
An in-depth review of pediatric femoral shaft fractures.
If you're interested in orthopedics or pediatrics you'll definitely want to check this review out!
1/10
If you're interested in orthopedics or pediatrics you'll definitely want to check this review out!
1/10

Pediatric femoral shaft (PFS) fractures constitute a small portion of pediatric fractures roughly 1-2% with a bimodal age distribution
Most common causes:
✯ Toddlers: falls
✯ Teenage/adolescent: MVA
Most common causes:
✯ Toddlers: falls
✯ Teenage/adolescent: MVA
In children younger than walking age child abuse must be suspected. As high as 80% of PFS fractures in this age group are due to child abuse.
In the toddler age group as high as 25% of PFS fractures are due to child abuse, so it must be ruled out.
In the toddler age group as high as 25% of PFS fractures are due to child abuse, so it must be ruled out.
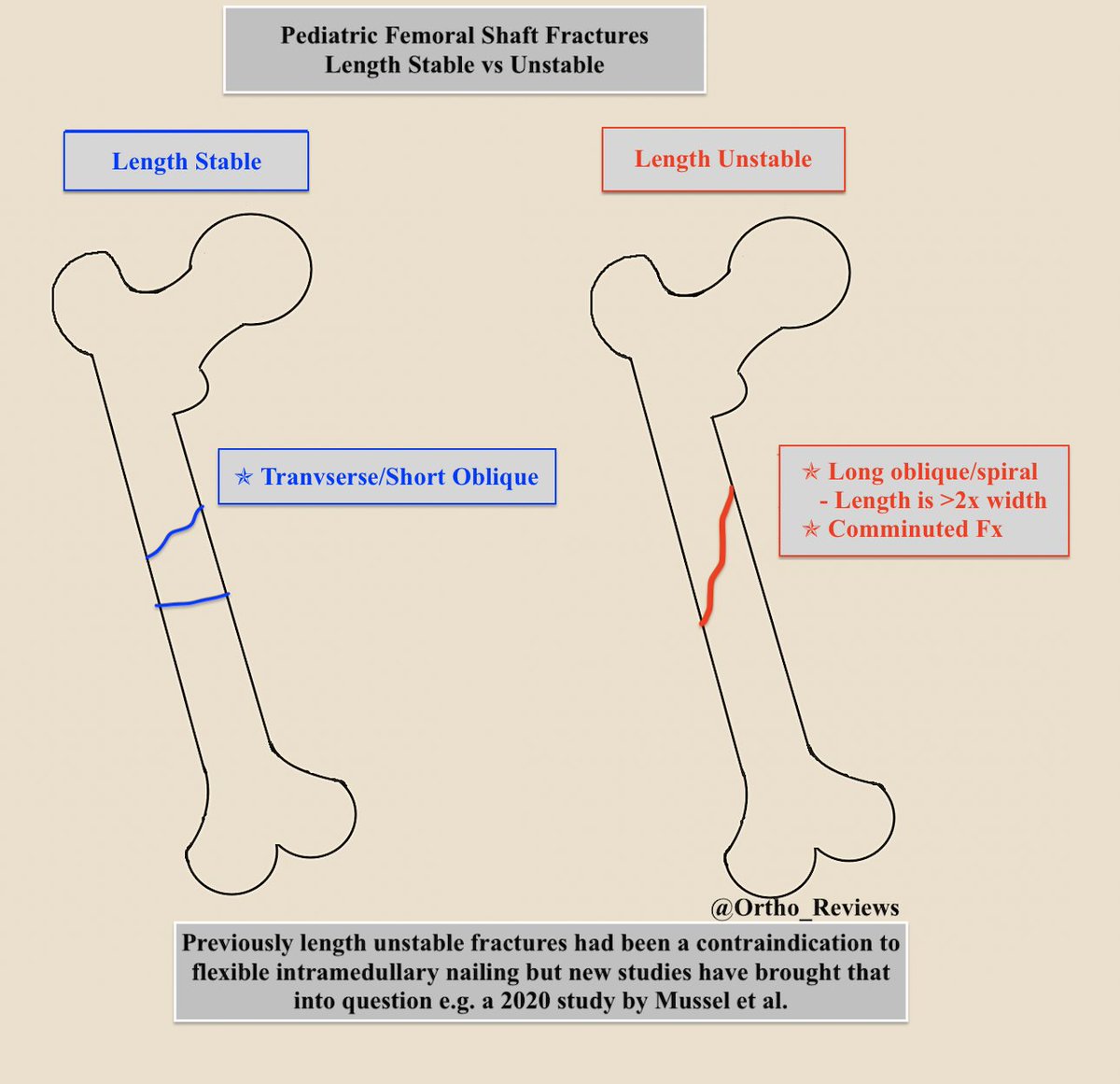
Length Stable vs. Length Unstable fractures may guide treatment decisions, though recent studies have brought this into question.
Which of the following is a length unstable fracture pattern?
Which of the following is a length unstable fracture pattern?
Length Unstable Fractures are described as:
✯ Long Oblique or Spiral Fractures
-Fracture length is > 2x the width
✯ Comminuted Fractures
✯ Commonly they have > 2 cm shortening
✯ Long Oblique or Spiral Fractures
-Fracture length is > 2x the width
✯ Comminuted Fractures
✯ Commonly they have > 2 cm shortening
Fracture treatment is guided by the patient's age and weight.
Which of the following would be a good treatment option for a 3 y.o. 14 kg boy presenting with a minimally displaced short oblique mid-femoral shaft fracture?
Which of the following would be a good treatment option for a 3 y.o. 14 kg boy presenting with a minimally displaced short oblique mid-femoral shaft fracture?
Treat options based on age, weight, and stability of fracture:

