
1) Welcome to a new #accredited #tweetorial on currently available treatments for mineralocorticoid receptor (MR) antagonism (#MRA), the differences among them, and how these differences impact on treatment of cardio-reno-metabolic diseases #CaReMe #FOAMed
2) Our expert author is Dr. Patrick Holmes MB BS, MSc, DipTher, MRCGP (@drpatrickholmes), a GP Partner at St. George’s Medical Practice, Darlington for 23 years. He is a Trustee for the Primary Care Diabetes Society and is Associate Editor for Diabetic Medicine @diabeticmed. 

3) This program is supported by an educational grant from Bayer & is intended for #healthcare providers. Author disclosures can be found at ckd-ce.com/disclosures/. Prior programs, still available for CE/#CME credit, are at ckd-ce.com. CE/#CME credit 🇬🇧🇪🇺🇨🇦🇺🇸
4) Credit available for #physicians #physicianassociates #nurses #nursepractioners #pharmacists First, a poll. Which of the following are potential unwanted effects of MR antagonism using spironolactone? Answer before you scroll ⤵️!
5) The answer is d, hypokalaemia. Spironolactone is associated w/⬆️risk of #hyperkalaemia. Before investigating the differences in the currently commercially available #MRAs, let's review the basics. MR is a steroid hormone receptor.
6) Steroid hormone receptors [e.g., androgen receptor, progesterone receptor, glucocorticoid receptor (GR) etc…] are a sub-family of intracellular receptors & nuclear transcription factors.
7) The MR has a complex structure, with a DNA-binding domain that interacts with the nuclear DNA, a ligand-binding domain as well as two areas of activation function.
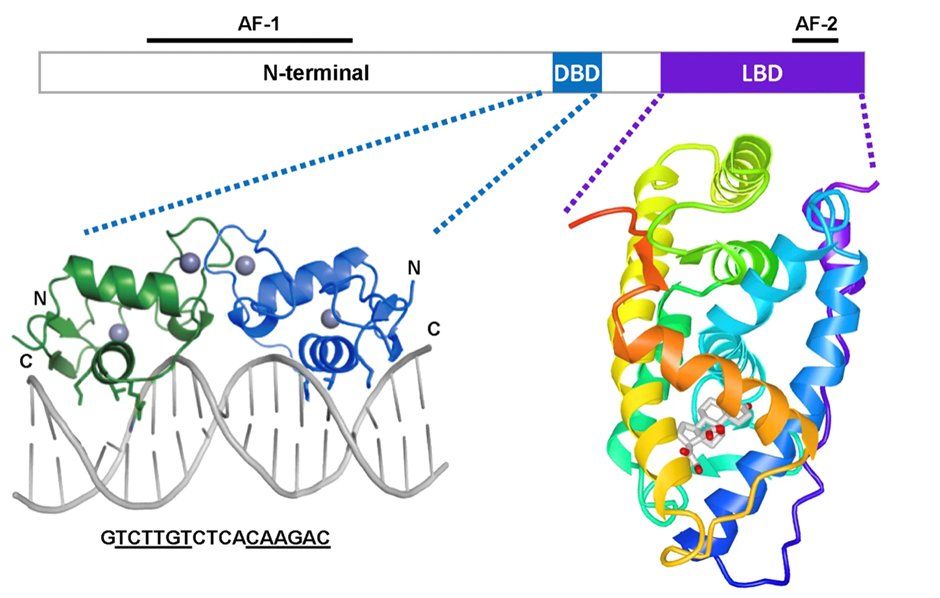
8) Whilst the GR is activated by the hormone/ligand cortisol, the MR is promiscuous with the same binding affinity for aldosterone & cortisol. Furthermore, progesterone competes with aldosterone for MR binding with similar affinity, acting as a MRA. (onlinelibrary.wiley.com/doi/10.1002/cp…)
9) In 1987 the MR gene was cloned. This in turn led to animal experiments using MR knock-out (MRKO) strains compared to normal ‘wild-type’ strain animals. Typically, rodents.
10) Complete MRKO is lethal with 10 days of birth due to the ensuing severe pseudohyperaldosteronism, thus demonstrating the critical importance of MR in salt, water, & #bloodpressure maintenance during early life.
