🚨 US states with a higher fully vaccinated #Covid19 population, saw an increase in all-cause mortality in Q4/2021 compared to Q4/2020!
Slight positive Pearson correlation is visible R2=0.22, p=0.00.
#Covid #Covid19 #Corona #Coronavirus
Slight positive Pearson correlation is visible R2=0.22, p=0.00.
#Covid #Covid19 #Corona #Coronavirus

When comparing mortality and the impact of vaccination from an epidemiological perspective, it is important to look at similar time periods and then assess the impact of the vaccines.
Some jump to early conclusions, when just looking at a single time period:
Some jump to early conclusions, when just looking at a single time period:

Here's the same chart with Q4/2020 data. As we can clearly see, there was already a strong difference/slope in mortality even without any vaccination.
Likely explanation for this are other con-founders such as, general health, drug use, co-morbidities, obesity, etc.
Likely explanation for this are other con-founders such as, general health, drug use, co-morbidities, obesity, etc.

Hence it is important to compare the change in mortality after the vaccination has been introduced to asses it's impact.
Here's a bigger version:
Here's a bigger version:

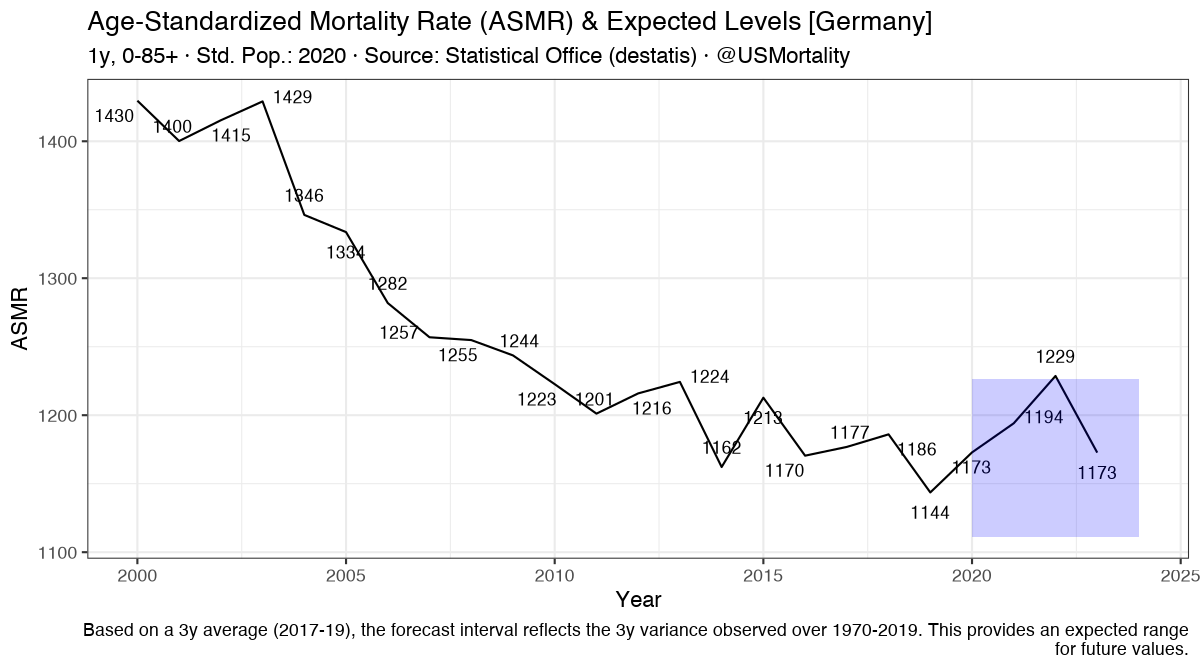
Note, that mortality here is age-corrected & population adjusted all-cause mortality, using the US 2000 standard population table.
Doc: docs.google.com/spreadsheets/d…
Doc: docs.google.com/spreadsheets/d…
If you want to see the individual states, please refer to usmortality.com
• • •
Missing some Tweet in this thread? You can try to
force a refresh