1/ STEP 4 Trial of Semaglutide for obesity treatment is a beautiful illustration of the physiology of body weight regulation. Let's explore it in this 🧵 

2/ First off, all study participants "received open-label once-weekly subcutaneous semaglutide, 0.25 mg, increased every 4 weeks to the maintenance dose of 2.4 mg once weekly by week 16, and continued to week 20."
3/ In addition, all participants received a lifestyle intervention from week 0 to week 68, which included:
👉counseling
👉Calorie-reduced diet
👉150 mins of PA / wk
👉tracking
In behavioral weight management, this is referred to as standard behavioral therapy (SBT).
👉counseling
👉Calorie-reduced diet
👉150 mins of PA / wk
👉tracking
In behavioral weight management, this is referred to as standard behavioral therapy (SBT).

4/ As expected, all participants lost wt, ~11% BWL at 20 weeks.

5/ After 20 wks, they were randomly assigned to placebo injections or continued semaglutide for the remainder of the 68-week trial. Since both groups were still engaging in behavioral intervention for weight loss...
What do you think happened?
What do you think happened?
6/ Expectedly or unexpectedly, the placebo group started regaining weight (on track for a nadir of 3-5% wt loss from baseline, which we typically see in long-term lifestyle interventions). However, the semaglutide group continued to lose weight.
How come?
How come?

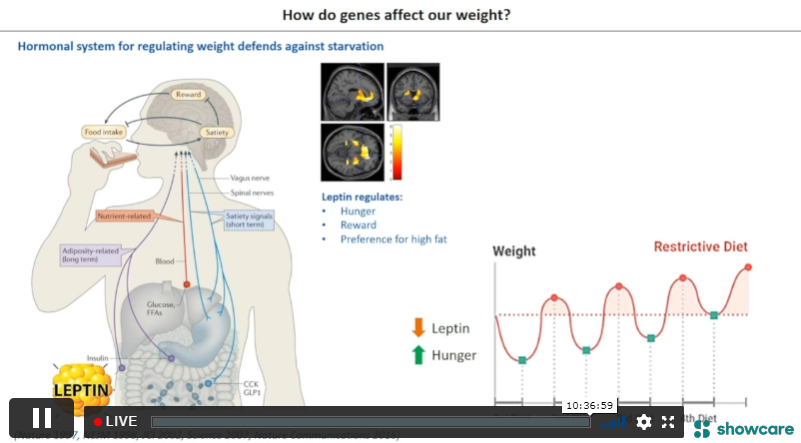
7/ Weight regain is primarily due to counter-physiological mechanisms owing to our evolutionary biology. I explain it in a previous thread here. ⬇️
https://twitter.com/MichaelAlbertMD/status/1503807886568341515?s=20&t=DqAKUZbC8VQoqsAxzNClWA
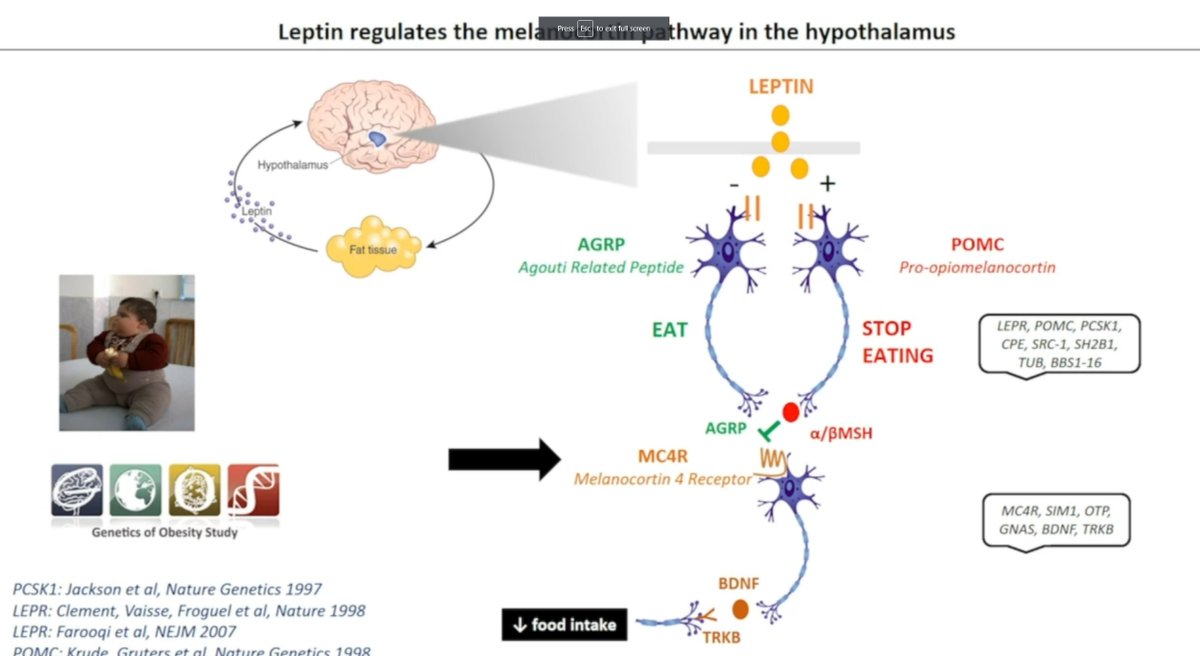
8/ Why does semaglutide work so well for obesity? Semaglutide has a number of proposed mechanisms, but most of its weight-related effects appear to be mediated through a single G protein-coupled receptor (GPCR) located in CNS.
sciencedirect.com/science/articl…
sciencedirect.com/science/articl…

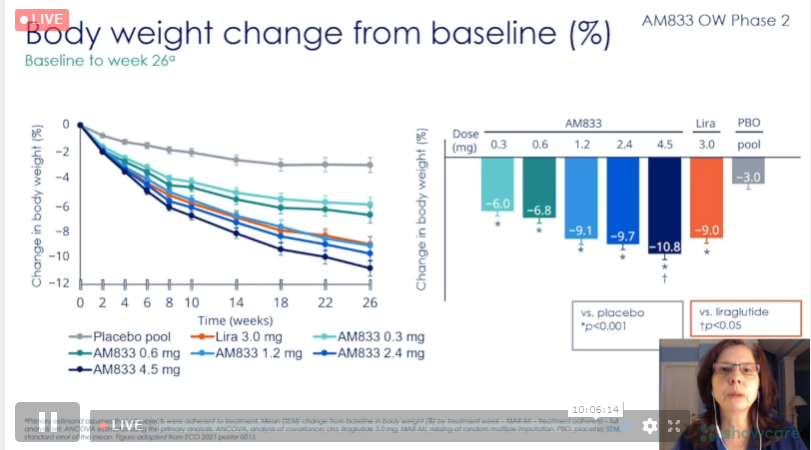
9/ As a result, there is a measurable decrease in ad-libitum eating likely related to better appetite control, ⬇️ cravings, better management of eating (overall), and less preference for energy-dense fatty foods.
ncbi.nlm.nih.gov/pmc/articles/P…
ncbi.nlm.nih.gov/pmc/articles/P…
10/ Semaglutide is helping to address many of the central neurohormonal systems that go awry as part of the pathophysiology of obesity.
nature.com/articles/s4157…
nature.com/articles/s4157…
11/ STEP 4, along with other research, demonstrates that the effective treatment of obesity is derived from biological therapies. Hoping to reinforce self-efficacy without addressing the abn physio is neglecting the central role of the 🧠 in maintaining excess adiposity. [end]
• • •
Missing some Tweet in this thread? You can try to
force a refresh