
We haven't done a HIIT-related thread in a while, but today I was inspired by this new meta-analysis on Sprint Interval Training (SIT), so here we go. I will teach you how you too can say incredible, mind-bending things and get them past the reviewers (in Frontiers, but still...) 

What did the meta find? (1) The worst you'll feel during SIT does not differ from the worst you'll feel during moderate-intensity continuous exercise (MICE), and (2) enjoyment of SIT and MICE does not differ.

Now, you don't need to be an expert to understand that these claims are made up and patently false. Anyone who has done a Wingate test knows that this is one of the most brutal, most violently unpleasant physical experiences, so imagine doing several of these back-to-back.
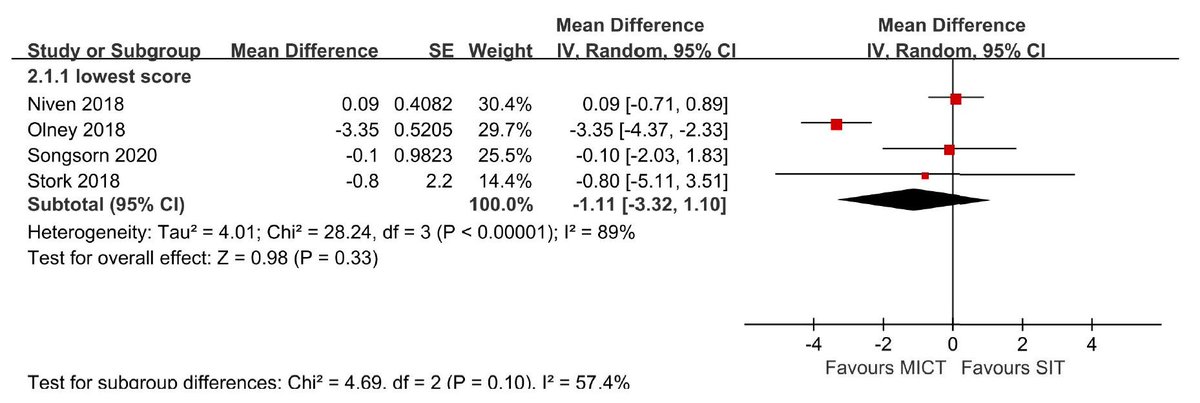
Yet, here are the data -- and you can't argue with data, can you? As you can see, the diamond crosses the zero line, indicating no difference between SIT and moderate-intensity continuous exercise for the worst feeling during exercise! How is this possible? Stick around, kids.
