
⚠️TRIPLING HOSPITALIZATIONS IN 2 WEEKS—In #Omicron epicenter of Gauteng Province, South Africa🇿🇦, there is more than **tripling of #COVID19 hospitalizations** in 2 weeks—➡️ from 135 hospital admissions to 418. This is data directly from 🇿🇦’s CDC @nicd_sa🧵
nicd.ac.za/diseases-a-z-i…
nicd.ac.za/diseases-a-z-i…

2) here is the exact #COVID19 hospitalizations breakdown for Gauteng Province by both public and private hospitals. It’s increasing equally - tripling in both classes of hospitals. This is not just a surveillance issue. Trust the @nicd_sa data first. nicd.ac.za/diseases-a-z-i…

3) breakdown many #COVID19 patients currently hospitalized / in ICU / on ventilator in Gauteng 🇿🇦—747 hospitalized, 57 in ICU, and 23 on a ventilator. @nicd_sa doesn’t give the time series for all of these. It’s still early. Less hope it doesn’t rise further.

4) Of the 747 currently hospitalized with #COVID19 in Gauteng Province (#B11529 epicenter of South Africa), 137 of the 747 hospitalized COVID patients are receiving “high care” or ICU care— or 18%.

5) of the 747 hospitalized for #COVID19 in #Omicron epicenter of Gauteng Province, 140 are receiving oxygen or on a ventilator—19%.

6) most recently, positivity in Gauteng soared from 1% to 30% in 2 weeks.

7) As a reminder, Gauteng Province is the epicenter of #Omicron where genome sequencing revealed it to now “becoming dominant” over even Delta.


8) Don’t let the misinformation hit ya without double checking the data first. The “Omicron is mild” was based on an out of context quote.
https://twitter.com/drericding/status/1464838724131471362
9) Also, don’t forget the well known lag between cases ==> hospitalization ==> then death. Cases have soared 6x already…. Hospitalizations are rising (see top), and death is a lagging indicator.
Figure by @Antonio_Caramia
Figure by @Antonio_Caramia

10) South Africa 🇿🇦 is also reporting most young #COVID19 patients are unvaccinated- 65%. And majority of the remainder are only partially vaxxed.
https://twitter.com/drericding/status/1465015829041451014
11) 💡Nota Bene in epidemiology— We also know that a more infectious disease that seriously harms fewer of those infected but infect more people ➡️ will ultimately maim more people (a greater absolute number seriously ill) than a high severity disease that is less infectious. 👀

