
1) Welcome to our THIRD #accredited serialized #tweetorial from @onc_ce, your new (and only) home for the latest education from #experts on #cancer care. #Physicians #nurses #pharmacists #PAs and #NPs can all earn 0.5h CE/#CME by following this thread!
2) We continue to highlight the San Antonio Breast Cancer Symposium (#SABCS21), with more expert commentary for OUR #tweetorial followers! Our content authority is Hal Burstein MD (@drhburstein) from @DanaFarber Cancer Institute & @HarvardMed.
3) @Onc_ce and its companion website oncologytweetorials-ce.com are supported by educational grants from Astra Zeneca and Daiichi Sankyo and content is intended for #healthcare providers. Faculty disclosures are listed at oncologytweetorials-ce.com/disclosures/.
4) @SABCSSanAntonio is a primary international scientific symposium for interaction and exchange among basic scientists and clinicians working in #breastcancer. #SABCS21 was a hybrid meeting this year, with many renowned researchers welcoming the opportunity to collaborate FTF!
5) Most #breastcancers–early or late stage–are ER+ so improvements in management of ER+ tumors are really imp't from a public health perspective. CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) are well established in treatment of ER+ MBC.
(nejm.org/doi/full/10.10…)
(nejm.org/doi/full/10.10…)

6) CDK4/6 inhibitors are approved for use in first line (with AIs) or in second line with the SERD fulvestrant. But how well do these drugs work in different subtypes of advanced, ER+ breast cancer?
7) At #SABCS21, @drlisacarey reported on outcomes for ER+ breast cancers subtyped genomically as luminal A, luminal B, basal like, or HER-enriched. Remember, all are ER+. Clear benefit was shown for CDK4/6i (here, ribociclib) in all subtypes except basal-like.

8) For a long time, there was some nihilism that we couldn't improve OS in ER+ advanced #breastcancer; there were too many possible lines of therapy. Recent updates have proven that is not the case! In fact, they suggest OS should be expected as a primary outcome for new agents.
9) Here for example is update of MONALEESA-2 trial from @DrLisaCarey @UNC_Lineberger. 1st line therapy of ER+ #metastaticbreastcancer with AI (letrazole +/- ribociclib: >12m gain in OS. Interesting that the OS benefits are greater in absolute terms than PFS benefits . . .

10) . . . and look to last longer/emerge later. Suggests CDK4/6i exposure truly shifts growth patterns of sensitive, ER+ tumors.


11) Mechanisms of resistance to CDK4/6i are not well known but include RB loss. Provocative data from @sloan_kettering suggests that germline BRCA2 mutations make for resistance to CDK4/6i treatment.

12) Implications? For tumors that are ER+ & BRCA2 associated, go with PARPi before CDK4/6i? Not really known, clinically. And maybe in adjuvant setting, for ER+ and BRCA2+, would opt for PARPi instead of CDK4/6i in higher risk cases . . .
13) . . . where either is being considered. But this is @DrHBurstein speculating here. Remember – most, but not all, BRCA1 tumors are ER neg.
14) With success of CDK4/6i treatment, new cyclin-dependent kinase inhibitors are emerging. CT7001/samuraciclib is a CDK7 inhibitor. In combo with fulvestrant, it shows RR of 12% in pts with prior CDK4/6i treatment. Side effect profile differs in important ways from CDK4/6i…

15) . . . because with CDK7i, there is no neutropenia. There is, however, diarrhea and nausea/vomiting.

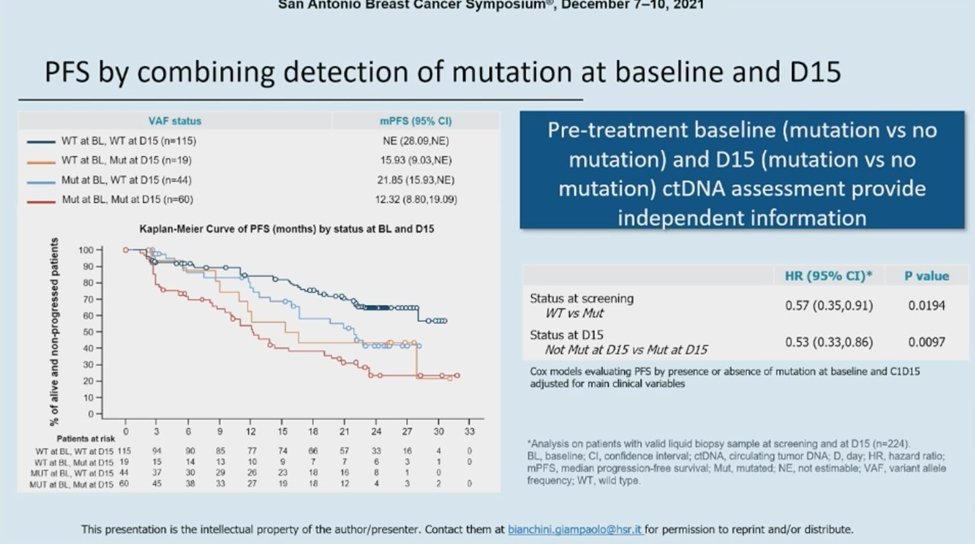
16) Genomic sequencing of ER+ MBC on liquid biopsy helps stratify patients. In BioltaLEE study from @BianchiniGP, all patients received let + ribo. Those tumors w/ no targeted mutations had better PFS than those with genomic mutations.

