Big German Update!
- Excess Mortality 3,834 (+21.4%) in week 46/2021 vs median 16-20 (not age/pop. corrected)
- Covid deaths in week 46: (1,129) which only makes up 1/4 of the excess; if covid was the only excess that'd make up +6.4%
1/n
#Covid #Covid19 #Corona #Coronavirus
- Excess Mortality 3,834 (+21.4%) in week 46/2021 vs median 16-20 (not age/pop. corrected)
- Covid deaths in week 46: (1,129) which only makes up 1/4 of the excess; if covid was the only excess that'd make up +6.4%
1/n
#Covid #Covid19 #Corona #Coronavirus

So we can see something "strange" might be happening in Germany, majority of excess deaths (75%) are not from covid anymore...
Covid deaths are practically at the same level as last year though:
Covid deaths are practically at the same level as last year though:

Because cases are so much higher, CFR is also lower.
Prevalence is likely the same, as latest RKI sentinel showed still 6% prevalence of SARS-CoV-2 for week 46.
Prevalence is likely the same, as latest RKI sentinel showed still 6% prevalence of SARS-CoV-2 for week 46.



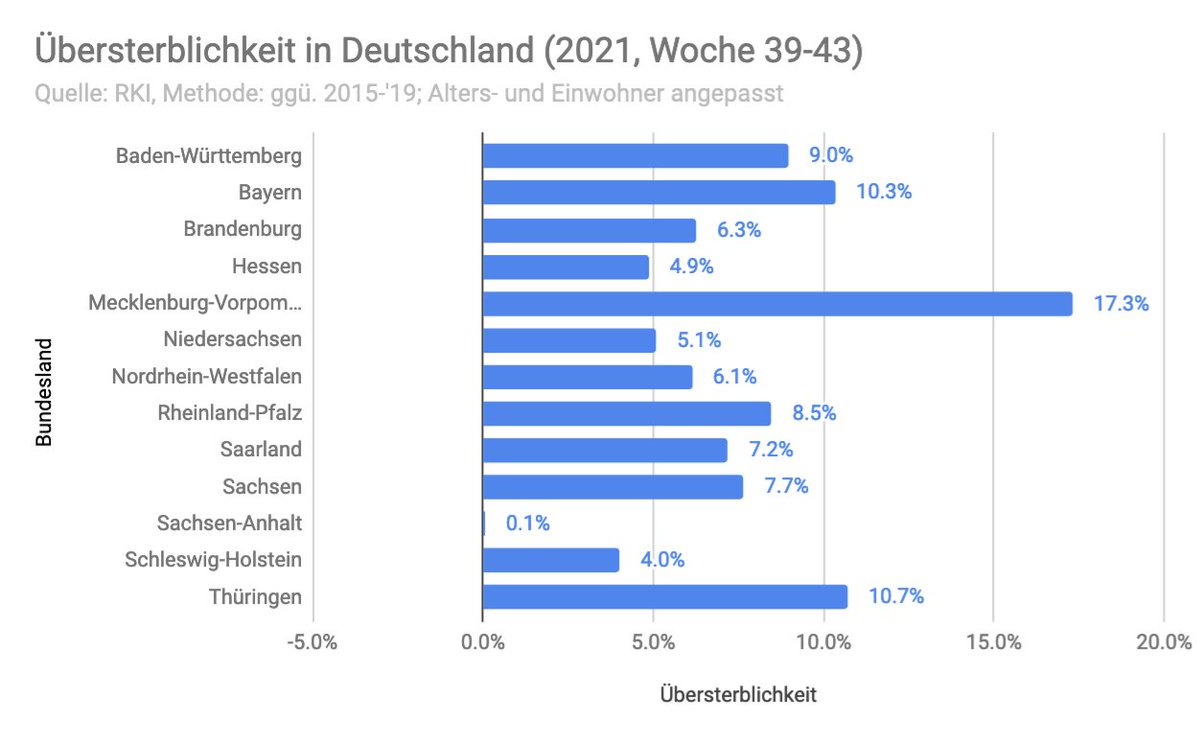
Now let's look at excess death correlation vs vaccination for last 4 weeks available.
Including all states we can see a weak correlation in favor of the vaccinated states. Correl -0.47; R2=0.22; p>0.0649.
Including all states we can see a weak correlation in favor of the vaccinated states. Correl -0.47; R2=0.22; p>0.0649.