11) MRKO cardiac cells compared to wild-type in a myocardial infarction 🐭 model led to :
⤴️ infarct healing
👉improved cardiac remodelling
⤵️ pulmonary oedema
⤵️ contractile dysfunction
⤴️ infarct healing
👉improved cardiac remodelling
⤵️ pulmonary oedema
⤵️ contractile dysfunction
12) Myeloid MRKO gives us insights into the key role of MR and inflammation and fibrosis. In a glomerulonephritis model, podocyte MRKO provided no kidney protection.
13) However myeloid MKRO led to
⤵️ proteinuria
⤵️ cardiac hypertrophy
⤵️ fibrosis
⤵️ inflammation
⤵️ endothelial sodium channel circuits
⤵️ proteinuria
⤵️ cardiac hypertrophy
⤵️ fibrosis
⤵️ inflammation
⤵️ endothelial sodium channel circuits
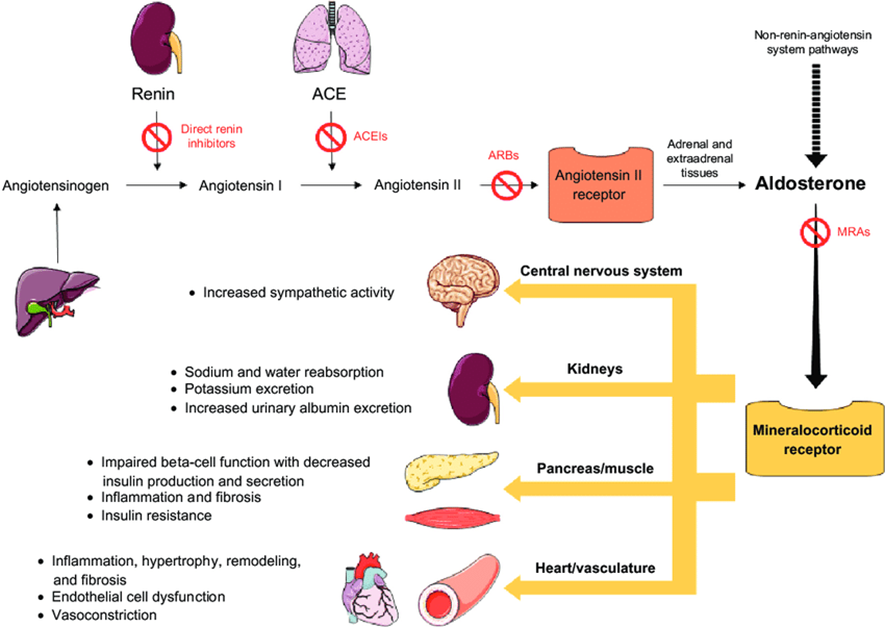
14) This leads to aldosterone driving physiological MR activity in those tissues, whereas in the cardiomyocytes cortisol is also a major active MR ligand. Long-term use of ACEi/ARBs use in #heartfailure, #CKD or #hypertension can lead to “aldosterone breakthrough’ ...
15) ... due to incomplete suppression of serum aldosterone levels that may also worsen MR overstimulation.