17) Lesson: for sensitivity to endocrine treatments, fewer mutations probably better than more.
18) Activating mutations in ER (ESR1m) are commonly found after AI treatment & on tumor progression. Presumably, they account for resistance to AI therapy as the ER is ‘on’ even in the absence of estrogen.
19) So what do you know?
ESR1 mutations are associated with all of the following except:
a. ER activity in the absence of estrogen
b. Sensitivity to CDK4/6 inhibitors
c. Resistance to aromatase inhibitors
d. Shorter overall PFS
ESR1 mutations are associated with all of the following except:
a. ER activity in the absence of estrogen
b. Sensitivity to CDK4/6 inhibitors
c. Resistance to aromatase inhibitors
d. Shorter overall PFS
20) Mark you answer and come back tomorrow for the remainder of this look at 🔑data from #SABCS21, along with your link to FREE CE/#CME! Nods to @erikahamilton9 @hoperugo @teamoncology @ElisaAgostinett @prat_aleix @StoverLab @drteplinsky @OncBrothers @MridulaGeorgeMD @jesusanampa
21) Welcome back to our #accredited #tweetorial on highlights of new ER+ #breastcancer, advanced stage, from #SABCS21. I am @drhburstein and you have found your new, ONLY source for oncology CE/#CME by tweetorial! Thanks for joining! Hello to @josemarciofigu1 @aftimosp @DrSGraff
22) Now that ESR1m can be identified on liquid biopsies, a question is whether early identification of ESR1m could prompt a change in therapy that would be clinically advantageous. The PADA-1 trial from @institut_curie set out to test that hypothesis.

23) In PADA-1, patients with ER+ MBC received AI+palbociclib. They had serial liquid biopsy to test for ESR1m acquisition, along with traditional staging. If the ESR1m was rising without over tumor progression on scans, patients were randomized . . .
24) . . . to ongoing AI/palbo vs switching to fulvestrant/palbo. Switching led to longer PFS (12M vs 6M median). But …

25) Important to remember that many patients with 6 mo or longer have no overt clinical progression despite rising ESR1m & ongoing AI treatment, AND that there was crossover tx that typically lasted for ~ 4 M, so the ‘net benefit’ of detection and switch is relatively modest.

