**VALVE CASE OF THE MONTH**
@BrHeartValveSoc
Last case of 2021!
If EVER you needed an example of why not to judge a 3-dimensional structure with 2-dimensional imaging...this it it!
I think you'll like this one...😁
#echofirst #cardiotwitter #MedTwitter
@BrHeartValveSoc
Last case of 2021!
If EVER you needed an example of why not to judge a 3-dimensional structure with 2-dimensional imaging...this it it!
I think you'll like this one...😁
#echofirst #cardiotwitter #MedTwitter
Male, late 60s, underwent biological MVR (29mm) 11 yrs previously for
Severe MR. Has permanent AF & VVIR pacemaker
Admitted to local hospital with breathlessness
This is admission chest x-ray
Severe MR. Has permanent AF & VVIR pacemaker
Admitted to local hospital with breathlessness
This is admission chest x-ray

Treated with diuretics, offloaded successfully
Rpt CXR after a week - nearly normal
Rpt CXR after a week - nearly normal

First TTE after offloading...
AP4Ch with colour Doppler
@cardiacLucy @nat_echo @RobChamb87 @BiancaJudyC @vitormweaver @scrivsy85 @em_echo @boegel_kelly @CKFreeEcho @wess_jmm @LukshmiM @MCRImaging
@BSEcho
@cardiacLucy @nat_echo @RobChamb87 @BiancaJudyC @vitormweaver @scrivsy85 @em_echo @boegel_kelly @CKFreeEcho @wess_jmm @LukshmiM @MCRImaging
@BSEcho
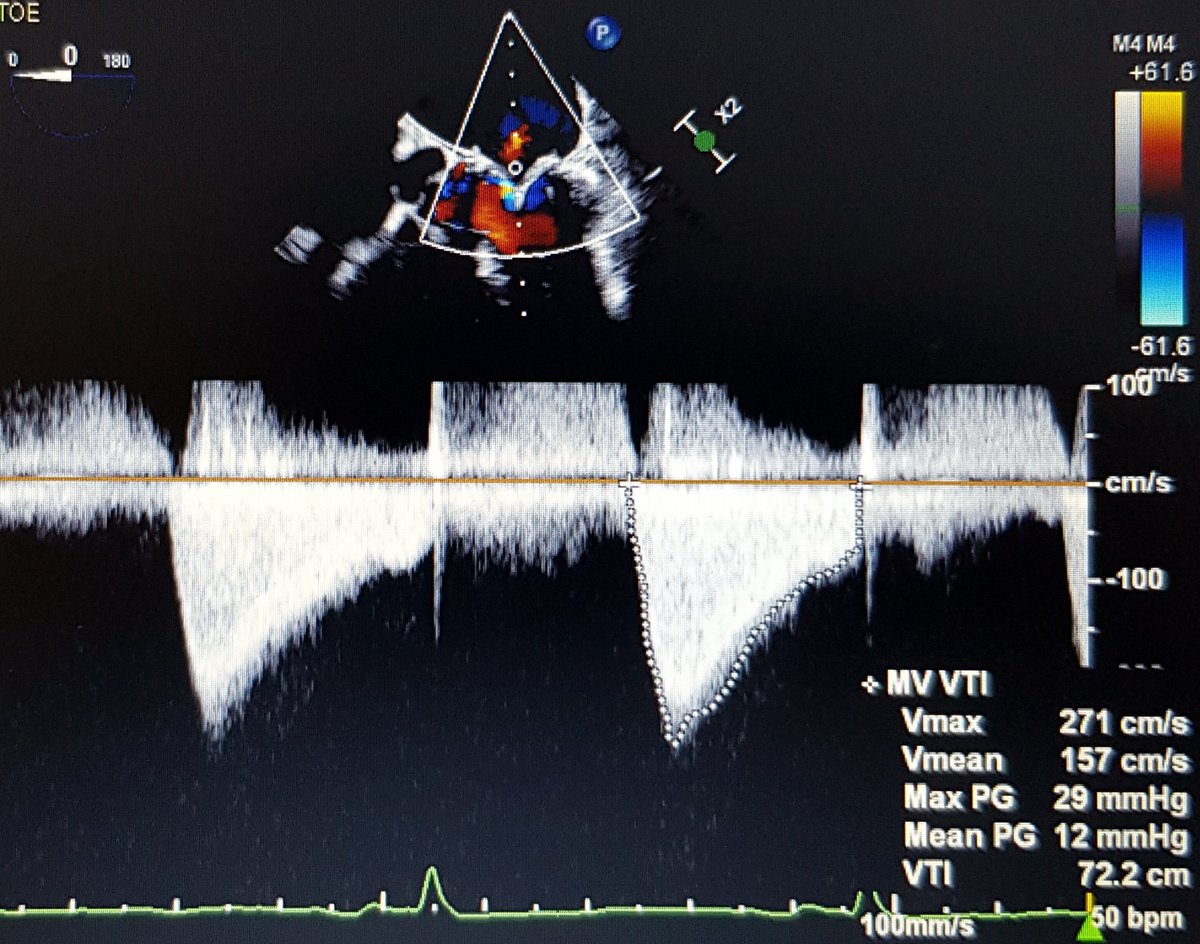
Mean MV gradient 13mmHg! Not tachycardic, well aligned CW Doppler
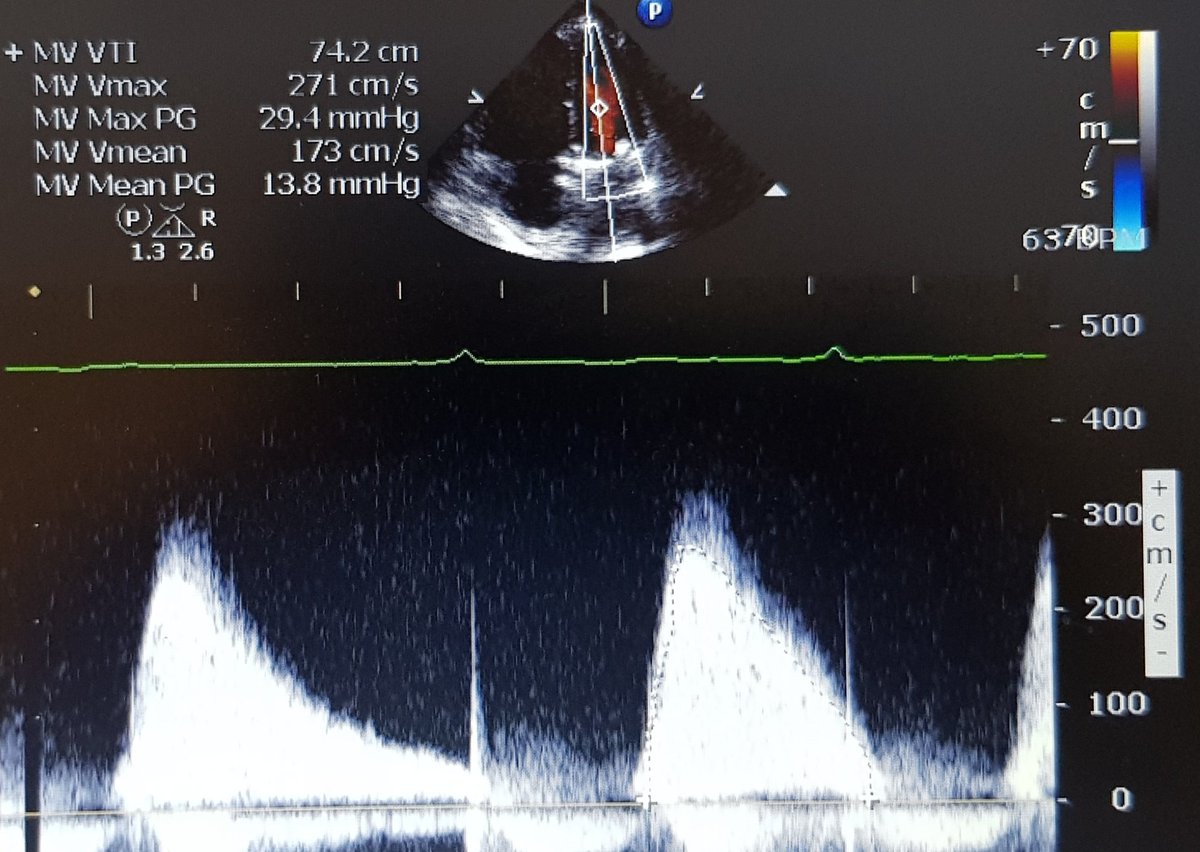