The first thing you have to do is start giving new meanings to words. Like "sprint" does not really mean "sprint," "high intensity" does not really mean "high intensity," and so on. It's a little Orwellian but it works when your readers are gullible or share your agenda.
So, what is "legit" SIT? Depends on who you ask and when you ask them. What argument are they trying to make at the time? One of the tricks of this business is that you have to learn to speak from both sides of your mouth -- while keeping a straight face. It ain't easy.
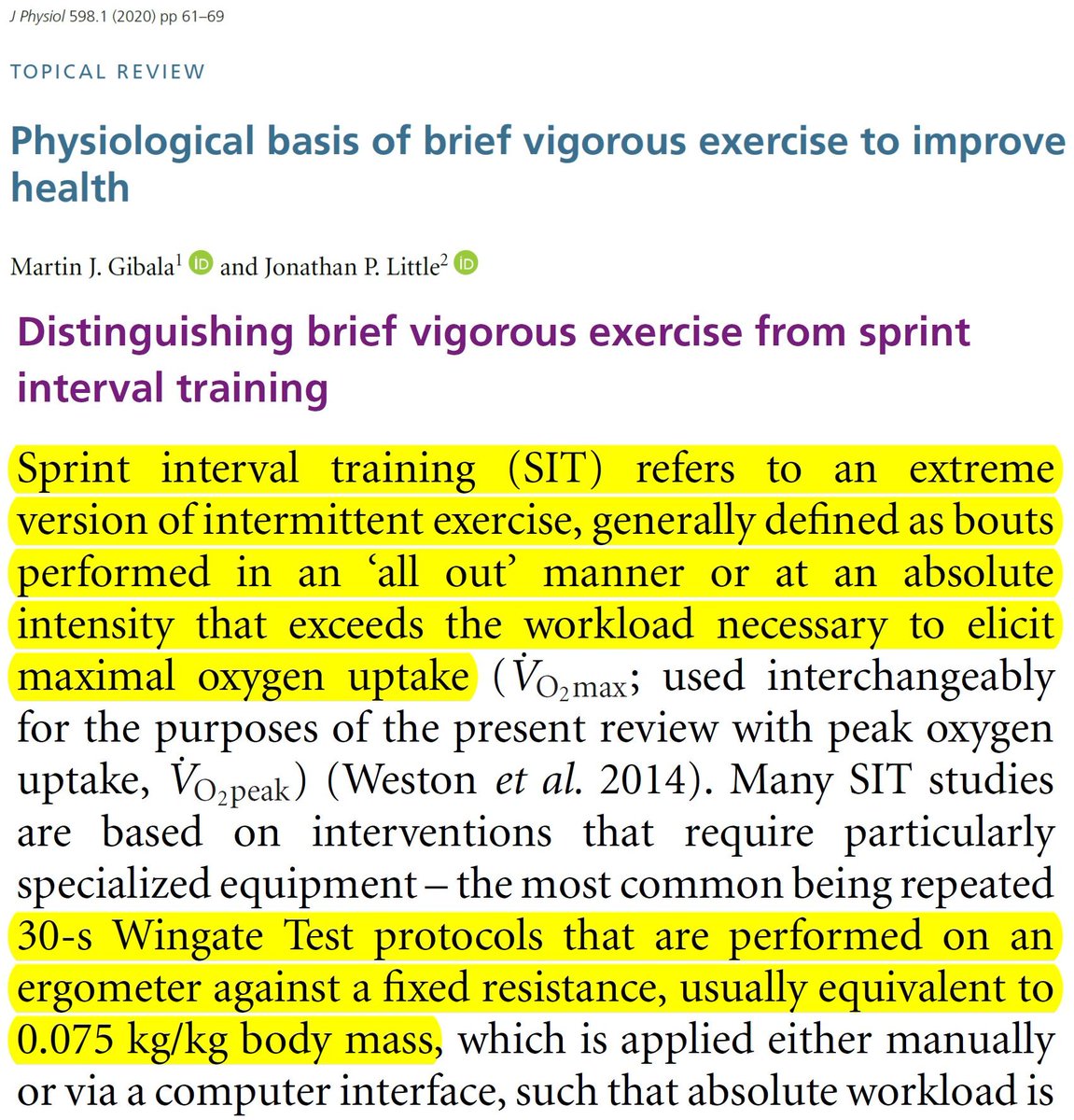
If you want to convince your readers that SIT is physiologically effective, you say that SIT involves "all out" effort, and a workload that exceeds the workload associated with VO2max. And a good example of SIT is a Wingate test (30s against resistance of 7.5% of body weight).

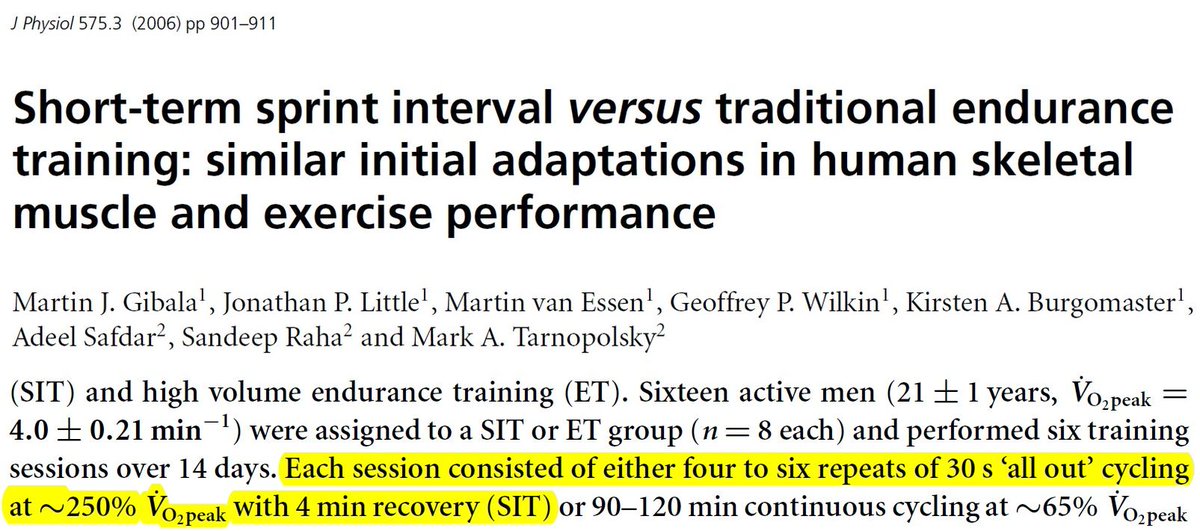
For example, when you want to be certain you'll find physiological adaptations, you set a workload to the equivalent of 250% of VO2peak. And you forget to mention anything about adverse events, like nausea, lightheadedness, or vomiting.
