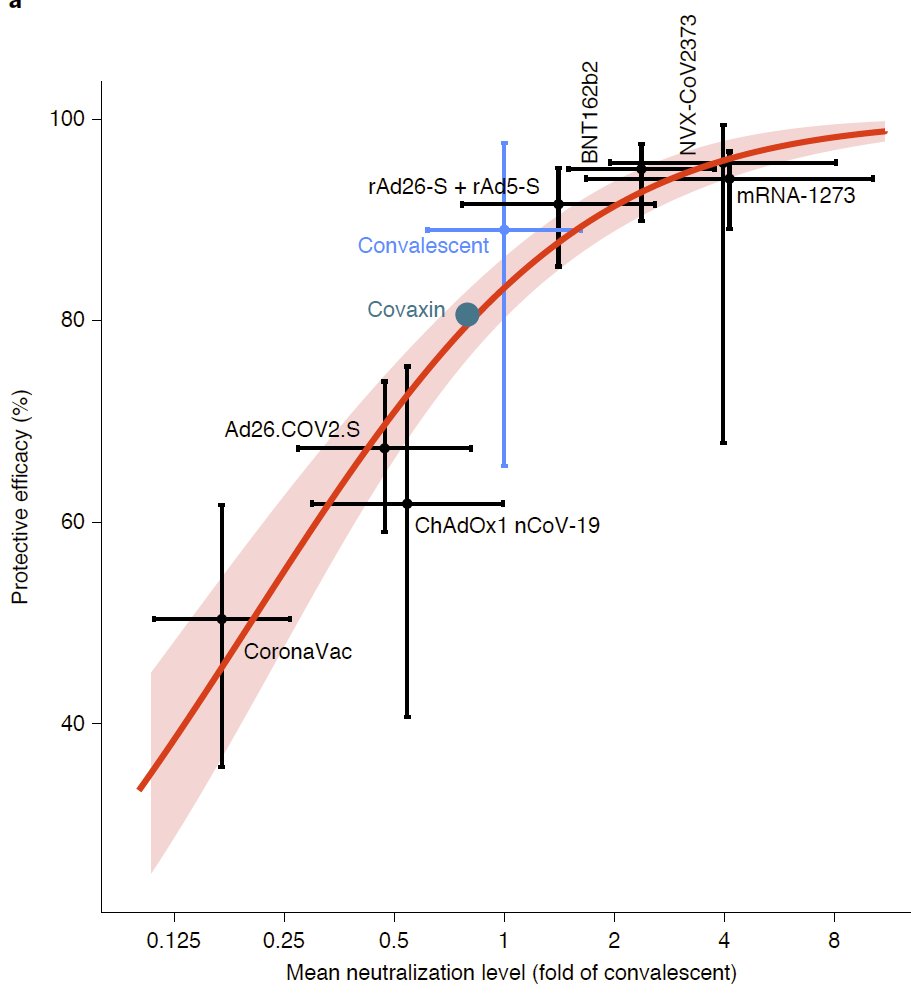
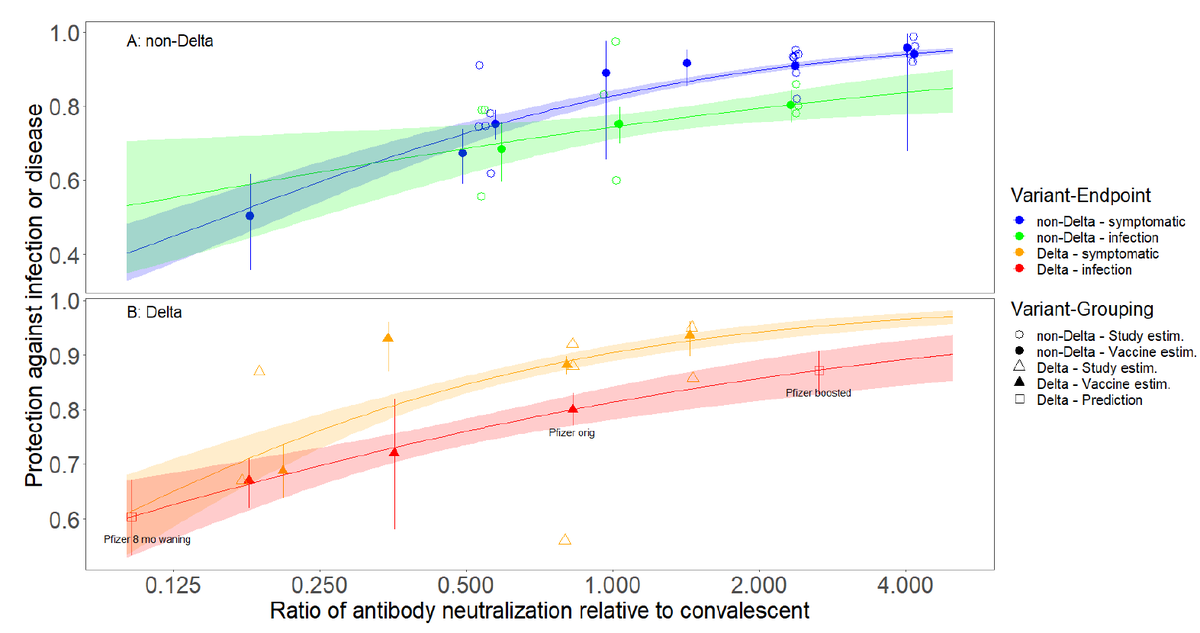
We extended this work by gathering many additional studies on protection against both symptomatic infection & all (but not "any") infections for both Delta & non-Delta variants. Each point is a vaccine-variant study & filled symbols aggregate data for a vaccine-variant.
