Nice thread @EdMHill describing modeling from 1 of 3 teams on possible outcomes in UK that guided recent decision to postpone re-opening.
Big takeaways:
-I wish US gov had been open to scientific guidance in 2020
-Big uncertainty in behavior changes w/ re-opening
cont.
Big takeaways:
-I wish US gov had been open to scientific guidance in 2020
-Big uncertainty in behavior changes w/ re-opening
cont.
https://twitter.com/EdMHill/status/1404517796978036739
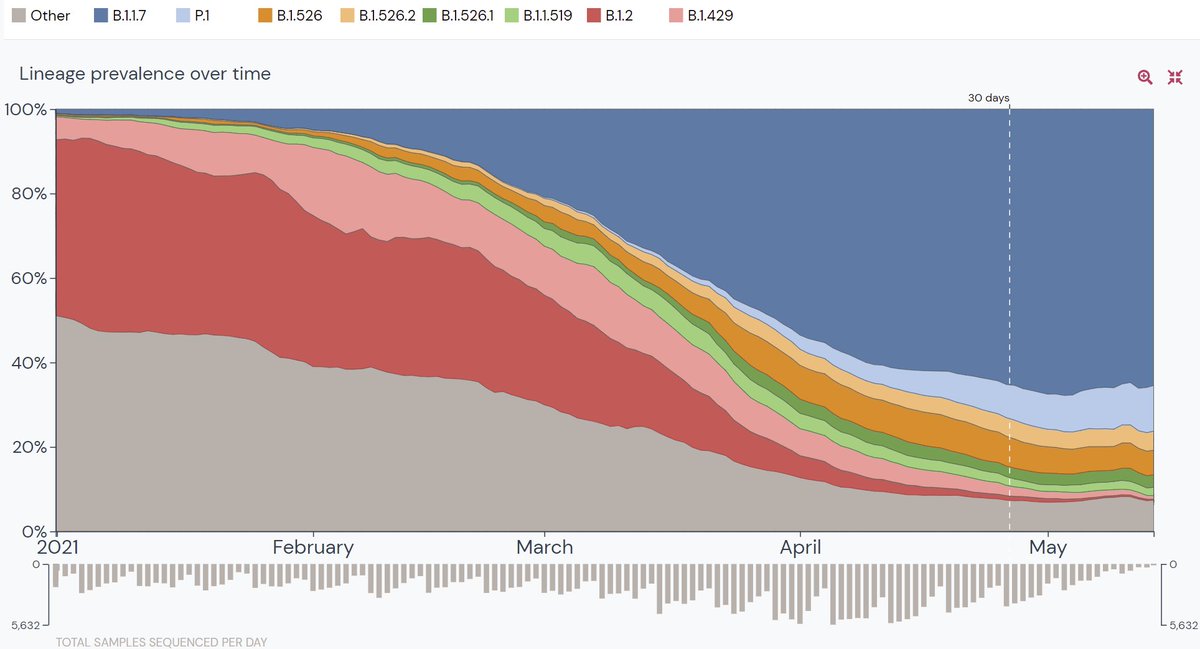
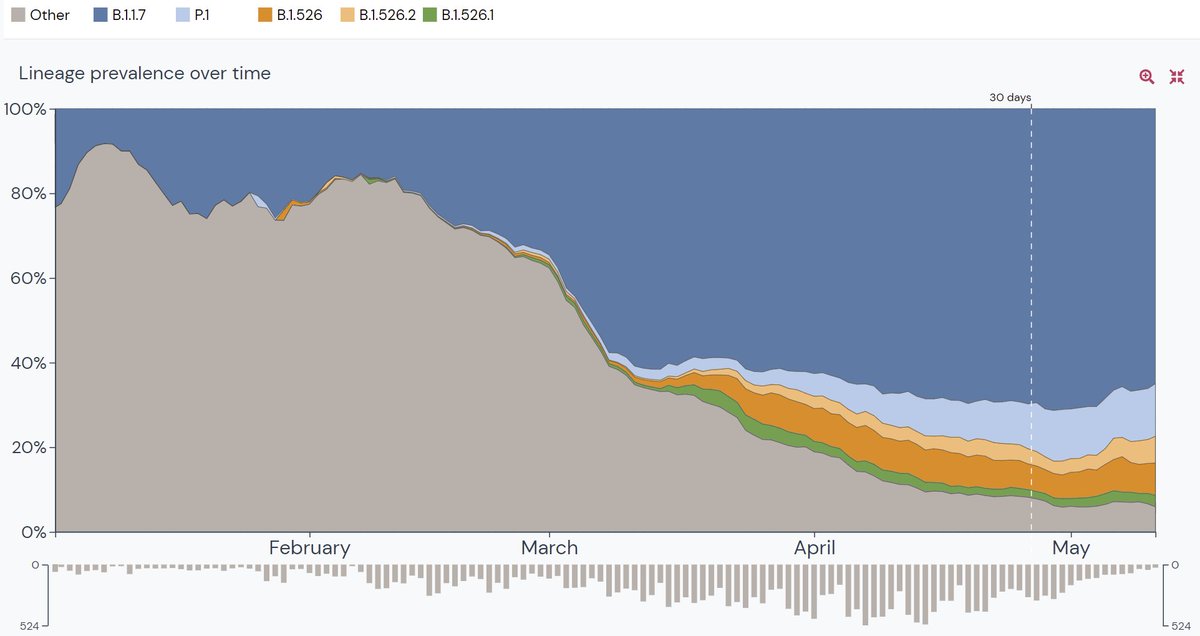
-Big uncertainty in relative transmissibility of delta (b.1.617.2) variant & vaccine effectiveness for transmission (not symptomatic disease). PHE-UK has provided fantastic real-time analyses of available data, but some critical data, that could be collected, are missing.
-Importance of limited vaccine supply. US can't seem to give away vaccine even with beer, lotteries & more. In UK (& most, but not all, of world) every dose is precious & in-demand.
*Clarification - thread describes modeling from 3 modeling groups not one.
• • •
Missing some Tweet in this thread? You can try to
force a refresh