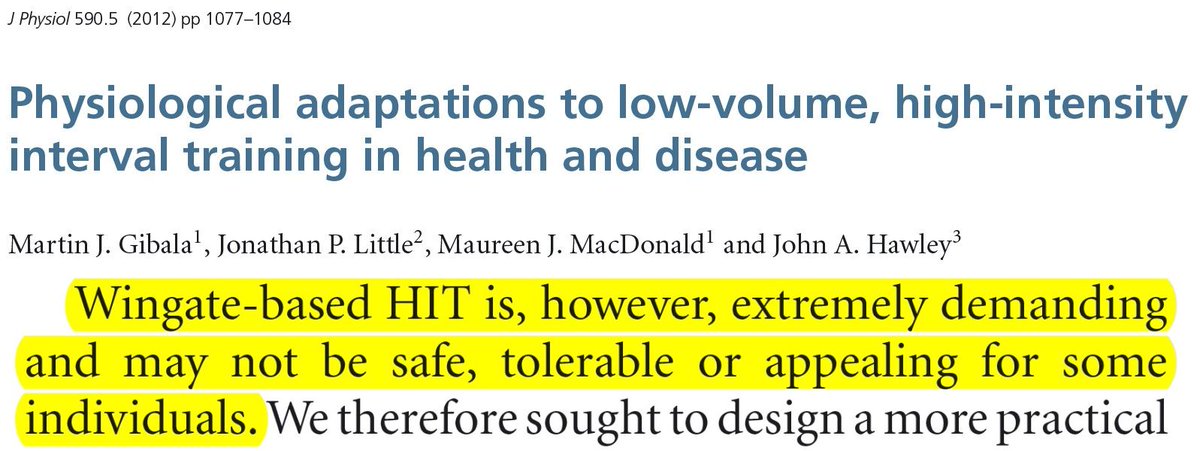
But obviously you know that average people can't do this stuff without barfing or passing out. And when you're in the right frame of mind, you may even admit it publicly. "SIT" per se is not safe, tolerable, or appealing / sustainable in "real life."
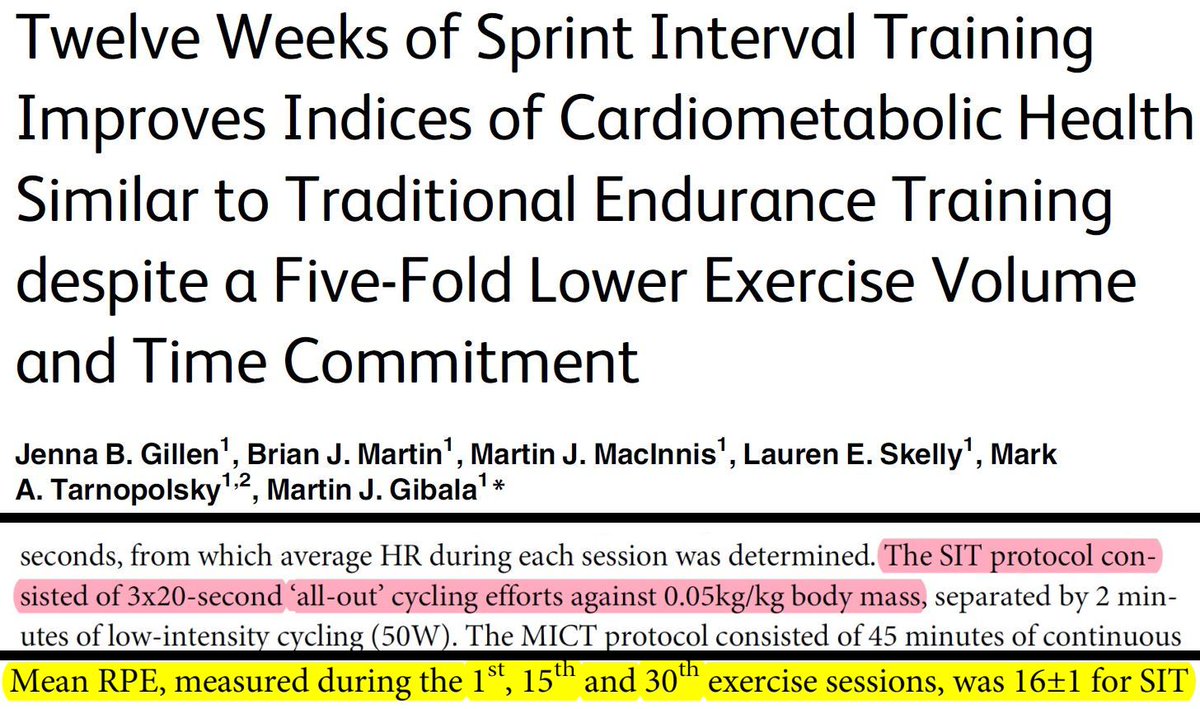
So, now you have to start making up stuff. You say that "SIT" is no longer "SIT," it's something kinder and gentler. So, you reduce the duration of each interval to 20 sec and the resistance to 5% of body weight. This brings "SIT" down to the "vigorous" range (RPE 14-17 by ACSM).
This is because you know one simple but important thing: even if your intensity is "all out," physiological intensity (e.g., VO2) can't rise to 90-100% in 20-30 seconds.