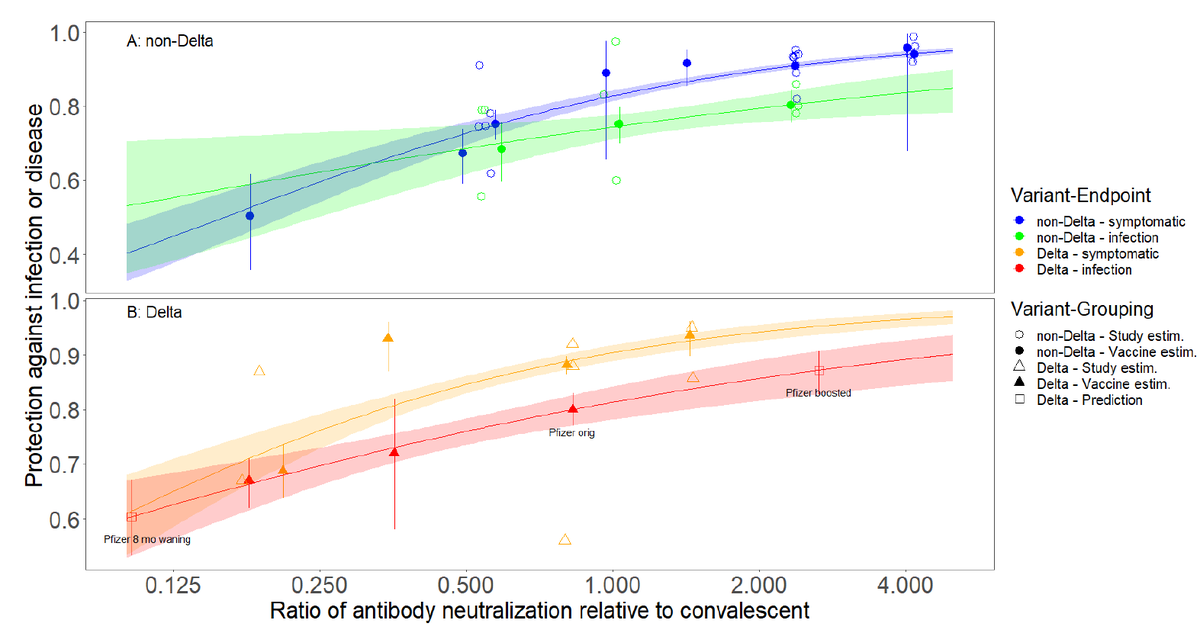
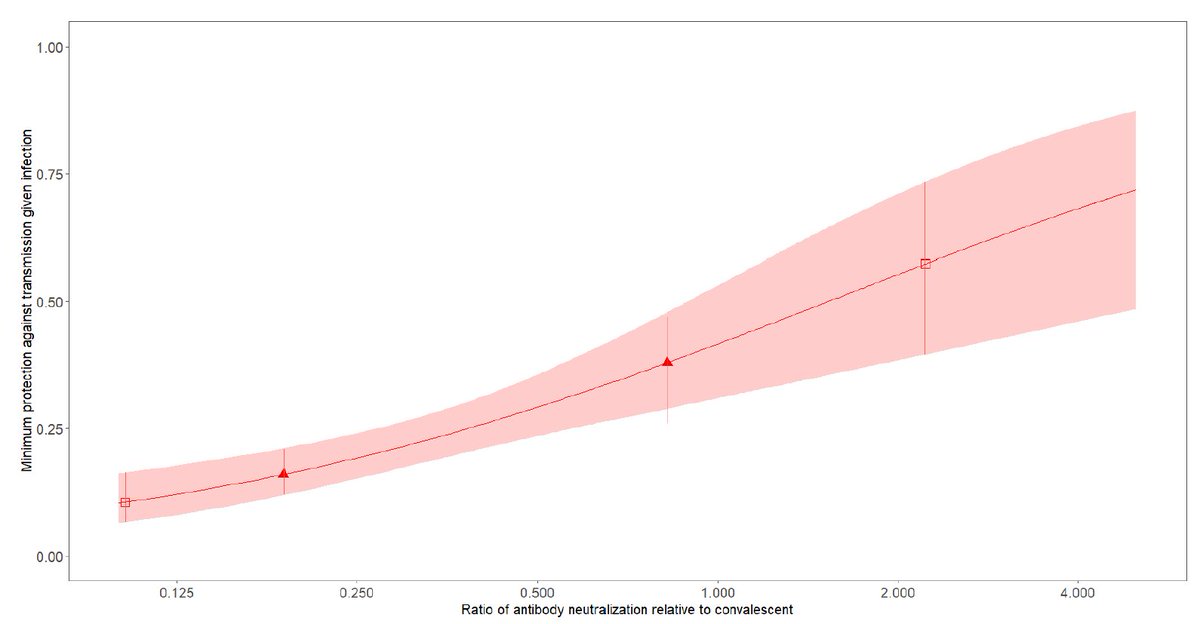
The relationship b/w protection against infection & neutralizing antibody levels (relative to convalescent sera) was strong, although data for Delta were limited to a few vaccines studied in rich countries (Pfizer, Astrazeneca). Protection was higher vs disease than infection.
