I hope @jburnmurdoch doesn't mind a QT, but re his article on SARS vs 'flu IFR - imo, a good thread as per, but some folks insist on just reading headlines...
My take? Well, the comparison has issues, many that John covers, but my main thought is:
My take? Well, the comparison has issues, many that John covers, but my main thought is:
https://twitter.com/jburnmurdoch/status/1502240909244649480?s=20&t=6ZzlpDYf8nghqMAkKAMajg
Just look at what vaccines might achieve if they were part of a supported, multi-layered approach, rather than being left to tackle COVID alone...
First, let's deal with the comparisons. John rightly mentions multiple caveats such as the fact that seasonal flu waves last just a few months, and that, critically, at present SARS2 prevalence is VERY high (and going up), yet flu is
only just creeping back as we increase mixing and relax the mitigations that have held the inherently high R0 of SARS2 in check - these effectively almost eliminated influenza spread in the past couple of years.
Flu is seasonal, because it is an endemic infection that we as a
Flu is seasonal, because it is an endemic infection that we as a
population have developed immunity to over hundreds of years. There are variances and differences in immunity for variations in flu strains, and sometimes we have bad years when the vaccine isn't the best match. Nobody should underestimate the impact of influenza, or indeed other
respiratory viruses and/or bacterial pneumonia. They remain huge health burdens. In fact, as @chrischirp pointed out in her recent article in @ScienceMagazine we could do far better at controlling these infections based upon our pandemic experience.
I realise that John has had
I realise that John has had
grief over the article, and it is important to remember that journalists don't generally choose headlines, so it's a shame that responses have been extreme.
However, I do feel that the comparison to seasonal flu remains difficult. As above, SARS2 is highly prevalent, and has been
However, I do feel that the comparison to seasonal flu remains difficult. As above, SARS2 is highly prevalent, and has been
and will continue to be so for the foreseeable. Thus, we need to factor time, R0 and IFR when calculating the clinical impact.
What was very clear from the data was a drop in IFR coincident with the Omicron wave. This is partly due to the VERY high number of infections, plus a
What was very clear from the data was a drop in IFR coincident with the Omicron wave. This is partly due to the VERY high number of infections, plus a
reduction in severity compared to delta WITHIN A VACCINATED/IMMUNE POPULATION. Anyone maintaining that BA1 or BA2 is inherently "mild" should take a look at the US and esp Hong Kong where boosters/vaccine coverage aren't as good as here.
This is a key point for me, yes, the IFR
This is a key point for me, yes, the IFR
has dropped cf seasonal flu during the omicron wave, but consider the populations we're discussing. Flu vax uptake is generally poor, whereas the vaccine and booster programmes vs SARS2 in the UK have been VERY good by comparison, covering nearly all those that might succumb to
severe disease. As such, to borrow from a nice analogy from @adsquires, not only are we talking about shooting bullets from a sniper rifle vs a machine gun, the SARS2 bullets are also trying to penetrate combat armour vs a woolly jumper. Still, this is a consequence of a very
good vax programme, so we're OK making this comparison, right? Well, certainly NOT on a world stage. But on the UK side, we're again about to embark upon another round of boosters in the coming weeks. Immunity against infection is waning at a considerable rate, but why is this an
issue when the vaccines have weakened the link between infection and severe disease? Well, for many people, it may not be, but as we're genetically diverse there will always be people that make a suboptimal response to the vaccines, and this doesn't "just" involve the vulnerable.