nature.com/articles/ncpne…
The image below summarises the downstream effects of MR activation
🔓doi.org/10.2147/VHRM.S…
nature.com/articles/ncpne…
The image below summarises the downstream effects of MR activation
🔓doi.org/10.2147/VHRM.S…
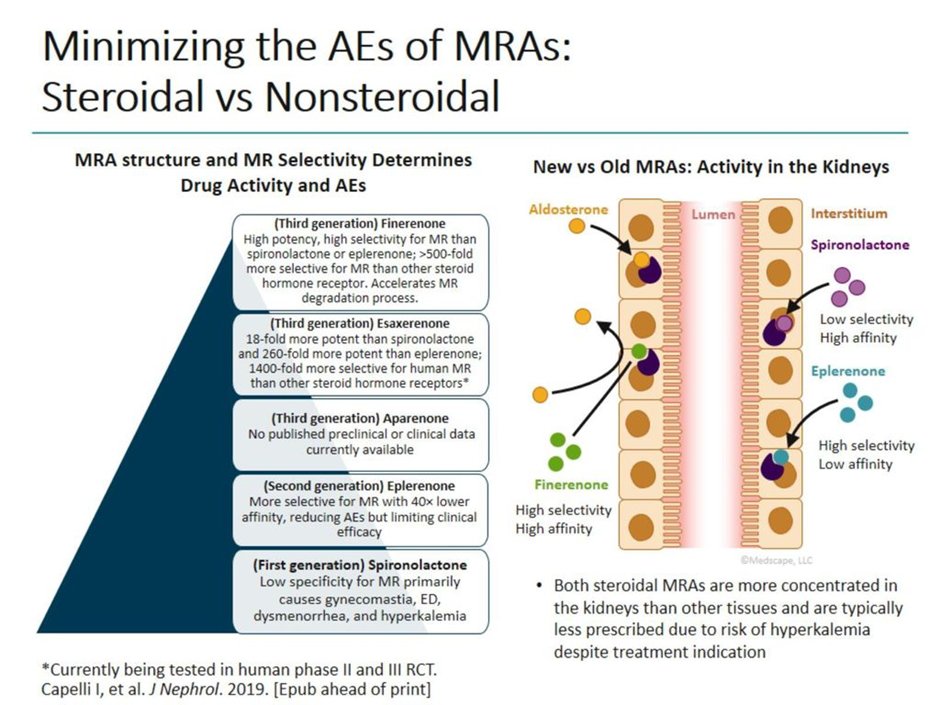
16) Next up: comparisons of the commercially available MRA’s. MRA’s differ significantly in chemical structure, which in term drives significant differences in their clinical utility. 1st & 2nd generation MRAs are steroidal, and not dissimilar to aldosterone.
17) 3rd generation MRA’s are non-steroidal and belong to the dihydropyridine chemical class.
👉1st generation MRAs = #spironolactone & #canrenone
👉2nd generation MRA = #eplerenone
👉3rd generation MRA = #finerenone & #esaxerenone
👉1st generation MRAs = #spironolactone & #canrenone
👉2nd generation MRA = #eplerenone
👉3rd generation MRA = #finerenone & #esaxerenone


18) Return tomorrow for more education from @GoggleDocs principal @drpatrickholmes and your link to grab 0.5h CE/#CME on options for #MRA! Nods to @drkevinfernando @HannahBeba @AmarPut @edgarvlermamd @ChristosArgyrop @sophia_kidney @nephondemand @dguerrot @goKDIGO
CORRECTION: Which of those is NOT a potential unwanted effect of spironolactone?
@cardiomet_ce apologizes for the confusion!
@cardiomet_ce apologizes for the confusion!
19a) Welcome back! You're differentiating among mineralocorticoid receptor antagonists #MRAs with expert faculty @drpatrickholmes. Follow this thread to your CE/#CME! Tip my hat to @parthaskar @kamleshkhunti @DiabetesUK @drpratikc @docwas @AliRacaniere @DSNforumUK @profmjdavies
19b) & profuse apologies from the vast @ckd_ce home office for the posting error in tweet 4. Many of you realized that we had left out the “NOT” in the❓, but the point is that steroidal #MRAs are assoc'd w/gynecomastia/mastodynia, impotence/⬇️libido, hypotension & HYPERkalemia.
20) For the rest of the tweetorial I have focused on the 2 most widely used steroidal MRAs (spironolactone & eplerenone) & the only 2 commercially available non-steroidal MRAs (finerenone & esaxerenone). Below is a summary of the key pharmacodynamic & pharmacokinetic data.
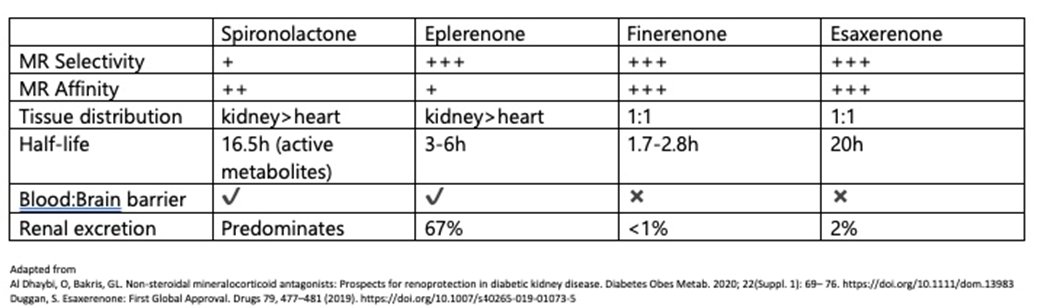
21) Re the importance of MR selectivity: spironolactone’s lack of selectivity for the MR, w/ binding to both progesterone & androgen receptors. leads to gynecomastia (10x⤴️in RALES).