Admission with fluid overload
Very high gradient across 11yr old bioprosthesis
Could be SVD...so local hospital proceeds to TOE. Here are their 2D images
Very high gradient across 11yr old bioprosthesis
Could be SVD...so local hospital proceeds to TOE. Here are their 2D images
120degree view
One leaflet clearly fixed in this view, other leaflet moves well
Still a lot of turbulence on colour Doppler imaging
TOE MV mean gradient still high, above 10mmHg...
So, I'm sent images and asked what do I think. Patient stable & euvolaemic. Valve doesn't seem severely stenotic on 2D images (1 leaflet seems fixed). I wasn't convinced he needed urgent re-do surgery, but surgeons accepted transfer to our centre for more tests
So, we decide to repeat the TOE, this time with 3D imaging
Images here from our #echofirst heroine @EuniceOnwordi - great view of MVR from LA aspect
Images here from our #echofirst heroine @EuniceOnwordi - great view of MVR from LA aspect
And here is key image from LV aspect...
So, you can see now that actually TWO leaflets are fused together and only one is moving freely
So, you can see now that actually TWO leaflets are fused together and only one is moving freely
Took the dataset into 3DQ, used 3D-MPR for a 3D-planimetry MV area...which was 1.5cm2
So, you've seen 2D & 3D images, CW Doppler & clinical presentation
POLL! Does this patient need a mitral valve re-do operation?
