An in-depth review of Terrible Triad Injuries.
If you're interested in orthopedics you won't want to miss this one!
1/12
If you're interested in orthopedics you won't want to miss this one!
1/12

Terrible triad injuries are complex posterior elbow dislocations associated with coronoid and radial head fractures as well as capsular and ligamentous injuries.
These injuries commonly result from a fall on an outstretched arm and the structures of the elbow fail from lateral to medial.
LCL --> anterior capsule --> MCL
LCL --> anterior capsule --> MCL

Contributions to elbow stability:
The radial head provides an anterior/valgus buttress, while the coronoid provides an anterior/varus buttress.
The LCL provides varus/posterolateral rotary stability, while the MCL provides valgus/posteromedial rotary stability.
The radial head provides an anterior/valgus buttress, while the coronoid provides an anterior/varus buttress.
The LCL provides varus/posterolateral rotary stability, while the MCL provides valgus/posteromedial rotary stability.
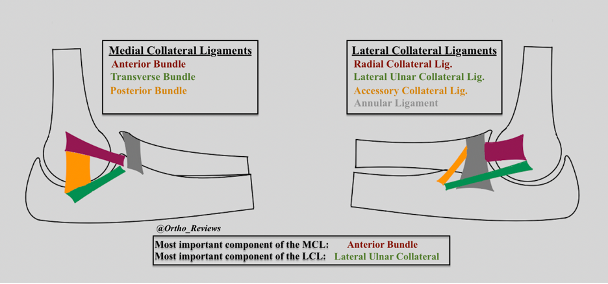
Which of the following is the most important component of the medial collateral ligament complex of the elbow?
Components of the LCL:
Ulnar Collateral Ligament **
Radial Collateral Ligament
Accessory Collateral Ligament
Annular Ligament
Components of MCL:
Anterior Bundle **
Posterior Bundle
Transverse Bundle
** Most important for Stability
Ulnar Collateral Ligament **
Radial Collateral Ligament
Accessory Collateral Ligament
Annular Ligament
Components of MCL:
Anterior Bundle **
Posterior Bundle
Transverse Bundle
** Most important for Stability
Morrey Classification System of coronoid fractures:
1: Coronoid tip avulsion
2: <50% of Coronoid
3: >50% of Coronoid
Type 1: most common in Terrible Triad.
Type 3: associated w/ posterolateral instability.
1: Coronoid tip avulsion
2: <50% of Coronoid
3: >50% of Coronoid
Type 1: most common in Terrible Triad.
Type 3: associated w/ posterolateral instability.

Mason Classification System of radial head fractures:
1: < 2mm displacement
2: > 2mm displacement
3: comminuted
4: fractures associated with elbow dislocation
1: < 2mm displacement
2: > 2mm displacement
3: comminuted
4: fractures associated with elbow dislocation

A step-wise approach is undertaken for surgical repair of terrible triad injuries.
1) ORIF vs radial head replacement
2) ORIF of coronoid if > 10% involved
3) Repair of the LCL
1) ORIF vs radial head replacement
2) ORIF of coronoid if > 10% involved
3) Repair of the LCL
After these three steps you should assess elbow stability under fluoro
If the elbow remains unstable consider repairing the MCL
If the elbow still remains unstable after repair of the MCL some may consider an internal fixator such as an IJS (shown below) or external fixation
If the elbow remains unstable consider repairing the MCL
If the elbow still remains unstable after repair of the MCL some may consider an internal fixator such as an IJS (shown below) or external fixation

Patients should be immobilized following surgery, with supervised motion beginning at the surgeon's preference.
Immobilization positioning:
MCL intact, LCL repaired: 90° in full pronation to reduce posterolateral instability
MCL and LCL repaired: 90° in neutral rotation.
Immobilization positioning:
MCL intact, LCL repaired: 90° in full pronation to reduce posterolateral instability
MCL and LCL repaired: 90° in neutral rotation.
Complications include:
✯ Continued instability
✯ Hardware failure
✯ Stiffness from immobilization
✯ Post-traumatic arthritis.
✯ Continued instability
✯ Hardware failure
✯ Stiffness from immobilization
✯ Post-traumatic arthritis.
If you enjoyed this review, please like or retweet to help the page grow and give us a follow!
Author: @CSMorford
#TerribleTriad #Elbow #Trauma #Ortho #Orthopedics #OrthoTwitter #Bones #Trauma #MedEd #MedicalEducation #MedTwitter #ERAS #MedStudent #Tweetorials #Radiology
Author: @CSMorford
#TerribleTriad #Elbow #Trauma #Ortho #Orthopedics #OrthoTwitter #Bones #Trauma #MedEd #MedicalEducation #MedTwitter #ERAS #MedStudent #Tweetorials #Radiology
• • •
Missing some Tweet in this thread? You can try to
force a refresh