
#TBTWebinar is back ‼️
🥼 @MPishvaian @BreastCancerMD1 @Latinamd @BenWestphalen
#CME🔗 bit.ly/3vdXBb4
Pretest 👉 bit.ly/3rYNZir
Claim credit 👉 bit.ly/3ljVVXM
Supported by AstraZeneca Pharmaceuticals & Daiichi Sankyo, Inc
twitter.com/i/broadcasts/1…
🥼 @MPishvaian @BreastCancerMD1 @Latinamd @BenWestphalen
#CME🔗 bit.ly/3vdXBb4
Pretest 👉 bit.ly/3rYNZir
Claim credit 👉 bit.ly/3ljVVXM
Supported by AstraZeneca Pharmaceuticals & Daiichi Sankyo, Inc
twitter.com/i/broadcasts/1…
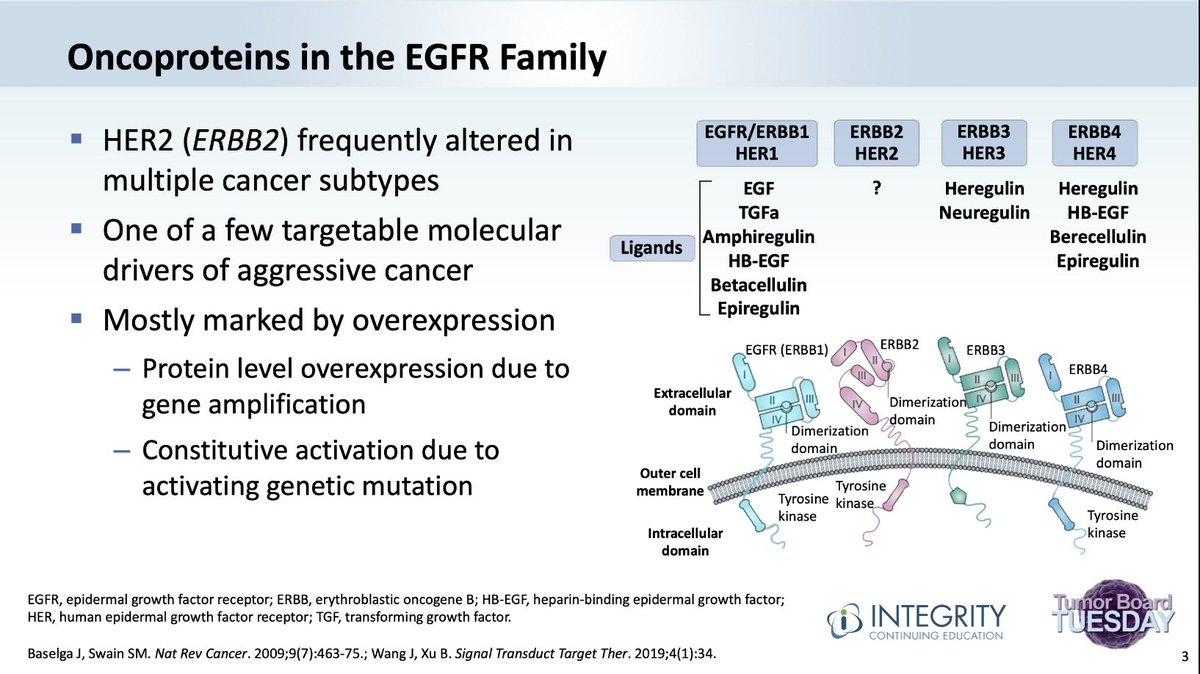
#TumorBoardTuesday HER2 #TBTWebinar 🔑
➡️HER2 activity requires receptor dimerization
✅HER1 = EGFR
✅HER3, HER4
➡️HER2 is frequently overexpressed in multiple cancers
✅Protein⬆️due to gene🧬 amplification
✅Constitutive activation due to activating🧬mutation
➡️HER2 activity requires receptor dimerization
✅HER1 = EGFR
✅HER3, HER4
➡️HER2 is frequently overexpressed in multiple cancers
✅Protein⬆️due to gene🧬 amplification
✅Constitutive activation due to activating🧬mutation
#TumorBoardTuesday HER2 #TBTWebinar 🔑
➡️HER2 (ERBB2) alterations occur in multiple cancer types
✅Breast Ca 25%
✅Gastric Ca 22%
✅GE jxn Ca 32%
✅CRC 5%
✅Lung Ca 6 to 30%
✅Biliary Ca 5 to 20%
🤔There is some disease specificity re: overexpression vs activating🧬mutation
➡️HER2 (ERBB2) alterations occur in multiple cancer types