@SCTSUK @BISMICS @ishahm
@EnochAkowuah1 @hatemsoliman
@mrjzacharias @DrMoritzWvB
@dralisonduncan
POLL! Does this patient need a mitral valve re-do operation?
@SCTSUK @BISMICS @ishahm
@EnochAkowuah1 @hatemsoliman
@mrjzacharias @DrMoritzWvB
@dralisonduncan
Well, the surgeons decided to go back to theatre and replace the valve
As 3D TOE revealed, they found 2 leaflets were fused together & fixed, whilst 1 leaflet moved freely
Patient opted for another bioprosthesis
As 3D TOE revealed, they found 2 leaflets were fused together & fixed, whilst 1 leaflet moved freely
Patient opted for another bioprosthesis
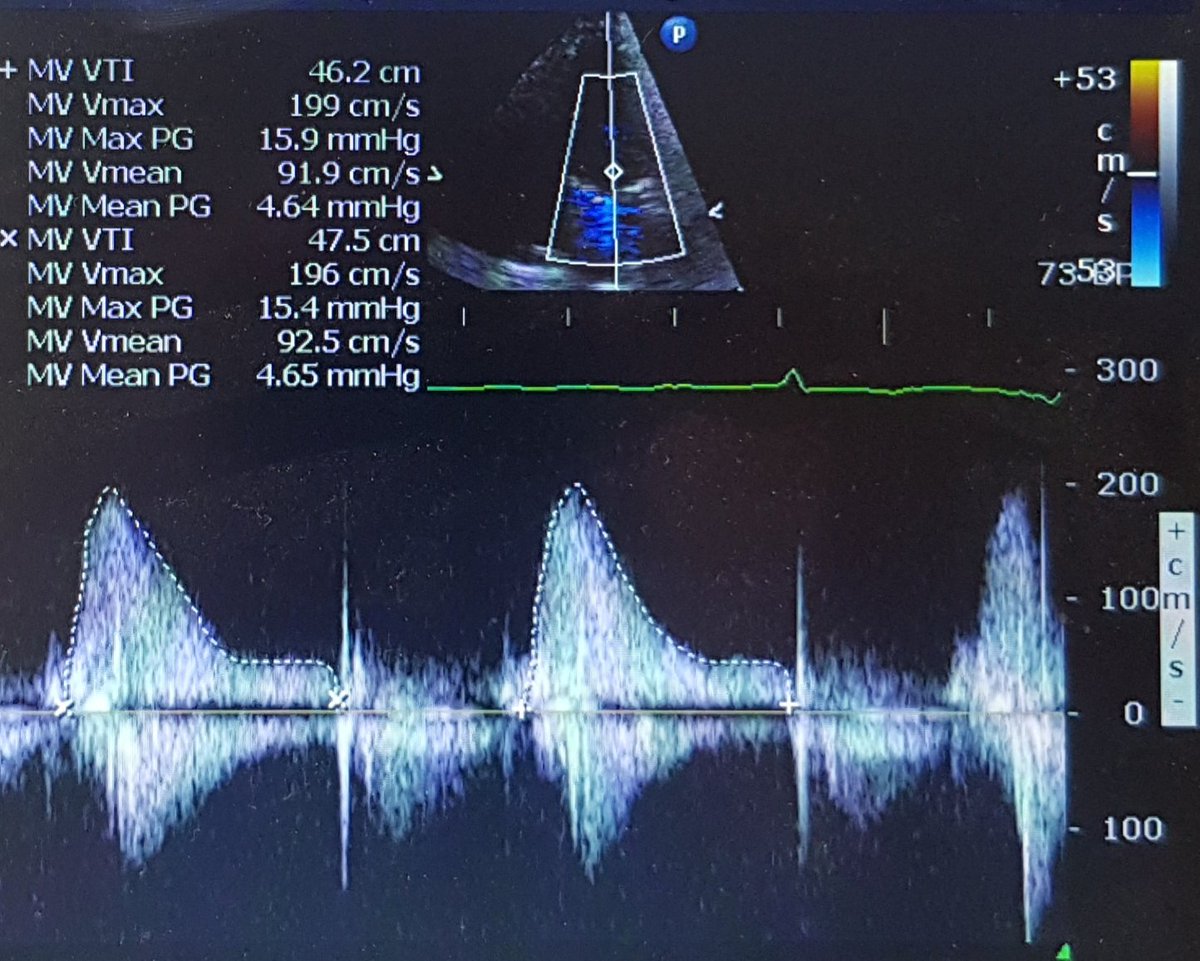
Here is the post-op echocardiogram - mean MV gradient down to ~4mmHg!
I think it's a great reminder of the utility of 3D echocardiography especially for assessing prosthetic valves - the 2D images here didn't suggest that valve alone should cause MVG of >10mmHg
3D crucial here
I think it's a great reminder of the utility of 3D echocardiography especially for assessing prosthetic valves - the 2D images here didn't suggest that valve alone should cause MVG of >10mmHg
3D crucial here
• • •
Missing some Tweet in this thread? You can try to
force a refresh