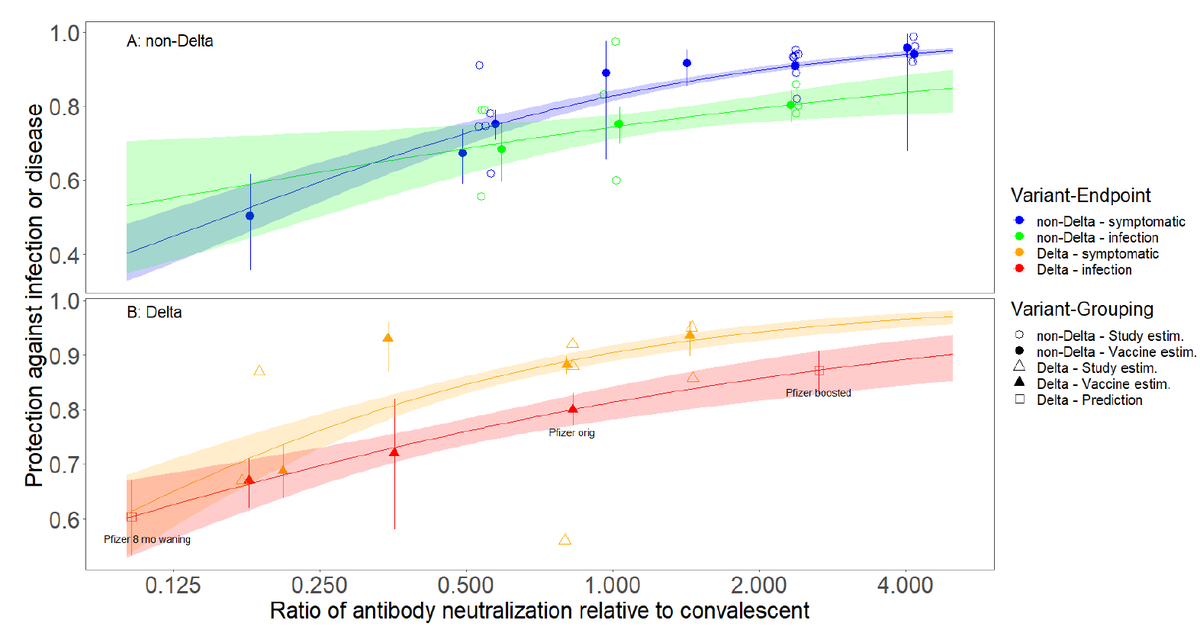
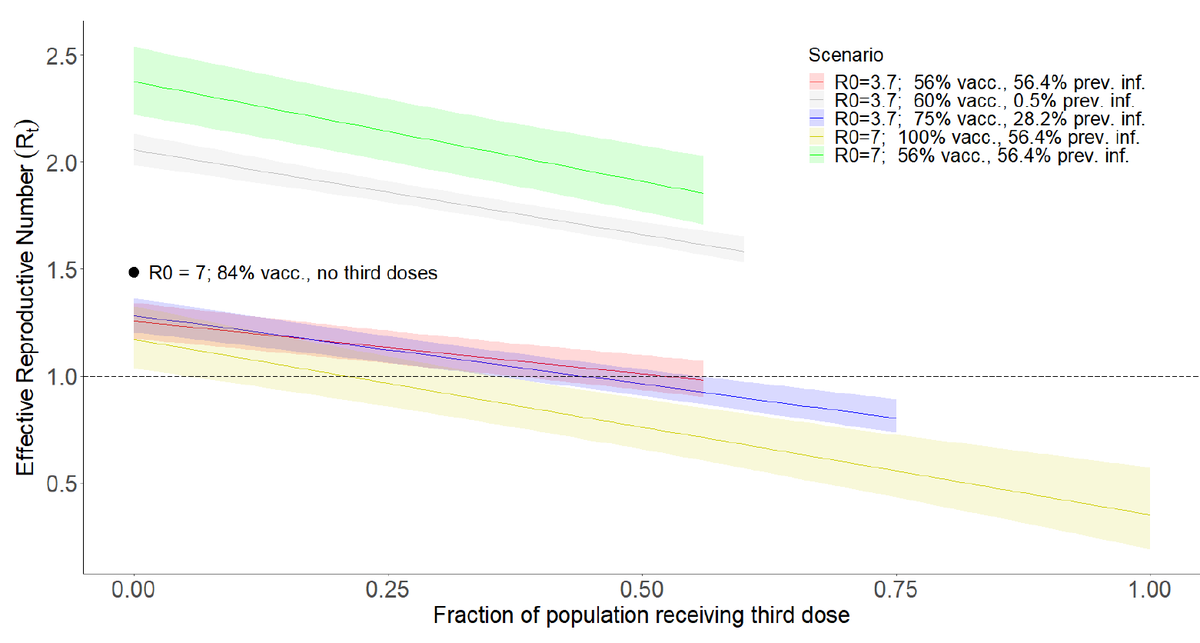
We used relationship for protection against all infections for Delta (red line) + very limited study of minimum protection against transmission given infection (doi.org/10.1101/2021.0…) to estimate impacts of boosting on transmission via the pathogen reproductive number, Rt.