✅Breast Ca 25%
✅Gastric Ca 22%
✅GE jxn Ca 32%
✅CRC 5%
✅Lung Ca 6 to 30%
✅Biliary Ca 5 to 20%
🤔There is some disease specificity re: overexpression vs activating🧬mutation

#TumorBoardTuesday HER2 #TBTWebinar 🔑
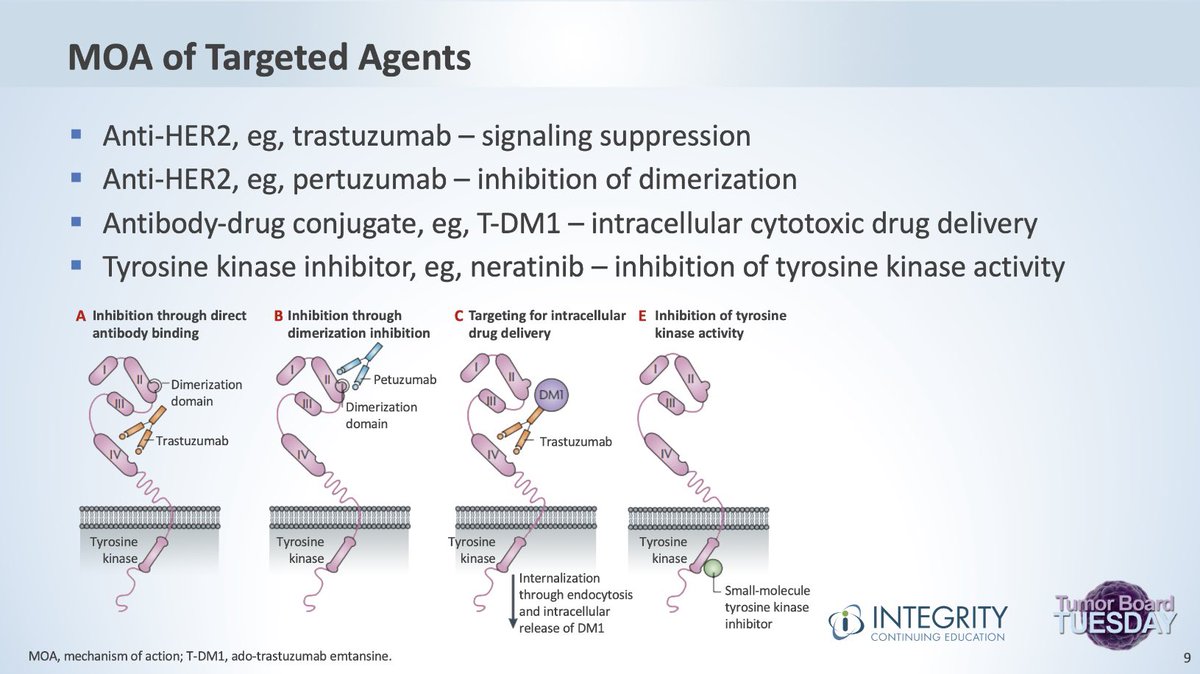
➡️MOA of Targeted Agents🎯
✅Anti-HER2, eg, trastuzumab🚫signaling
✅Anti-HER2, eg, pertuzumab🚫dimerization
✅Antibody-drug conjugate (ADC), eg,T-DM1 intracellular cytotoxic💊deliv
✅Tyrosine kinase (TK) inhibitor, eg, neratinib🚫activity
➡️MOA of Targeted Agents🎯
✅Anti-HER2, eg, trastuzumab🚫signaling
✅Anti-HER2, eg, pertuzumab🚫dimerization
✅Antibody-drug conjugate (ADC), eg,T-DM1 intracellular cytotoxic💊deliv
✅Tyrosine kinase (TK) inhibitor, eg, neratinib🚫activity
#TumorBoardTuesday HER2 #TBTWebinar 🔑
➡️There are many HER2 🎯 targeted agents
(Including trastuzumab, pertuzumab, and lapatinib)
➡️These are some of the newer agents
✅Trastuzumab emtansine (T-DM1)
✅Trastuzumab deruxtecan (T-DXd)
✅Margetuximab
✅Tucatinib
✅ARX788
➡️There are many HER2 🎯 targeted agents
(Including trastuzumab, pertuzumab, and lapatinib)
➡️These are some of the newer agents
✅Trastuzumab emtansine (T-DM1)
✅Trastuzumab deruxtecan (T-DXd)
✅Margetuximab
✅Tucatinib
✅ARX788

#TumorBoardTuesday HER2 #TBTWebinar 🔑
➡️Recent Ph3 trials of HER2🎯Tx in breast Ca