Eplerenone, finerenone & esaxerenone in RCTs had similar rates of gynecomastia to placebo.
Eplerenone, finerenone & esaxerenone in RCTs had similar rates of gynecomastia to placebo.
22) Renal tissue selectivity, high renal excretion, high MR affinity & long half-life all likely drive risk of hyperkalaemia (🔓academic.oup.com/eurheartj/arti…).
👉Hyperkalaemia rates spironolactone > eplerenone
👉Rates steroidal MRAs > non-steroidal MRAs
👉Risks⤴️ as kidney function⤵️
👉Hyperkalaemia rates spironolactone > eplerenone
👉Rates steroidal MRAs > non-steroidal MRAs
👉Risks⤴️ as kidney function⤵️
23) So what about impact on blood pressure ⁉️
Spironolactone is thought to ⤵️BP than other MRAs.(link.springer.com/article/10.100…)
Eplerenone ⤵️BP more than finerenone (🔓academic.oup.com/eurheartj/arti…)
whereas eplerenone has a similar impact on BP as esaxerenone (🔓ahajournals.org/doi/full/10.11…)
Spironolactone is thought to ⤵️BP than other MRAs.(link.springer.com/article/10.100…)
Eplerenone ⤵️BP more than finerenone (🔓academic.oup.com/eurheartj/arti…)
whereas eplerenone has a similar impact on BP as esaxerenone (🔓ahajournals.org/doi/full/10.11…)
24) Here at @CKD_ce we are keen to focus on the utility of MRAs in the treatment of #CKD. Due to the risk of hyperkalaemia, steroidal MRAs have a limited role in #CKD. Of the non-steroidal MRAs only finerenone is licensed for CKD in people with #type2diabetes (currently only 🇺🇸)

25) So let's leave you with a 3-part, rapid-fire knowledge check: first, which MRA has a 🇺🇸 license for the treatment of CKD in people with type 2 diabetes? Mark your answer before you scroll down!
26) The answer is c, #finerenone. 🇺🇸 approval for the treatment of adult patients with #CKD associated w/ #T2D was based on the results from the phase 3 FIDELIO-DKD trial (🔓nejm.org/doi/full/10.10…):


27) Second, what was the relative increased risk of hyperkalaemia with spironolactone in the RALES study compared to placebo?
28) In the RALES trial (🔓pubmed.ncbi.nlm.nih.gov/10471456/), hyperkalaemia was in fact seen🔟times more often in patients treated with spironolactone than with placebo, and serious hyperkaelemia occurred twice as often (choice d).
29) BTW, check out cardiometabolic-ce.com/category/hyper… for several opportunities to learn and earn CE/#CME on contemporary management of hyperkalemia, including facilitation of #RAASi.
30) Finally, finerenone is associated with what risk of developing gynaecomastia compared to placebo in the combined analysis of the FIGARO & FIDELITY trials?
31) The answer is: (b), about the same risk, removing the potential for a compliance problem for ♂️s who use steroidal #MRAs. See 🔓link.springer.com/article/10.118….
32) In summary, as per @AgarwalRajivMD, nonsteroidal MRAs appear to demonstrate a better benefit–risk ratio than steroidal MRAs, and given that overactivation of the MR leads to inflammation and fibrosis in cardiorenal disease, they represent an important advance!
33) And that's it--you have just earned 0.5h CE/#CME! Go to ckd-ce.com/MRA2 to claim your credit, and FOLLOW US for more education by #tweetorial, all FREE, all by EXPERT authors! I am @drpatrickholmes of @GoggleDocs. Be sure to follow @cardiomet_ce as well!
• • •
Missing some Tweet in this thread? You can try to
force a refresh