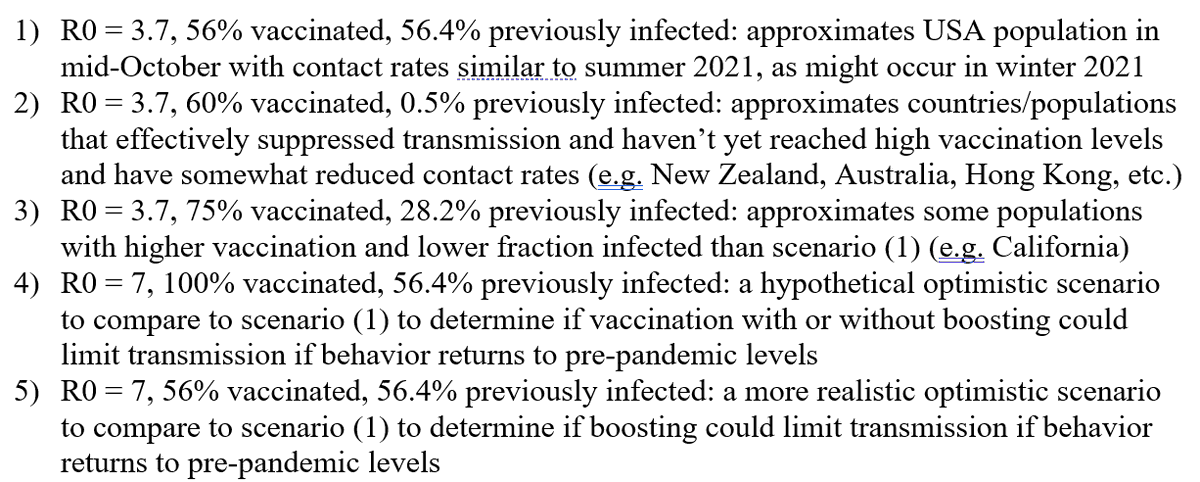
We considered 5 several scenarios that varied vaccine coverage, fraction previously infected, & contact rates (which scale R0 & Rt) which roughly describe, using mid-October data: USA, CA, New Zealand w/ summer surge 2021 (R0=~3.7) or pre-pandemic contact rates (R0=~7).
