1/9 #TumorBoardTuesday Thursday Case Wrap Up🎀
⏰ for #TBT Case Wrap Up!
We looked at dx and tx of Carcinoma of Unknown Primary (#CUP), including how 🧬 can change tx.
There was a lot to learn–we captured what we could of the discussion here:
twitter.com/i/events/15089…
⏰ for #TBT Case Wrap Up!
We looked at dx and tx of Carcinoma of Unknown Primary (#CUP), including how 🧬 can change tx.
There was a lot to learn–we captured what we could of the discussion here:
twitter.com/i/events/15089…
2/9 #TumorBoardTuesday Thurs Case🎀
Take🏠:
#CUP is complicated!
✅Comprehensive approach needed, including:
H&P,🔬, 🩻, 🧬
✅Overall inc of CUP is ⬇️–many liver CUP being recognized as cholangio
✅NGS can help augment the w/u
✅STK11= frequently mut in lung; ⬇️response to IO
Take🏠:
#CUP is complicated!
✅Comprehensive approach needed, including:
H&P,🔬, 🩻, 🧬
✅Overall inc of CUP is ⬇️–many liver CUP being recognized as cholangio
✅NGS can help augment the w/u
✅STK11= frequently mut in lung; ⬇️response to IO

3/9 #TumorBoardTuesday Thursday Case🎀
@LaurenBzak’s case: Pt p/w solitary 🧠 lesion ➡️ poorly diff adenocarcinoma. But–not a primary CNS malignancy. NOTHING outside 🧠on CT or PET.
🧐What should we do next?
👍Detailed H&P (smoking hx)
👍PATH CONSULT!
@LaurenBzak’s case: Pt p/w solitary 🧠 lesion ➡️ poorly diff adenocarcinoma. But–not a primary CNS malignancy. NOTHING outside 🧠on CT or PET.
🧐What should we do next?
👍Detailed H&P (smoking hx)
👍PATH CONSULT!
4/9 #TumorBoardTuesday Thurs Case🎀
😱No clear answers from path:
🔸 CAM5.2 ➕
🔸 CK7 ➕
🔸 CK20 ➖
🔸 All other markers ➖
‼️Keep path team on board & provide lots of clin context‼️
IHC can narrow the list.
@OncoThor shared this excellent ref:
ncbi.nlm.nih.gov/pmc/articles/P…
😱No clear answers from path:
🔸 CAM5.2 ➕
🔸 CK7 ➕
🔸 CK20 ➖
🔸 All other markers ➖
‼️Keep path team on board & provide lots of clin context‼️
IHC can narrow the list.
@OncoThor shared this excellent ref:
ncbi.nlm.nih.gov/pmc/articles/P…