However, if we exclude the city states, which likely skew the analysis due to their different characteristics, it allows for a more fair comparison.
Here we can see no significant correlation. Correl=-0.18, R2=0.03; p=0.56
Here we can see no significant correlation. Correl=-0.18, R2=0.03; p=0.56

This means we'll have to wait an see how it plays out in the full season, especially since the vaccine efficacy is known to fade fast.
Finally let's look at some models:
Finally let's look at some models:
Model 1, shows that Germany has peaked, the model still does not pick up the peak...

Model 2, shows that a peak is near.

If we adjust the fit of model 2 to the last 4 days, we can see that Germany likely has peaked.
Now, we still need to see if the curve will actually start declining, or if we'll see other outbreaks, happening, like last year...
Now, we still need to see if the curve will actually start declining, or if we'll see other outbreaks, happening, like last year...

Sources & Calculations:
docs.google.com/spreadsheets/d…
docs.google.com/spreadsheets/d…
docs.google.com/spreadsheets/d…
destatis.de/DE/Themen/Gese…
docs.google.com/spreadsheets/d…
docs.google.com/spreadsheets/d…
docs.google.com/spreadsheets/d…
docs.google.com/spreadsheets/d…
docs.google.com/spreadsheets/d…
destatis.de/DE/Themen/Gese…