So, the risk is that allowing further waves without boosting means that the increases in hospitalisations and deaths we are seeing with omicron, and indeed with future variants, will be even worse, simply because the small chance of things going wrong is amplified by the sheer
number of infections. Absolute numbers count, we're still seeing hundreds dying every week in spite of our privileged position being able to provide so many boosters. In fact, as @danielgoyal mentioned in an excellent thread today, one of the main takeaways from the @FT article
is that vaccines underpin the vast majority of the IFR drop we've seen in the UK...so-called "natural infection", not so...sorry GBD/HART/U4T/CRG etc...and yet we prevaricate over "non-urgent" kids vax, and something like 17M people in the UK remain unvaccinated...a little unwise
putting all eggs in one basket, perhaps? I'm 100% for pushing vax across the board, and I'm sick of the mixed messaging we keep hearing, all it does is fuel the sorts of folks that message me with VAERS "data" every week🤦♂️
So, I hear the clarion call of "we don't test for flu (we
So, I hear the clarion call of "we don't test for flu (we
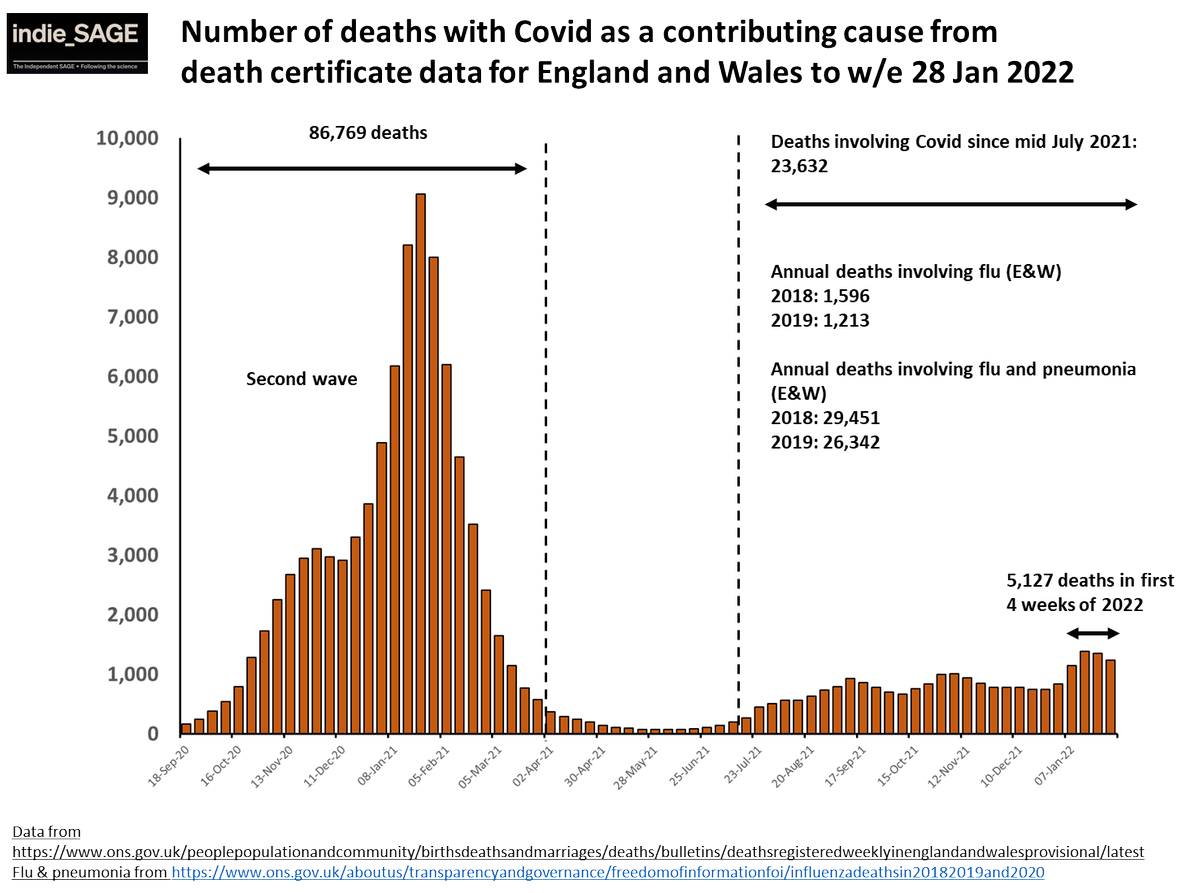
very much do, actually, just not en masse), and it kills just as many as COVID (erm, no, as John says), and the IFR is the same...well, actually, and this is NOT meant to detract from the clinical impact of flu, but the number of deaths with flu on the death certificate (as per
COVID) is far less than the figure quoted by the article (see Dan's thread again). There are good reasons for this, mainly because the correct comparator for pandemic, emergent SARS2 would be a pandemic emergent influenza with inherently high virulence and transmissibility...the
likes of which we haven't really seen in just over a century. I get why a comparison is useful to help people relate, but as I said in reply to John's thread, the headline and initial stance of the article will sadly be twisted by those for whom it provides (false) legitimacy, or
, and perhaps worse, enters into the common consciousness to fuel the collective UK COVID amnesia that's being pushed by those in power... ignorance is bliss, I guess.