Non-operative management:
Children < 6 mo: Pavlik Harness (left)
Children 6 mo-5 yo: Spica Casting (right)
Acceptable reduction criteria for casting:
Sagittal angulation: 20°
Coronal angulation: 10°
Malrotation: 10°
Shortening: 2 cm
Children < 6 mo: Pavlik Harness (left)
Children 6 mo-5 yo: Spica Casting (right)
Acceptable reduction criteria for casting:
Sagittal angulation: 20°
Coronal angulation: 10°
Malrotation: 10°
Shortening: 2 cm


Operative management:
Flexible Intramedullary nailing: (left)
< 11 yo.
< 50 kg
Length Stable Fx
Rigid IM nail (right) / plating:
> 11 yo.
> 50 kg
Length Unstable Fx
Flexible Intramedullary nailing: (left)
< 11 yo.
< 50 kg
Length Stable Fx
Rigid IM nail (right) / plating:
> 11 yo.
> 50 kg
Length Unstable Fx


Complications:
✯ Leg length discrepancy
✯ Nonunion is rare
✯ Muscle Atrophy
✯ Femoral Head AVN
Lateral trochanteric entry has a ↓ risk of AVN when compared to piriformis entry for antegrade nailing.
✯ Leg length discrepancy
✯ Nonunion is rare
✯ Muscle Atrophy
✯ Femoral Head AVN
Lateral trochanteric entry has a ↓ risk of AVN when compared to piriformis entry for antegrade nailing.
If you enjoyed this review, please like or retweet to help the page grow and give us a follow!
Author: @CSMorford
#FemurFracture #Pediatric #Peds #Ortho #Orthopedics #OrthoTwitter #Bones #Trauma #MedEd #MedicalEducation #MedTwitter #ERAS #MedStudent #Tweetorials #Radiology
Author: @CSMorford
#FemurFracture #Pediatric #Peds #Ortho #Orthopedics #OrthoTwitter #Bones #Trauma #MedEd #MedicalEducation #MedTwitter #ERAS #MedStudent #Tweetorials #Radiology
• • •
Missing some Tweet in this thread? You can try to
force a refresh