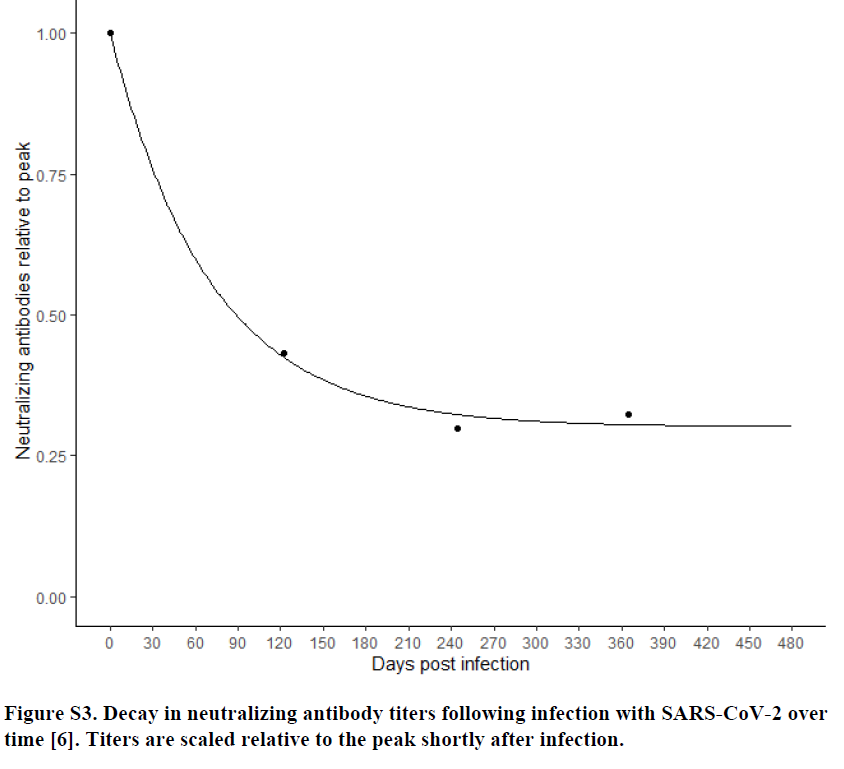
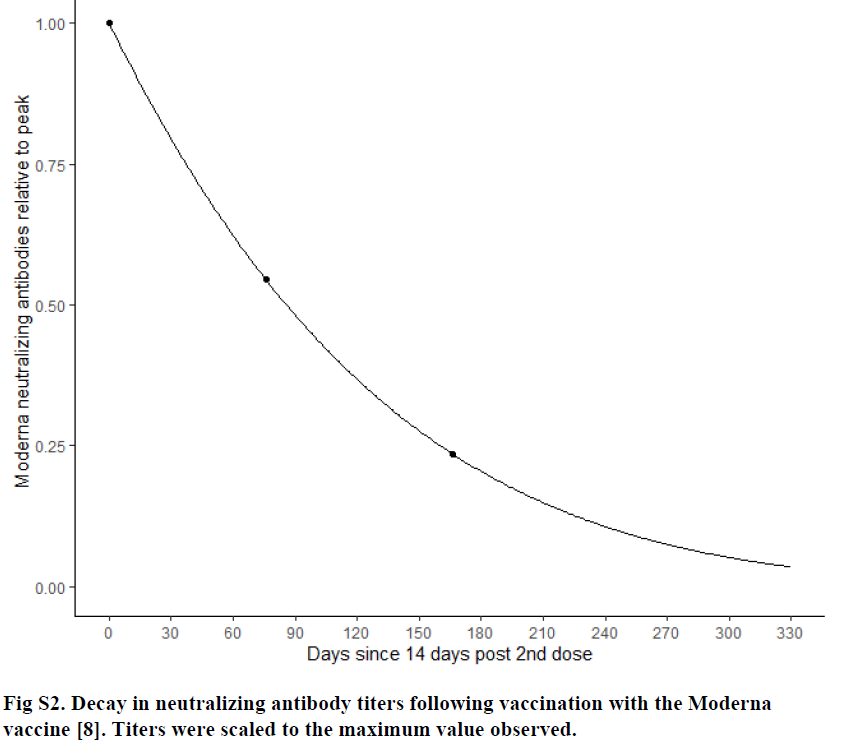
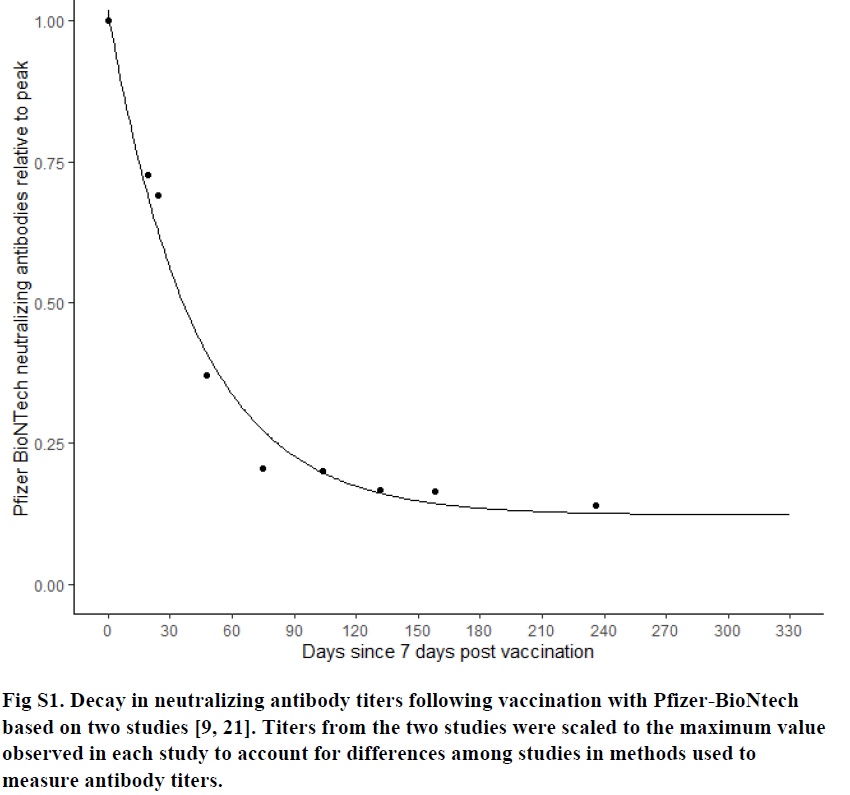
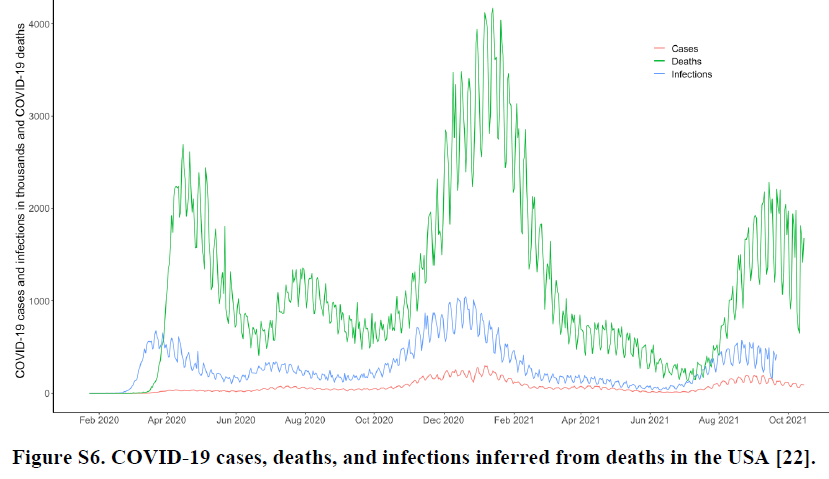
To take into account past vaccinations & infections, we had to estimate waning of protection based on patterns of waning of antibody levels for Pfizer, Moderna, previous infection & hybrid immunity & time series of infections & vaccinations by vaccine type.
We find:
Boosting could substantially reduce Rt, 21%-66%, with larger impacts for higher vaccine coverage & contact rates & smaller fraction previously infected.
Specifically
1)red line: boosting all US currently vaccinated could stop winter surge but only w/ lower contact rates
Boosting could substantially reduce Rt, 21%-66%, with larger impacts for higher vaccine coverage & contact rates & smaller fraction previously infected.
