
1/
A #dermtwitter and #MedEd #tweetorial on...
LINEAR IGA!
This is an autoimmune blistering disorder that can be triggered by drugs!
Hey #medtwitter, what do you think is one of common culprits for causing this eruption?
A #dermtwitter and #MedEd #tweetorial on...
LINEAR IGA!
This is an autoimmune blistering disorder that can be triggered by drugs!
Hey #medtwitter, what do you think is one of common culprits for causing this eruption?
2/
You'd be correct if you said vancomycin!
Vanco triggers IgA to attack proteins in the hemidesmosome that holds epidermis to the basement membrane. That means this is a part of the PEMPHIGOID group.
So you get TENSE blisters with a NEGATIVE NIKOLSKY.
You'd be correct if you said vancomycin!
Vanco triggers IgA to attack proteins in the hemidesmosome that holds epidermis to the basement membrane. That means this is a part of the PEMPHIGOID group.
So you get TENSE blisters with a NEGATIVE NIKOLSKY.

3/
For the #dermatology residents who need to memorize this, remember that the antigen that is targeted is the 97 kDa portion of the extracellular domain found in BPAg2.
For everyone, remember this is part of the pemphigoiD (D for deep) group, hence the exam findings.
For the #dermatology residents who need to memorize this, remember that the antigen that is targeted is the 97 kDa portion of the extracellular domain found in BPAg2.
For everyone, remember this is part of the pemphigoiD (D for deep) group, hence the exam findings.
4/
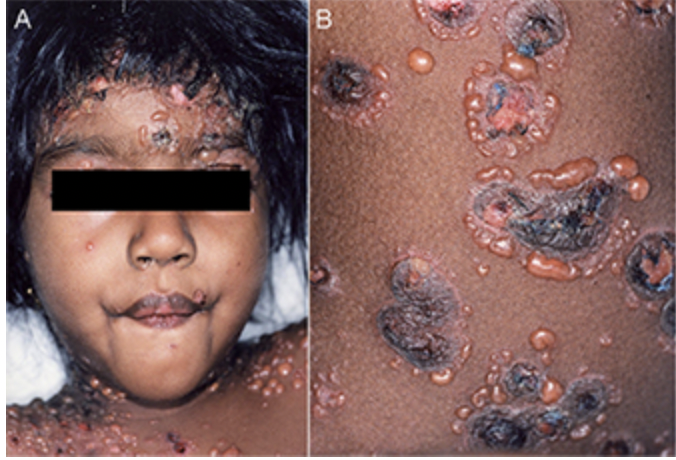
On clinical exam, the unusual thing about this blistering eruption is the configuration of the bullae. They are usually in an ANNULAR pattern!
So you might ask, wait - why is it called LINEAR IgA and not Annular IgA?!
On clinical exam, the unusual thing about this blistering eruption is the configuration of the bullae. They are usually in an ANNULAR pattern!
So you might ask, wait - why is it called LINEAR IgA and not Annular IgA?!
5/
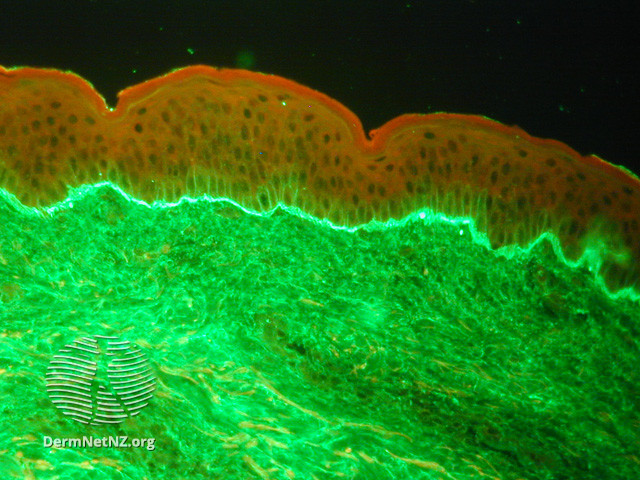
It's got to do with the direct immunofluorescence pattern. On the DIF, you see a linear deposition of IgA at the Basement Membrane Zone, leading to the name (as opposed to IgG in bullous pemphigoid).
But clinically, again, you see annular tense bullae with negative Nikolsky.
It's got to do with the direct immunofluorescence pattern. On the DIF, you see a linear deposition of IgA at the Basement Membrane Zone, leading to the name (as opposed to IgG in bullous pemphigoid).
But clinically, again, you see annular tense bullae with negative Nikolsky.
6/
While Vancomycin is the most common trigger, it's important to know other drugs can do it too (NSAIDs, ACEi, Diuretics, Abx, etc).
Additionally, kids can get an idiopathic version! Same clinical and pathologic findings, but we call it Chronic Bullous Disease of Childhood.
While Vancomycin is the most common trigger, it's important to know other drugs can do it too (NSAIDs, ACEi, Diuretics, Abx, etc).
Additionally, kids can get an idiopathic version! Same clinical and pathologic findings, but we call it Chronic Bullous Disease of Childhood.
7/
This tweet goes out to the derm residents out there. Remember that when you see IgA in the pathophysiologic process, you should think of neutrophils. That's the case here too!
So treatment is d/c of offending trigger, and starting an anti-PMN drug like dapsone or colchicine.
This tweet goes out to the derm residents out there. Remember that when you see IgA in the pathophysiologic process, you should think of neutrophils. That's the case here too!
So treatment is d/c of offending trigger, and starting an anti-PMN drug like dapsone or colchicine.
8/
If a recent drug doesn't seem to be at fault, there are other associated conditions (eg: IBD, cancer). I've seen IBD drive Linear IgA, in which case co managing with GI is super important. That's where choosing something that works on both gut and skin is critical!
If a recent drug doesn't seem to be at fault, there are other associated conditions (eg: IBD, cancer). I've seen IBD drive Linear IgA, in which case co managing with GI is super important. That's where choosing something that works on both gut and skin is critical!
9/
Let's summarize!
✅Linear IgA is a blistering disease where IgA targets the BMZ, causing annular tense bullae.
✅Vancomycin (and other drugs can trigger this) - as can IBD and cancer. Also can see in kids!
✅Treatment is addressing the underlying trigger, and anti-PMN drugs.
Let's summarize!
✅Linear IgA is a blistering disease where IgA targets the BMZ, causing annular tense bullae.
✅Vancomycin (and other drugs can trigger this) - as can IBD and cancer. Also can see in kids!
✅Treatment is addressing the underlying trigger, and anti-PMN drugs.
10/10
Thanks for joining for this short #thread/#tweetorial on Linear IgA! It's relatively rare, but a good one to know, especially if you ever reach for vancomycin in your patients!
Leave a suggestion for another topic if you'd like. Thanks everyone!
Thanks for joining for this short #thread/#tweetorial on Linear IgA! It's relatively rare, but a good one to know, especially if you ever reach for vancomycin in your patients!
Leave a suggestion for another topic if you'd like. Thanks everyone!
• • •
Missing some Tweet in this thread? You can try to
force a refresh