➡️DESTINY-Breast03
✅T-DXd v T-DM1
👉ORR 79% v 34%
👉12 mo OS 94% v 86% P=.007
➡️SOPHIA
✅Margetux+chemo v trastuz+chemo
👉ORR: 25% v 14%
👉mPFS: 5.7 v 4.4 mos P=.001
pubmed.ncbi.nlm.nih.gov/33480963/
➡️Recent Ph3 trials of HER2🎯Tx in breast Ca
➡️DESTINY-Breast03
✅T-DXd v T-DM1
👉ORR 79% v 34%
👉12 mo OS 94% v 86% P=.007
➡️SOPHIA
✅Margetux+chemo v trastuz+chemo
👉ORR: 25% v 14%
👉mPFS: 5.7 v 4.4 mos P=.001
pubmed.ncbi.nlm.nih.gov/33480963/

#TumorBoardTuesday HER2 #TBTWebinar 🔑
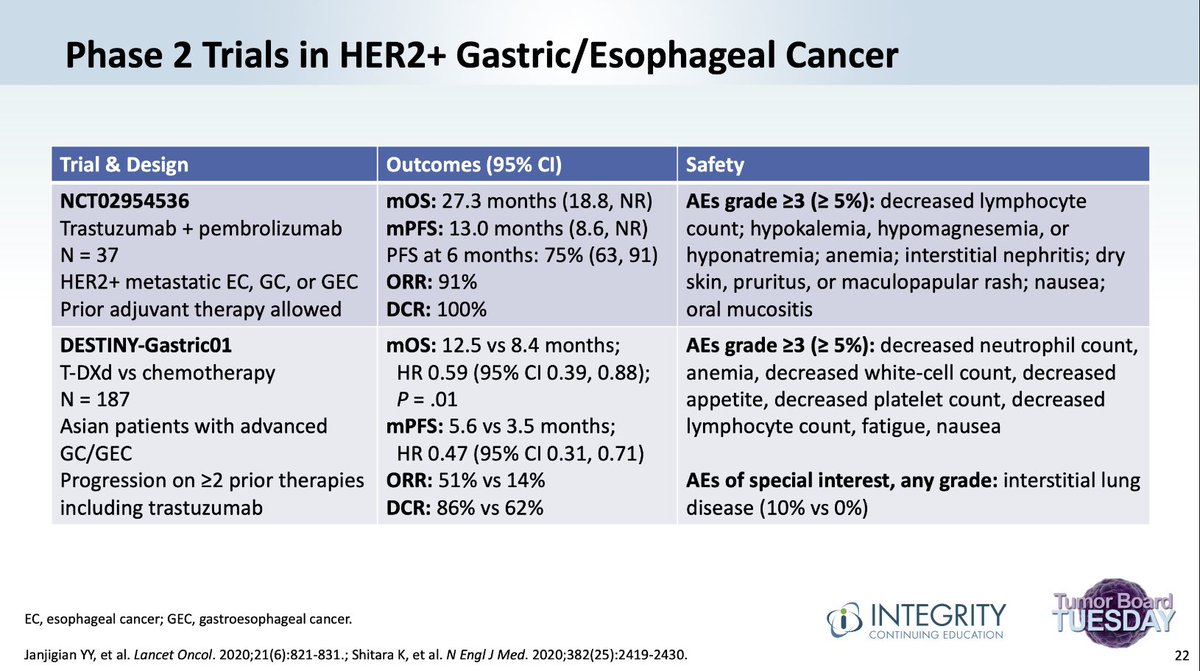
➡️Key Ph2 trials of HER2🎯Tx in Gastric/Esoph Ca
➡️My Pathway
✅Trastuzumab + pembrolizumab
👉ORR 91%‼️
👉mOS 27 mos
➡️DESTINY-Gastric01
✅T-DXd vs chemotherapy
👉ORR: 51% vs 14%
👉mOS: 13 v 8 mos P=.01
pubmed.ncbi.nlm.nih.gov/32469182/
➡️Key Ph2 trials of HER2🎯Tx in Gastric/Esoph Ca
➡️My Pathway
✅Trastuzumab + pembrolizumab
👉ORR 91%‼️
👉mOS 27 mos
➡️DESTINY-Gastric01
✅T-DXd vs chemotherapy
👉ORR: 51% vs 14%
👉mOS: 13 v 8 mos P=.01
pubmed.ncbi.nlm.nih.gov/32469182/
#TumorBoardTuesday HER2 #TBTWebinar 🔑
➡️Key Ph2 trials of HER2🎯Tx in #CRC
➡️HERACLES
✅Trastuz+lapat
👉ORR 30%
➡️MyPathway🛣
✅Trastuz+Pertuz
👉ORR 32%
➡️MOUNTAINEER🏔
✅Trastuz+Tucatinib
👉ORR 55%
➡️DESTINY-CRC01
✅Trastuzumab deruxtecan
👉ORR 45%
pubmed.ncbi.nlm.nih.gov/33961795/
➡️Key Ph2 trials of HER2🎯Tx in #CRC