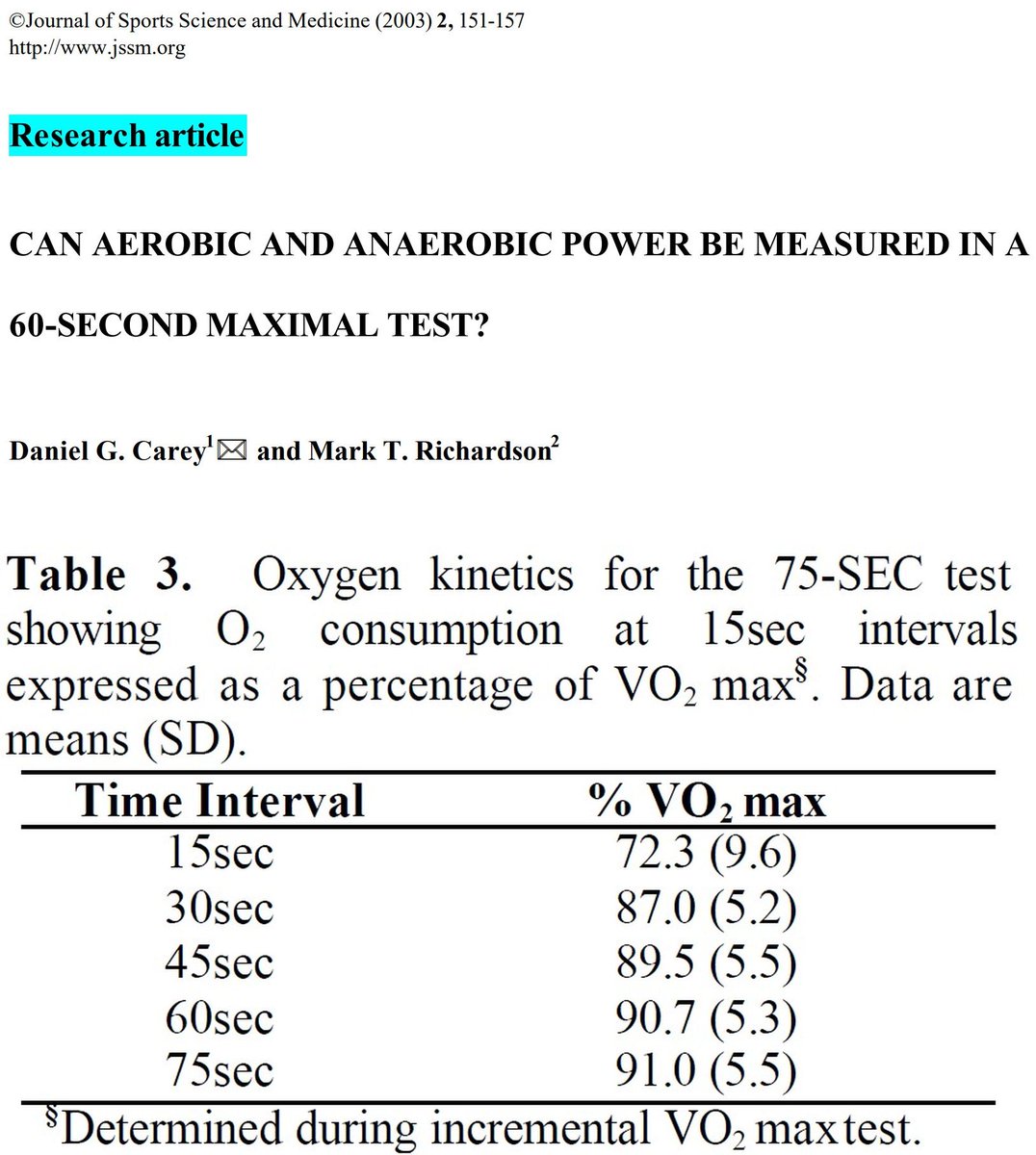
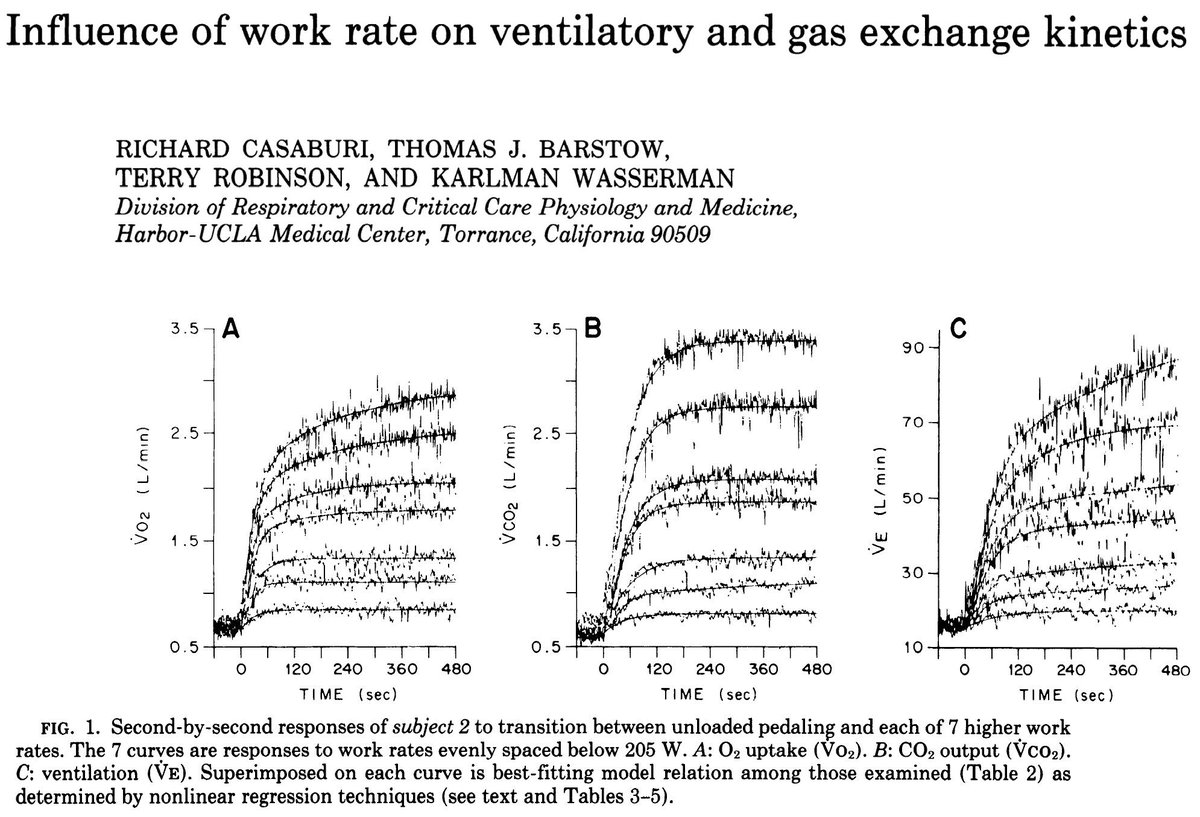
Exercise physiologists know about the dynamics of physiological parameters, such as VO2, at the onset of severe exercise. Even if the workload increases in square-wave fashion, physiological parameters take several seconds of minutes to rise to meet the demand.
One thing we learned from Tabata is that, if you want to reach ~100% VO2peak within a short period (e.g., 20 sec), you need to set the workload to a level that corresponds to 170% VO2peak.