docs.google.com/spreadsheets/d…
docs.google.com/spreadsheets/d…
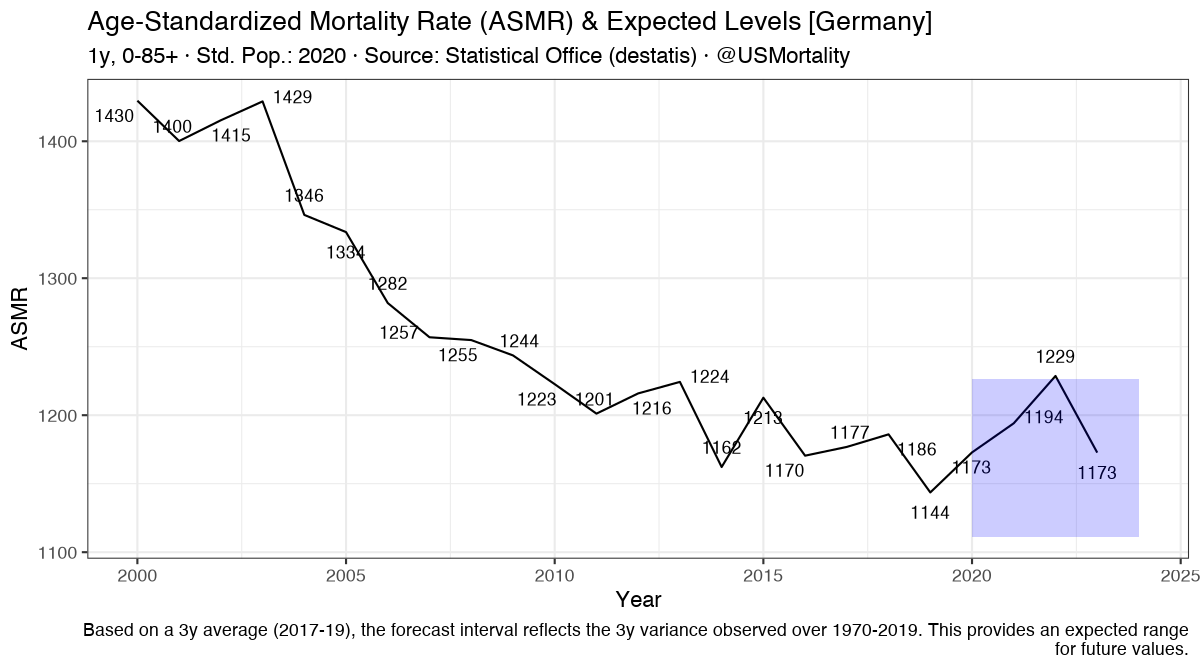
Great work by @jens_140081 shows that even with age and population corrected baseline, Germany is looking at +18% excess mortality for week 46/2021. In contrast covid only makes up for about 1/3 of that.
https://twitter.com/jens_140081/status/1465666274906759180?s=20
My twitter buddy @jens_140081 just told me that the age and population adjusted excess mortality for week 46 was:
- All-cause excess: +2,673
- Covid19: 1,129
Hence, even after adjusting for population and age changes, Covid19 mortality makes up only 42% of excess --> 58% other!!!
- All-cause excess: +2,673
- Covid19: 1,129
Hence, even after adjusting for population and age changes, Covid19 mortality makes up only 42% of excess --> 58% other!!!
One thing to note here, is that we are comparing "deaths by reported date" in contrast to "date of death"..
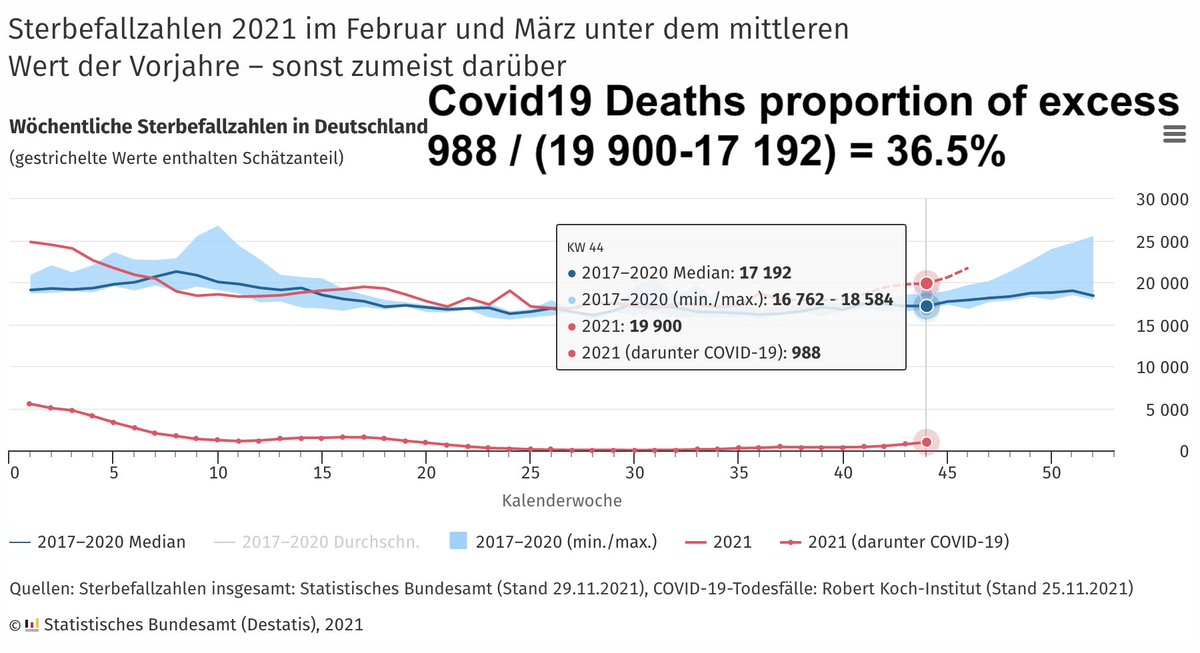
However if we compare the actual values for the latest week available, we can see that also only 36.5% of excess deaths are from covid!
However if we compare the actual values for the latest week available, we can see that also only 36.5% of excess deaths are from covid!
• • •
Missing some Tweet in this thread? You can try to
force a refresh