Specifically
1)red line: boosting all US currently vaccinated could stop winter surge but only w/ lower contact rates
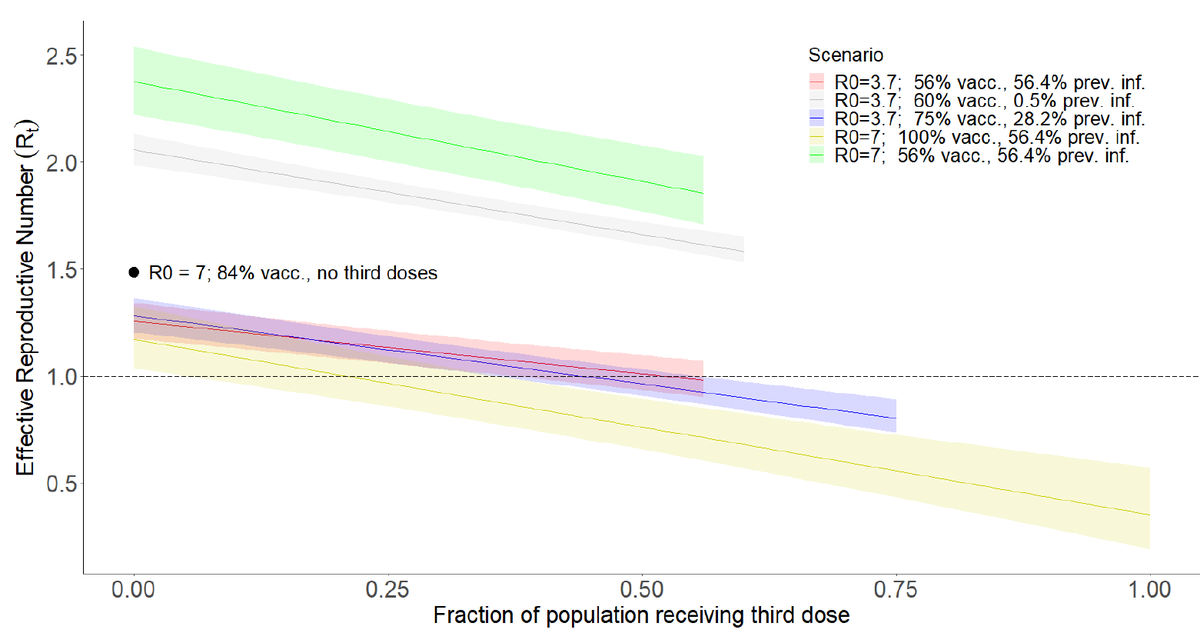
2) If contact rates return to pre-pandemic levels, need very high vaccine coverage (100%) & 25% boosted to prevent surge (yellow line). w/ current US vaccine coverage (56%) & estimated previous infection (56.4%) Rt remains far above one even if we boost everyone (green line).
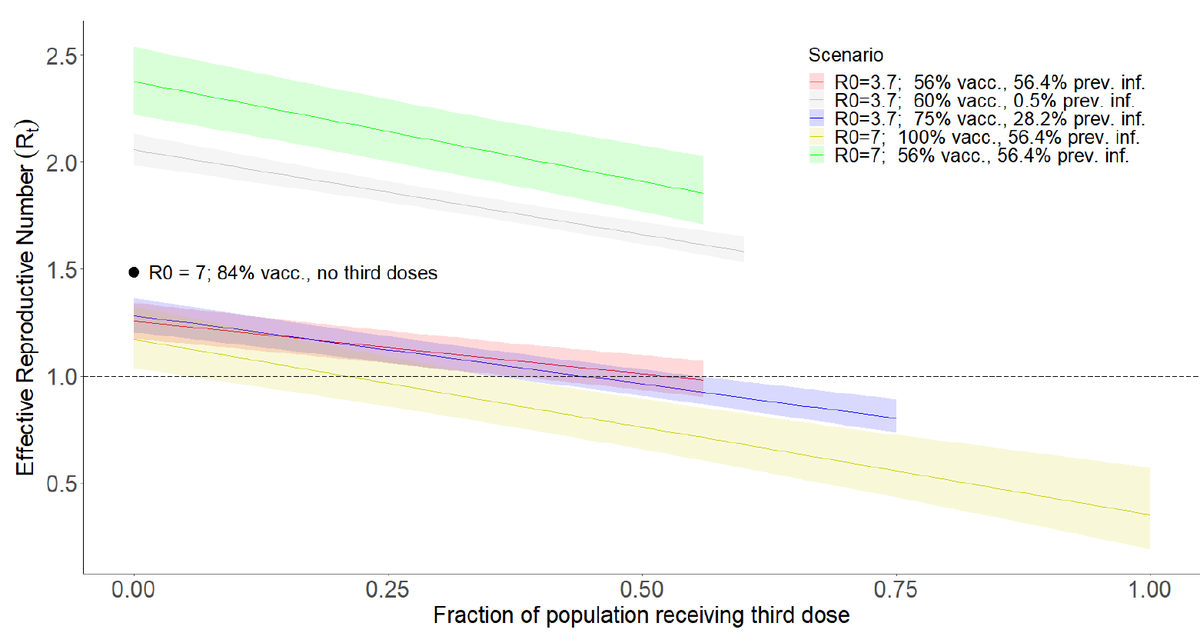
3) Places like Calif. (blue line), possibly UK (couldn't find good data on fraction previously infected - help!), could prevent surge w/ some boosting. Australia & New Zealand at risk of very high Rt b/c almost no protection from previous infection. Need to vaccinate fast!