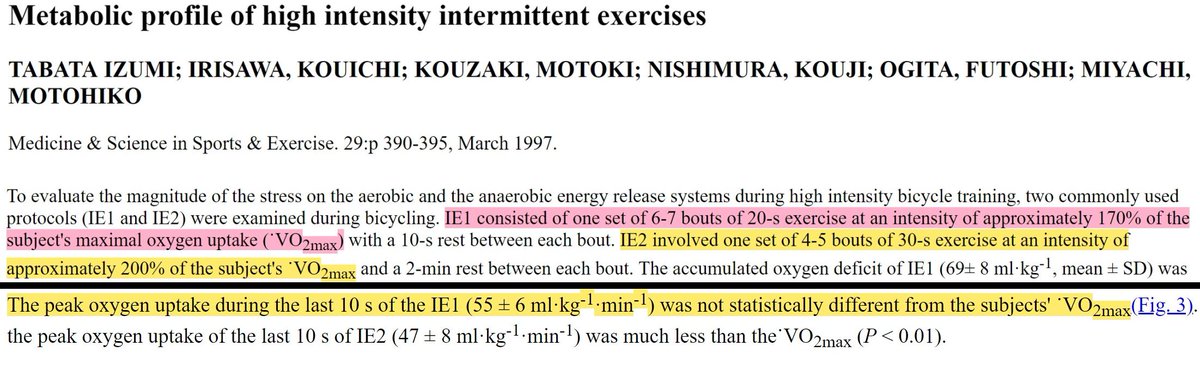
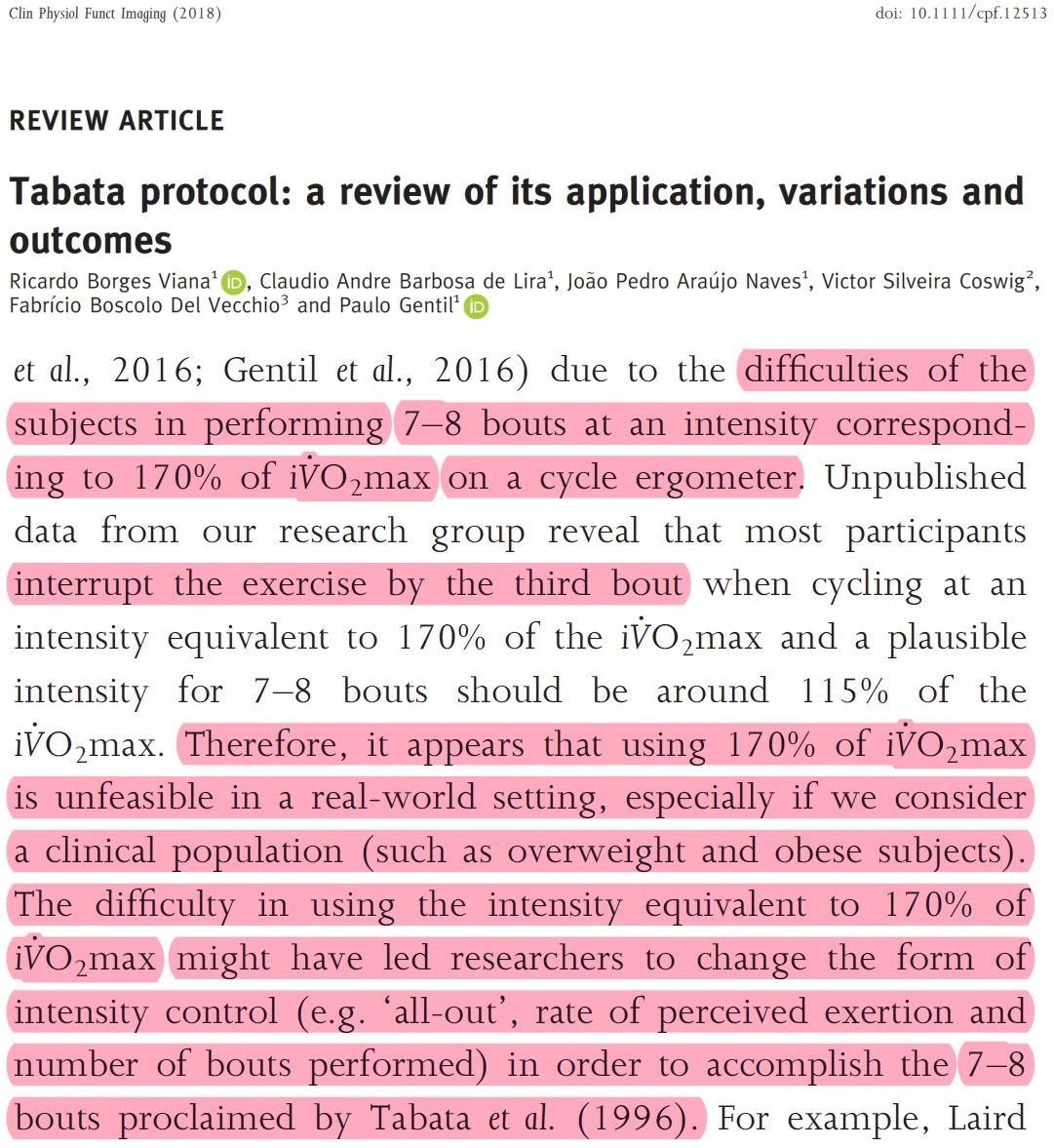
The problem, of course, is that even young and athletic participants cannot finish more than 2 of these 20-sec intervals at a workload corresponding to 170% VO2peak. I guess only Japanese exercise-science students can do 7-8 intervals, but no one else.
So, let's return to the studies that allegedly showed that doing SIT does not make you feel any worse than doing moderate-intensity continuous exercise... and let's look at only a couple of their tricks: (a) intensity and (b) timing of affect assessments. Are you ready?