➡️HERACLES
✅Trastuz+lapat
👉ORR 30%
➡️MyPathway🛣
✅Trastuz+Pertuz
👉ORR 32%
➡️MOUNTAINEER🏔
✅Trastuz+Tucatinib
👉ORR 55%
➡️DESTINY-CRC01
✅Trastuzumab deruxtecan
👉ORR 45%
pubmed.ncbi.nlm.nih.gov/33961795/

#TumorBoardTuesday HER2 #TBTWebinar 🔑
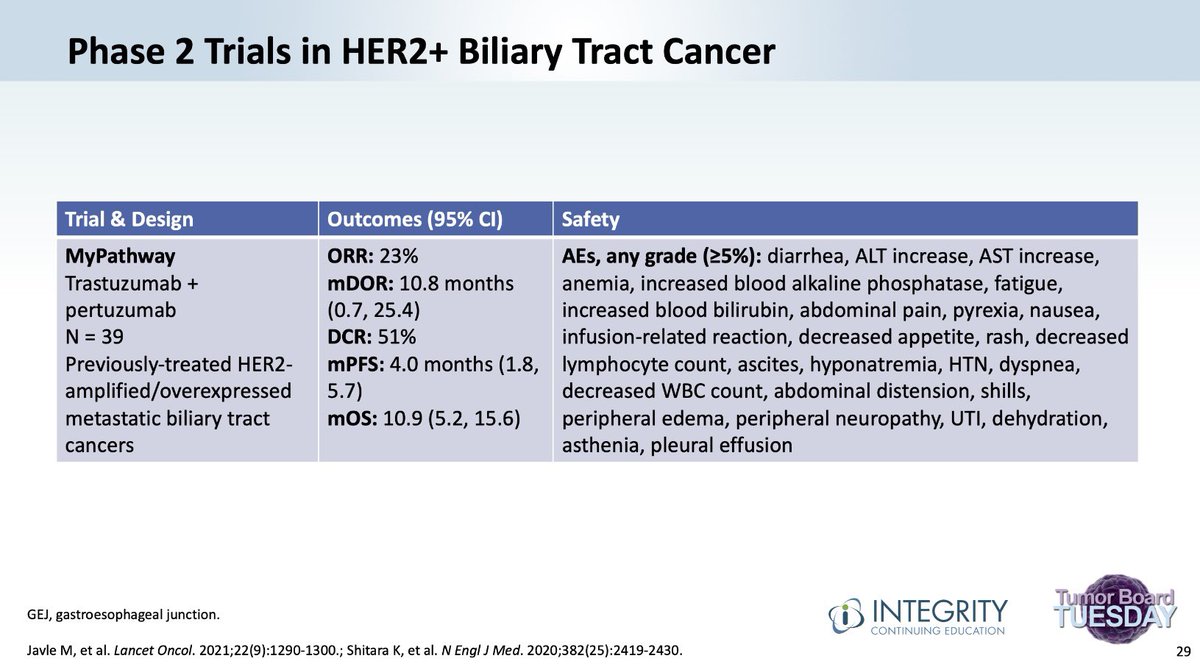
Ph2 trial of HER2🎯Tx in Biliary cancer
➡️MyPathway
✅Trastuzumab + Pertuzumab
👉ORR 23%
pubmed.ncbi.nlm.nih.gov/34339623/
Ph2 trial of HER2🎯Tx in Biliary cancer
➡️MyPathway
✅Trastuzumab + Pertuzumab
👉ORR 23%
pubmed.ncbi.nlm.nih.gov/34339623/
#TumorBoardTuesday HER2 #TBTWebinar 🔑
➡️Ph2 trials of HER2🎯Tx in Lung cancer🫁
➡️Basket trial 🧺
✅Trastuzumab emtansine
👉ORR 44%
➡️DESTINY-Lung01 🫁
✅Trastuzumab deruxtecan
👉ORR 55%
👉DCR 92%
👉mOS 17.8 mos
pubmed.ncbi.nlm.nih.gov/34534430/
➡️Ph2 trials of HER2🎯Tx in Lung cancer🫁
➡️Basket trial 🧺
✅Trastuzumab emtansine
👉ORR 44%
➡️DESTINY-Lung01 🫁
✅Trastuzumab deruxtecan
👉ORR 55%
👉DCR 92%
👉mOS 17.8 mos
pubmed.ncbi.nlm.nih.gov/34534430/

#TumorBoardTuesday HER2 #TBTWebinar 🔑
Ph2 trial of HER2🎯Tx in Salivary cancer
➡️MyPathway
✅Trastuzumab + Pertuzumab
👉ORR 60%
pubmed.ncbi.nlm.nih.gov/32067683/
Ph2 trial of HER2🎯Tx in Salivary cancer
➡️MyPathway
✅Trastuzumab + Pertuzumab
👉ORR 60%
pubmed.ncbi.nlm.nih.gov/32067683/

#TumorBoardTuesday HER2 #TBTWebinar 🔑