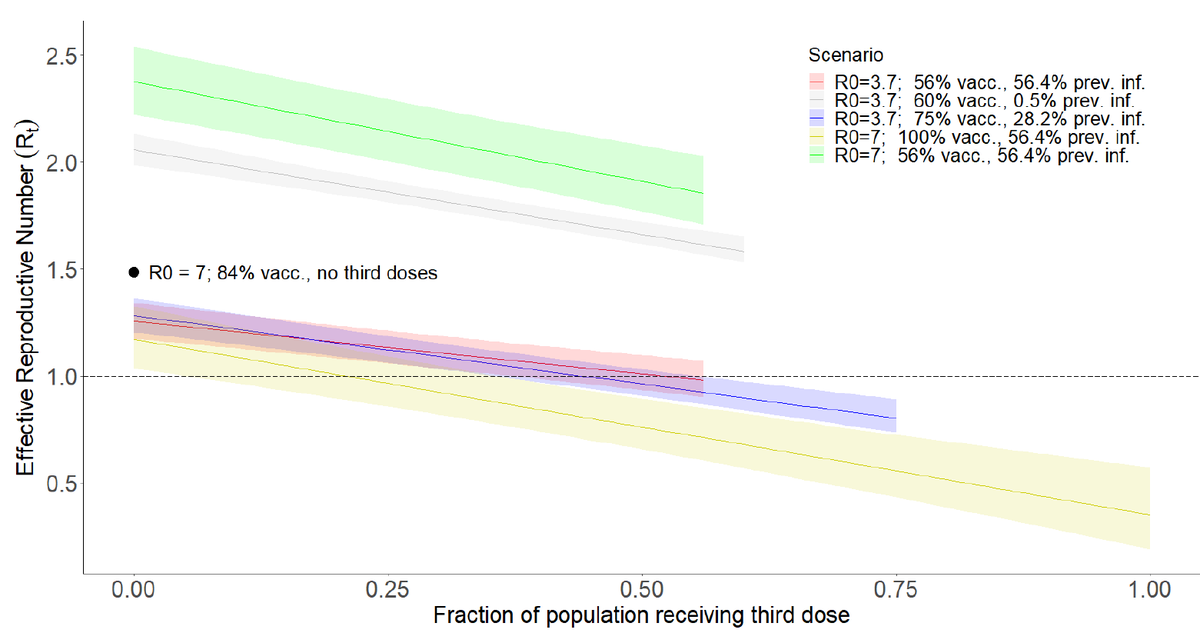
Finally, as expected, using 3rd doses to vaccinate unvaccinated is much more effective. Black dot shows Rt if all 3rd doses used at right end of green line were instead given to unvaccinated (2 shots each) to push coverage 56->84%. Much better, if it could be done.
Conclusions
-3rd dose substantially increases VE vs infection & transmission
-3rd doses could substantially reduce transmission & stop winter surge, but not w/ pre-pandemic behavior unless vacc coverage or prev infection high (~100%)
-doses (always) best used for unvaccinated
-3rd dose substantially increases VE vs infection & transmission
-3rd doses could substantially reduce transmission & stop winter surge, but not w/ pre-pandemic behavior unless vacc coverage or prev infection high (~100%)
-doses (always) best used for unvaccinated
Many caveats
Indirect measure of protection (no T-cells!)
Limited data esp. for transmission
No age-specific analysis
V. simple model: assume well-mixed pop for Rt
Didn't incorporate uncertainty in waning for Rt CIs (yet)
Indirect measure of protection (no T-cells!)
Limited data esp. for transmission
No age-specific analysis
V. simple model: assume well-mixed pop for Rt
Didn't incorporate uncertainty in waning for Rt CIs (yet)
Late addition (not yet in paper):
We can use relationship in paper to estimate (HUGE) benefit of getting vaccinated if you've been previously infected:
Protection vs infection increases from 62% -> 91%
Reduced chance of transmitting if infected:
12.5% ->76%
Get vaccinated!!!
We can use relationship in paper to estimate (HUGE) benefit of getting vaccinated if you've been previously infected:
Protection vs infection increases from 62% -> 91%
Reduced chance of transmitting if infected:
12.5% ->76%
Get vaccinated!!!
Critical feedback welcome!
@rozeggo @sbfnk @CT_Bergstrom @mishkendall @michaelmina_lab @bennyborremans @JoannaMasel
@mlipsitch @AdamJKucharski @LucaFerrettiEvo @joel_mossong @joel_c_miller @GidMK @taaltree @chrischirp @JamesWard73 @hampson_katie
@rozeggo @sbfnk @CT_Bergstrom @mishkendall @michaelmina_lab @bennyborremans @JoannaMasel
@mlipsitch @AdamJKucharski @LucaFerrettiEvo @joel_mossong @joel_c_miller @GidMK @taaltree @chrischirp @JamesWard73 @hampson_katie
Add. caveat: @michaelmina_lab has noted that a sharp increase in antibodies following vaccination often wanes quickly. Unfortunately, we currently don't know how long boosting will last. Have I missed a study from Israel or elsewhere? @florian_krammer @profshanecrotty @roby_bhatt
• • •
Missing some Tweet in this thread? You can try to
force a refresh