You will notice 2 things. (1) None of the studies tested "SIT" but rather various shortened or lighter versions of doubtful physiological effectiveness. (2) Affect was assessed during recovery, NOT during the high-intensity intervals, in an effort to capture the "relief" effect.
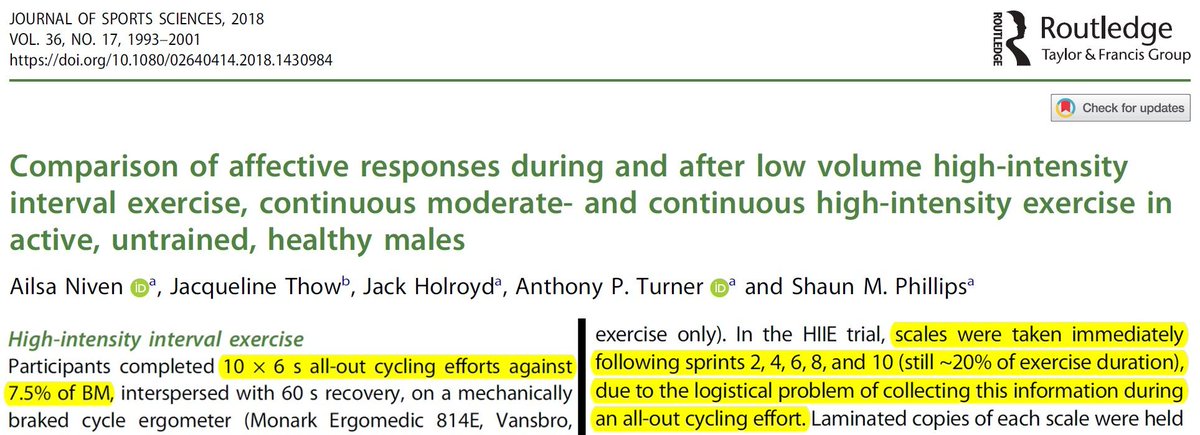
Look. Niven et al. (2018) had 6-sec intervals and asked participants how they felt only AFTER the intervals were over and participants were in recovery.