🔑Take home🏡points:
➡️HER2 is overexpressed/activated in many cancers
👉Worse prognosis
HER2🎯Tx has made a major impact:
✅Breast Ca
✅Gastric/GEJ Ca
✅CRC
✅Lung Ca
✅Biliary Ca
✅Salivary Ca
Several🗝️Ph3 trials in motion
🔑Take home🏡points:
➡️HER2 is overexpressed/activated in many cancers
👉Worse prognosis
HER2🎯Tx has made a major impact:
✅Breast Ca
✅Gastric/GEJ Ca
✅CRC
✅Lung Ca
✅Biliary Ca
✅Salivary Ca
Several🗝️Ph3 trials in motion

HER2 #TBTWebinar #OncTwitter
🙏for joining #TumorBoardTuesday HER2/3 series❗️
🙏#EmanuelPetricoin @PancPathologist @ErikaHamilton9 @BreastCancerMD1 @Latinamd @BenWestphalen @MPishvaian for being our experts‼️
🆓HER2🧬Resources 👉integrityce.com/HER2resources
🙏for joining #TumorBoardTuesday HER2/3 series❗️
🙏#EmanuelPetricoin @PancPathologist @ErikaHamilton9 @BreastCancerMD1 @Latinamd @BenWestphalen @MPishvaian for being our experts‼️
🆓HER2🧬Resources 👉integrityce.com/HER2resources
HER2 #TBTWebinar #OncTwitter #PancreaticCancer
Our next #TumorBoardTuesday discussion details:
🗓𝙉𝙀𝙓𝙏 𝙒𝙀𝙀𝙆 03/01/22
👨🏽⚕️@nanudasmd talks #PanCan NETs
📱Right here on our feed!!
Our next #TumorBoardTuesday discussion details:
🗓𝙉𝙀𝙓𝙏 𝙒𝙀𝙀𝙆 03/01/22
👨🏽⚕️@nanudasmd talks #PanCan NETs
📱Right here on our feed!!

• • •
Missing some Tweet in this thread? You can try to
force a refresh