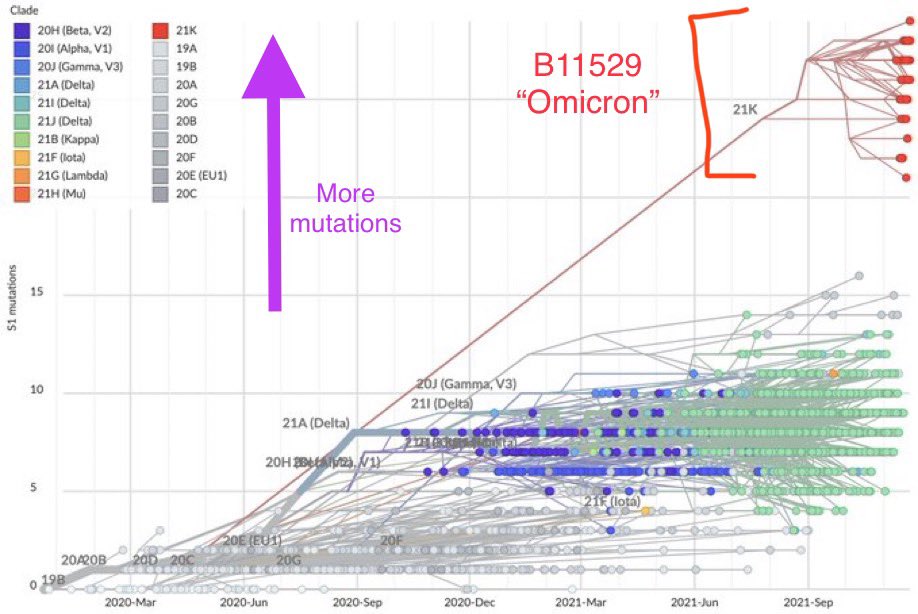
12) When I see a 🧬mutation divergence tree like this, it gives me pause. #Omicron is leaps & bounds different than other #SARSCoV2 variants. Evolution selected this unique combination for a reason—it wasn’t a regular rate of accumulating mutation errors. This is why the caution.
13) Beware the misinformation about it being “mild”. That’s a poorly quoted excerpt. And it’s not based on actual hospitalization data (see top post above). Don’t be misled.
https://twitter.com/DrEricDing/status/1464838724131471362
14) Feel free to fact check the hospitalization data I posted. Someone dug and tried to verify every number I posted on the 🇿🇦 Gauteng Province #OmicronVariant epicenter’s hospitalization.
P.s. If I ever make a materially sig factual error, I’m always happy to update/repost.
P.s. If I ever make a materially sig factual error, I’m always happy to update/repost.
https://twitter.com/Realanise/status/1465175627481292806
15) Here was @WHO’s official stances on all aspects of #Omicron — they still don’t know. But they acknowledge the increased hospitalizations is something to watch out for. We will have more epidemiological studies soon. Stay tuned.
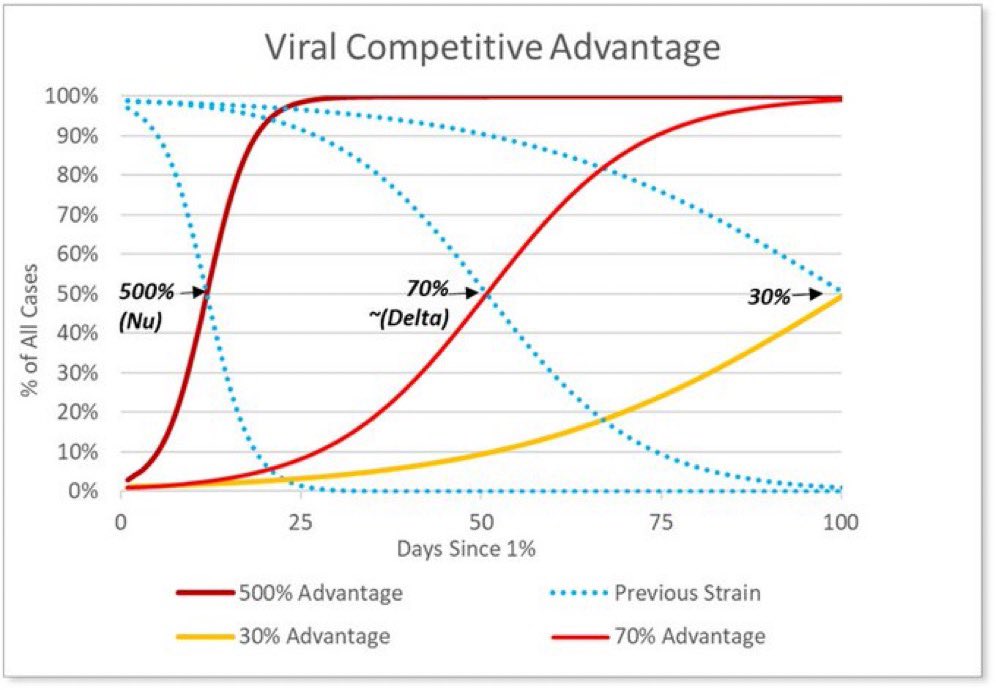
16) Let’s hypothetically suppose it is “milder”—but Even if it’s milder than delta, the increased transmissibility and/or immune escape would still make it more dangerous than delta. Exponentially more cases is still exponentially more hospitalizations & deaths! ~@lisa_iannattone

18) UPDATE— the #COVID19 hospitalization surge is now 4x in 2 weeks. Late reporting upped it from 3x yesterday to 4x today in the #Omicron-epicenter of Gauteng Province 🇿🇦. This is an acceleration it seems.

• • •
Missing some Tweet in this thread? You can try to
force a refresh




