26) Finally, we saw the first phase 3 data for a new class of anti-estrogen targeting drugs, called selective estrogen receptor degraders (SERDs) (pubmed.ncbi.nlm.nih.gov/34236340/). (Figure from futuremedicine.com/doi/10.2217/fo…)
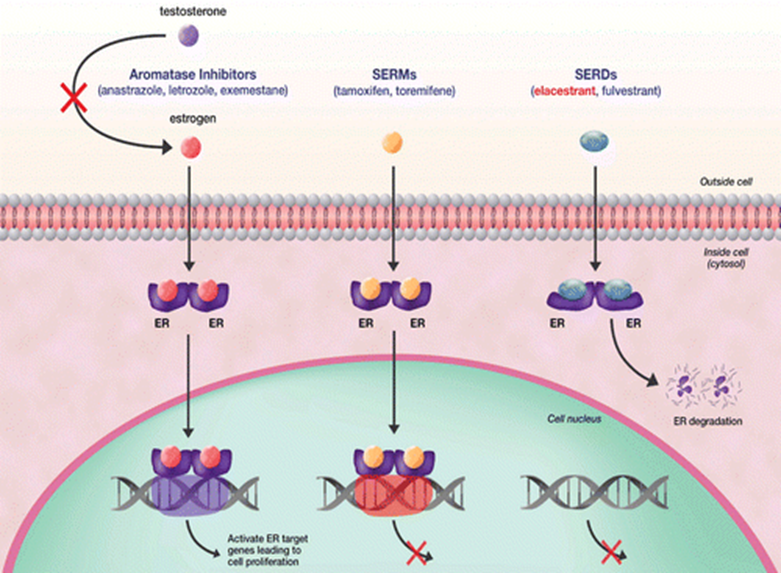
27) Fulvestrant is a SERD but requires intramuscular injection. Newer SERDs are orally available, and several have shown potent ability to cause intracellular loss of ER through protein degradation. The question is: how would they compare to existing endocrine options?
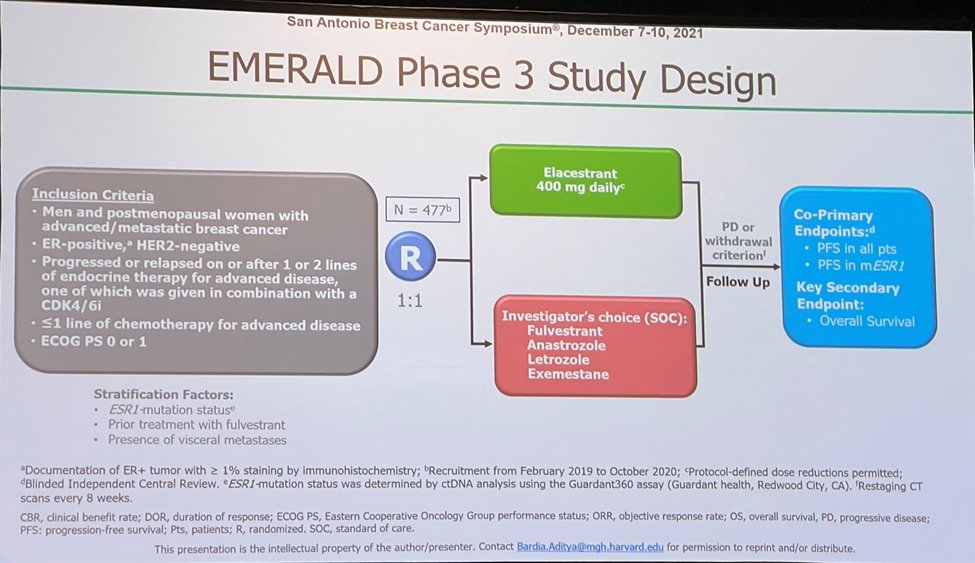
28) The EMERALD study (@dradityabardia) compared the SERD, elecestrant, against standard of care (SOC) endocrine treatments in a cohort of patients with ER+ MBC and prior ET+CDK4/6i therapy. Nearly all patients had prior AI treatment. SOC options included AI or fulvestrant.
29) Elecestrant showed modest improvement in PFS (3M vs 2M) compared to SOC therapies. But look at the shape of the progression curves.
30) Important to note that about half of the tumors are endocrine resistant and progress right away (red circle). Then the curves begin to diverge a bit favoring elecestrant, including a robust tail.

31) Most important comp is between elecestrant & fulvestrant in the cohort of patients who were naïve to prior fulvestrant. In the Forest plot, that group still has relative benefit with elecestrant comp'd to fulvestrant tho the absolute difference remains modest in median PFS.

32) What do you know?
Side effects of the first oral SERD, elecestrant, include:
VOTE before you scroll down!
Side effects of the first oral SERD, elecestrant, include:
VOTE before you scroll down!
33) It’s (a). Side effects of #elecestrant included greater risk of nausea than #fulvestrant.
Many are hopeful that this will be the first oral SERD to gain regulatory approval.
Many are hopeful that this will be the first oral SERD to gain regulatory approval.
34) One possible lesson of EMERALD is that median PFS may not be the best endpoint for endocrine refractory ER+ cancers. It might be more clinically meaningful to focus on rates of 6M or 12M PFS, given that half the cancers progress right away. @tmprowell @FDAoncology
35) SO there you have it--a quick review of data from #SABCS21 on ER positive breast cancer, advanced stage. You've just earned 0.5h CE/#CME! Go to oncologytweetorials-ce.com/ERBCadvanced to claim it! I am @drhburstein and I hope you will FOLLOW US for more expert-authored programs!
• • •
Missing some Tweet in this thread? You can try to
force a refresh