5/9 #TumorBoardTuesday Thursday Case🎀
➡️Now what❓
Well...it is @TumorBoardTues - so we think about NGS.
✍️Caveats: 🧬 & tumor origin (TOO) tests do NOT always provide the answer - they provide data points which contribute to the overall clinical picture🖼 & need context
➡️Now what❓
Well...it is @TumorBoardTues - so we think about NGS.
✍️Caveats: 🧬 & tumor origin (TOO) tests do NOT always provide the answer - they provide data points which contribute to the overall clinical picture🖼 & need context
5.5/9 #TumorBoardTuesday Thurs Case🎀
Our pt:
✳️ MSI stable
✳️ TMB 20 m/mB
✳️ PDGFRA amplification
✳️ TP53 c.388C>T (53%)
✳️ STK11 c.468C>A (59%)
✳️ SMARCA4 c.3554_3556delinsCAT (38%)
🔬 PD-L1 20%
Our pt:
✳️ MSI stable
✳️ TMB 20 m/mB
✳️ PDGFRA amplification
✳️ TP53 c.388C>T (53%)
✳️ STK11 c.468C>A (59%)
✳️ SMARCA4 c.3554_3556delinsCAT (38%)
🔬 PD-L1 20%
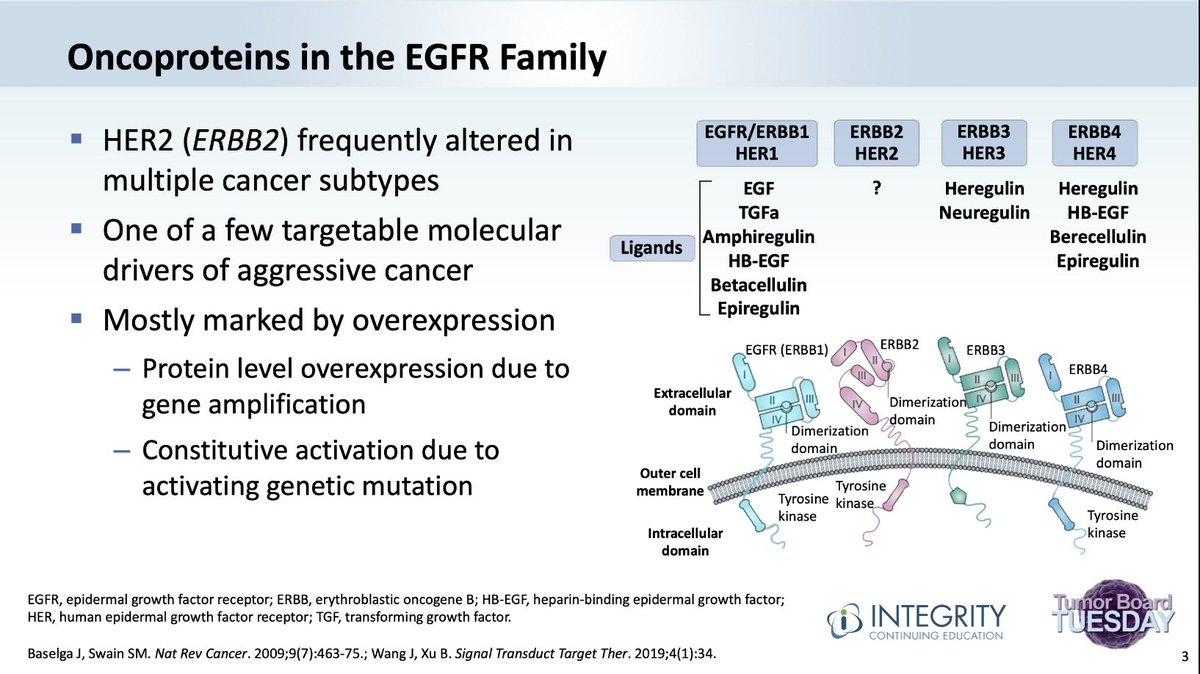
6/9 #TumorBoardTuesday Thurs Case🎀
Which led to discussion about STK11 & SMARCA4 mut. STK11 is assoc w ⬇️response to IO, SMARCA4 is assoc w ⬆️TMB and is common in lung ca w 🚬risk factor. Could this be 🫁 cancer oligomet to 🧠?
pubmed.ncbi.nlm.nih.gov/28555282/
pubmed.ncbi.nlm.nih.gov/31751681/
Which led to discussion about STK11 & SMARCA4 mut. STK11 is assoc w ⬇️response to IO, SMARCA4 is assoc w ⬆️TMB and is common in lung ca w 🚬risk factor. Could this be 🫁 cancer oligomet to 🧠?
pubmed.ncbi.nlm.nih.gov/28555282/
pubmed.ncbi.nlm.nih.gov/31751681/

7/9 #TumorBoardTuesday Thurs Case🎀
The best part about NGS: when alteration is found, may help inform tx.
@targetcancer pointed out an ongoing clin trial to move #CUP care forward
The best part about NGS: when alteration is found, may help inform tx.
@targetcancer pointed out an ongoing clin trial to move #CUP care forward
https://twitter.com/targetcancer/status/1509249255537614856
8/9 #TumorBoardTuesday Thurs Case🎀
Now that you’ve made it this far–you’re well equipped to get some free CME!
Answer 2 questions re: CUP evaluation and treatment here: bit.ly/3NlA3b7
Now that you’ve made it this far–you’re well equipped to get some free CME!
Answer 2 questions re: CUP evaluation and treatment here: bit.ly/3NlA3b7

9/9 #TumorBoardTuesday Thurs Case🎀
🙏 #CUP req being 🕵️♀️. Based on 🧬& TMB, going to trial IO for our pt.
🤔 TOO testing limited now, next gen informed by machine learning coming
📅 Join us for #TBT on 04/12 at 8pm EST @W_Park_MD discusses #PancreaticCancer! #PrecisionMedicine
🙏 #CUP req being 🕵️♀️. Based on 🧬& TMB, going to trial IO for our pt.
🤔 TOO testing limited now, next gen informed by machine learning coming
📅 Join us for #TBT on 04/12 at 8pm EST @W_Park_MD discusses #PancreaticCancer! #PrecisionMedicine
@BHuffmanMD @manjuggm @leslye23420629 @mtmdphd @KReissMD @graokane @rmistry91 @DocOnco @NDeVitoMD @drymtn @jhatjhmi1 @AdhamJurdia @hfuentesbayne @doctorC369 @oncospot @HemOncFellows
@kis_lorand @IHC_guy @sara_m88 @TimRowesays @DrBonillaOnc
@kis_lorand @IHC_guy @sara_m88 @TimRowesays @DrBonillaOnc
👨🏽⚕️ We enjoy all leaders and their fascinating case presentations and ❤️ new perspectives!
👩🏻⚕️If you'd like to lead a #TumorBoardTuesday case discussion, please message @MPishvaian, @TumorBoardTues, or @Empoweringpts9!! #GITwitter #OncTwitter #Oncology
👩🏻⚕️If you'd like to lead a #TumorBoardTuesday case discussion, please message @MPishvaian, @TumorBoardTues, or @Empoweringpts9!! #GITwitter #OncTwitter #Oncology
• • •
Missing some Tweet in this thread? You can try to
force a refresh