Anyway. Back to why I think we need to take this as positive reinforcement of our vaccines, but also to use them in a much better way...
Well, Dan beat me to highlighting John's graph, but here it is again...
Well, Dan beat me to highlighting John's graph, but here it is again...
https://twitter.com/jburnmurdoch/status/1501886446415847427?s=20&t=Ss-WLpdR1rCNWhReCSiZZg
This incredible vaccine effect speaks volumes, and is the main reason why many are simply moving on from the pandemic...a smidge early, imv. Again, this graph plots IFR, which as I mentioned needs to be coupled with R0 and time to provide the true clinical impact. Prevalence is
what allows SARS2 to find the gaps in the vax armour, and new VoC's can be better at penetrating them, effectively increasing R0 (inherent, Rt when we factor in variable susceptible populations). Again, most vaccinees won't suffer severe disease, but not all, so the denominator,
small as it is, is now multiplied by a much larger numerator. By no means as large as before vax, but still enough to cause 100s of deaths every day, and to increase rarer events such as children being hospitalised (cf adults). That, and despite the boosters etc., we are still
in a position where millions remain unvaccinated. The main gap is children, and I won't repeat my views on the lackadaisical way in which juvenile vaccines are being portrayed to UK parents.
So, how to reduce prevalence? Well, I'm bracing myself for being branded a lockdown
So, how to reduce prevalence? Well, I'm bracing myself for being branded a lockdown
zealot or similar once more, but actually this is entirely the opposite. It won't mention zero COVID either, but it damned well will involve suppressing virus transmission...
However, this doesn't need to be viewed as a restriction, and my view is that I'd rather take a few MINOR
However, this doesn't need to be viewed as a restriction, and my view is that I'd rather take a few MINOR
inconveniences like wearing a mask on a bus, if it meant that I could make the most of new found freedoms in the knowledge that clinically vulnerable people weren't being deprived of it, or at least much less so.
I'm going to get long COVID out of my system now, just by saying
I'm going to get long COVID out of my system now, just by saying
that current policy ignores it completely, which is negligent and will end up costing the beancounters more in the long run. But, the human cost, especially for #LongCovidKids is wholly unacceptable. To raise awareness of such a condition isn't scaremongering either, it's reality
. Fact is, we've spent 2 yrs swinging like a pendulum between extreme lockdowns/restrictions and attempted openings on different scales...our response to SARS2 is more seasonal than the virus, it seems...!
However, behaviour is a huge factor in determining spread, as we saw last
However, behaviour is a huge factor in determining spread, as we saw last
July in reaction to "freedom" day, Xmas with Omicron, and throughout the pandemic with shielders conveniently exempting themselves from daily stats.
We can provide a framework to allow people's behaviour and altruism to really get this virus under control in partnership with vax,
We can provide a framework to allow people's behaviour and altruism to really get this virus under control in partnership with vax,
but it will require effort and investment from government. It will almost certainly have benefits in other aspects as well, such as limiting flu spread...😉. How? Well, it's really not that difficult - clean the air, mitigate when it can't be done easily (masks, filters), test if
necessary when prevalence or scenarios require it, and vaccinate the (world) population effectively.
If we reduce prevalence, it will matter less that our antibodies wane, it will mean less long COVID, fewer deaths/hospitalisations, and actual freedom for all. We aren't talking
If we reduce prevalence, it will matter less that our antibodies wane, it will mean less long COVID, fewer deaths/hospitalisations, and actual freedom for all. We aren't talking
elimination, but if the worshippers of endemicity finally realise their dream, if the level of infections are anything like at present then we will genuinely never get anywhere near to normal. Look at how other countries are investing in ventilation, free masks, testing and esp
genetic surveillance, whilst we're now switching the lights off and hoping too much stuff doesn't get broken in the ensuing darkness...a low endemic setpoint is going to be critical for this virus...as it really isn't the same as seasonal flu...
• • •
Missing some Tweet in this thread? You can try to
force a refresh