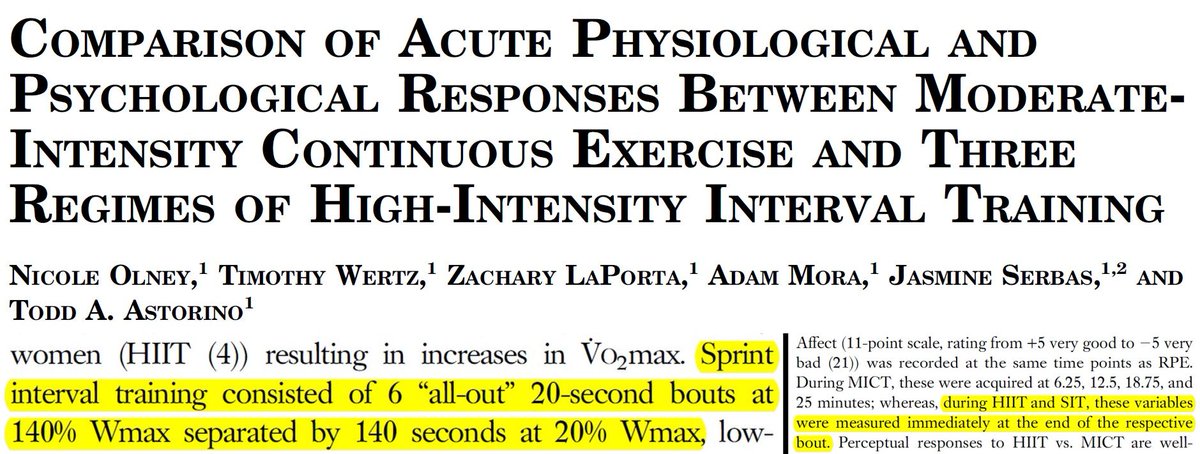
Olney et al. (2018) had 20-sec intervals and asked participants how they felt -- you guessed it -- only AFTER the intervals were over and participants were in recovery.
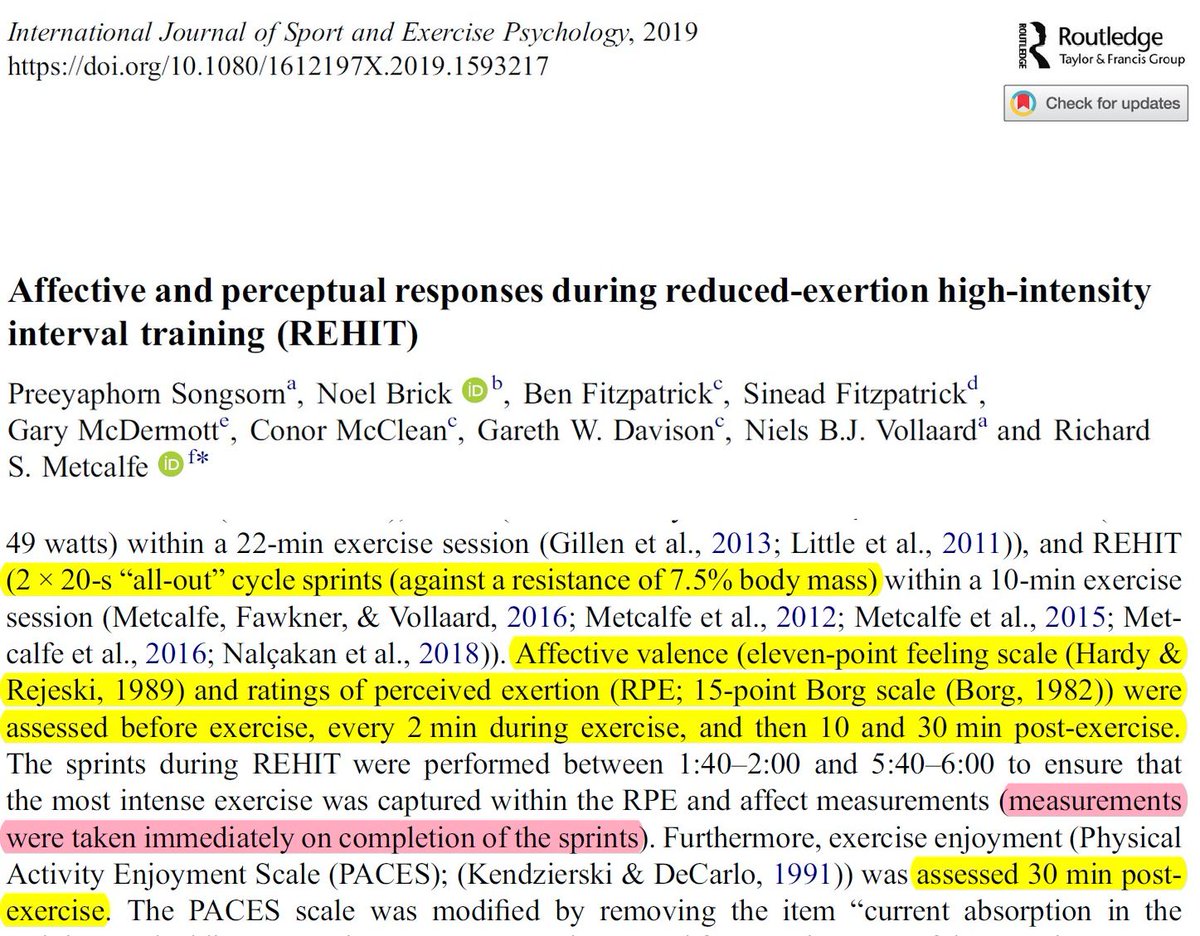
Songsorn et al. (2020) had 20-sec intervals and asked participants how they felt -- you guessed it -- only AFTER the intervals were over and participants were in recovery.
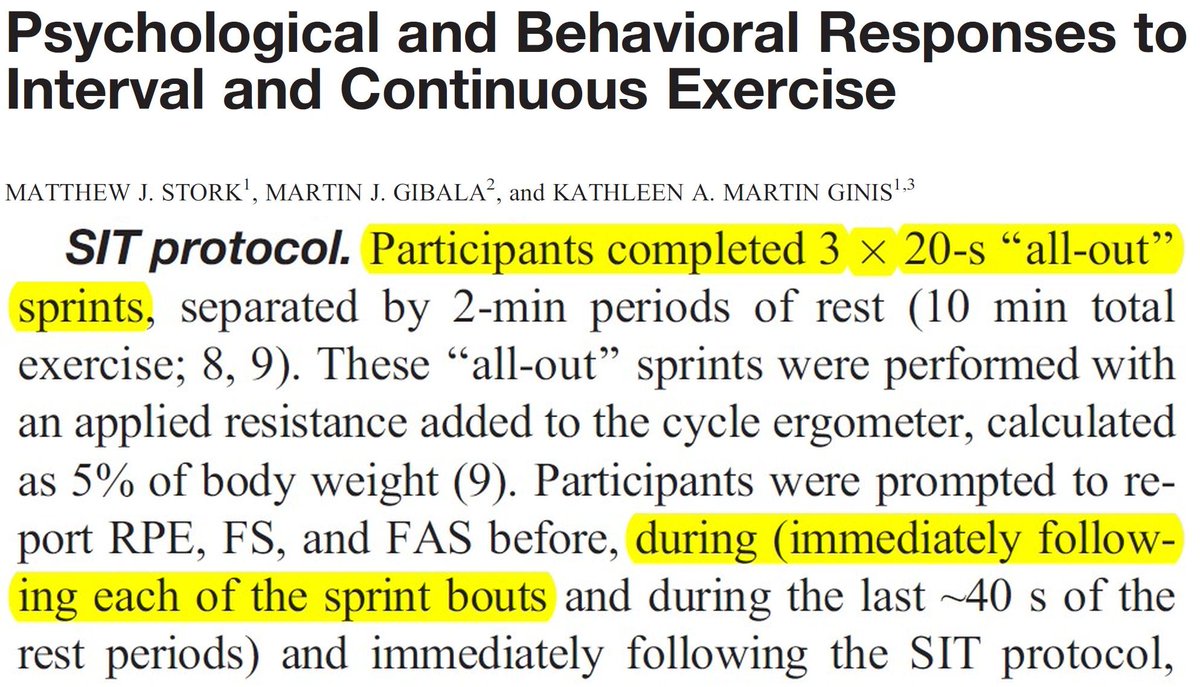
Stork et al. (2018) had 20-sec intervals and asked participants how they felt -- you guessed it -- only AFTER the intervals were over and participants were in recovery.
To recap: if you want to show that SIT and moderate-intensity exercise feel about the same, remember: (1) don't use "SIT" but something short that barely raises physiological intensity to vigorous level for a few seconds, and (2) ask people how they feel only AFTER they're done.
OK, enough for now. Some other day, I will show you how you can find that enjoyment is about the same after SIT and moderate exercise. Enjoyment has its own little tricks. Lots of "fun" (pun intended).
• • •
Missing some Tweet in this thread? You can try to
force a refresh













