🔥 Finally we have evidence, how Pfizer came to calculate a 95% vaccine efficacy!
Real efficacy is likely only 19%, with a very bad side effect profile of up to 0.8% severe side effects, as reported by German Hospital Study Charité!
🧵 1/n #Covid #Covid19 #Corona #Coronavirus
Real efficacy is likely only 19%, with a very bad side effect profile of up to 0.8% severe side effects, as reported by German Hospital Study Charité!
🧵 1/n #Covid #Covid19 #Corona #Coronavirus
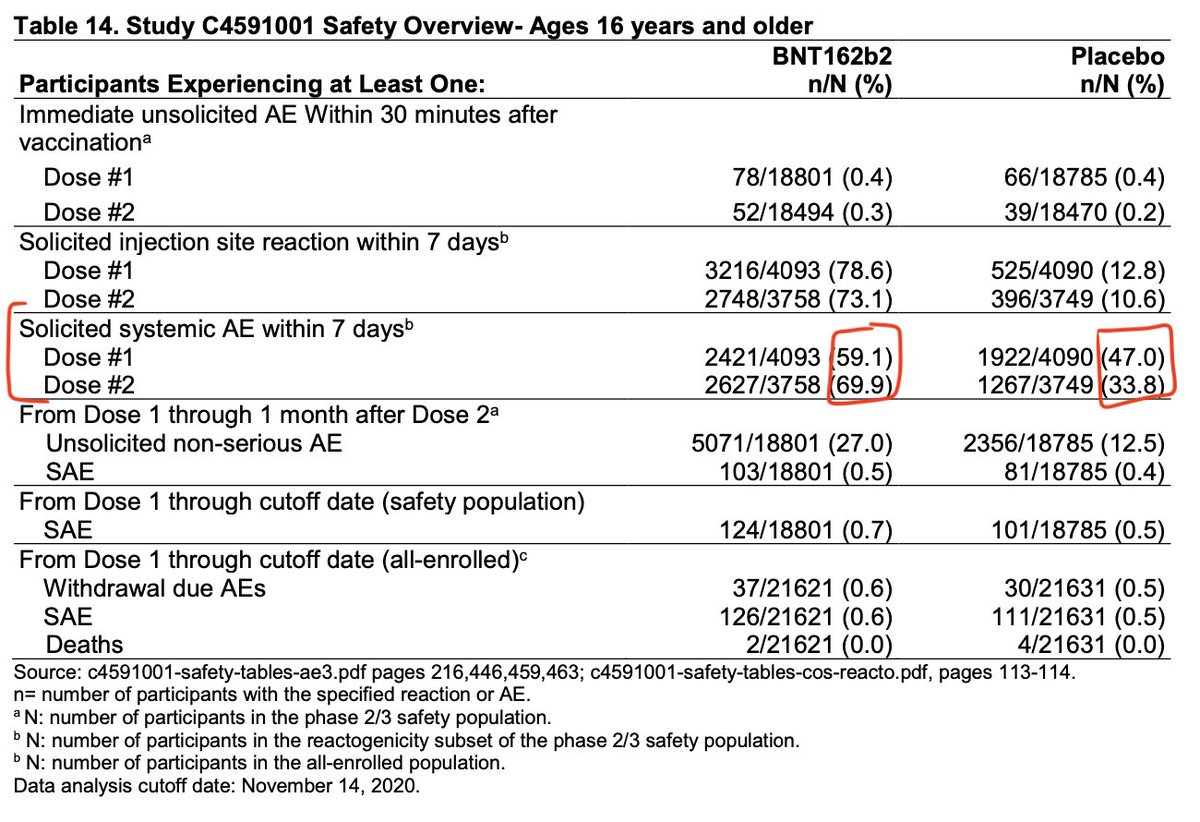
As we know from the published study, the vaccine arm suffered from +12.1% and +36.1% more systemic Adverse Events (side-effects) than the placebo group.
These side effects, are indistinguishable from COVID19 in most cases!
These side effects, are indistinguishable from COVID19 in most cases!
The following document, just released in the latest Pfizer batch shows, that Pfizer did NOT test patients for COVID-19, unless the investigator suspected COVID-19, and not vaccine side effects. So it is likely that they would almost never test, but classify them as vax reactions.

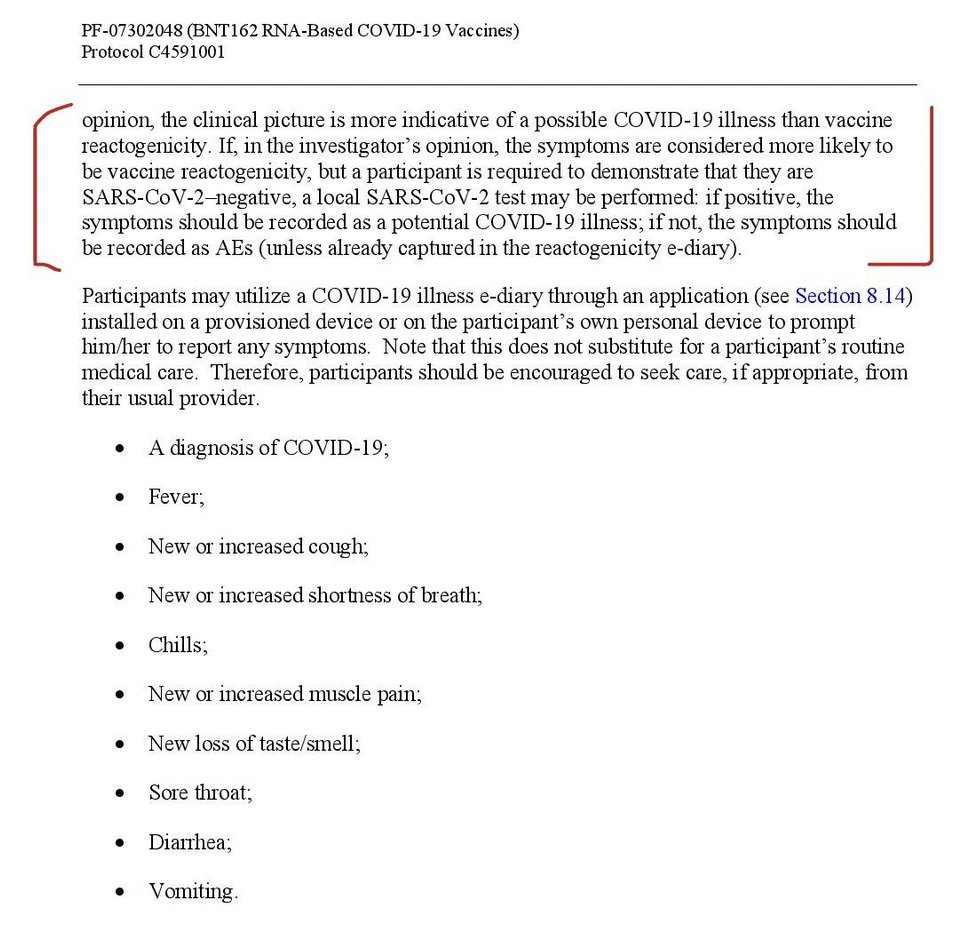
Pfizer reported these side effect as "unconfirmed COVID-19" in the just released documents.
Here we can see, that suspected COVID-19 was reported in 1595 vax recipients, and 1816 placebo recipients.
Based on these numbers VE is about 12%, but ...
Here we can see, that suspected COVID-19 was reported in 1595 vax recipients, and 1816 placebo recipients.
Based on these numbers VE is about 12%, but ...
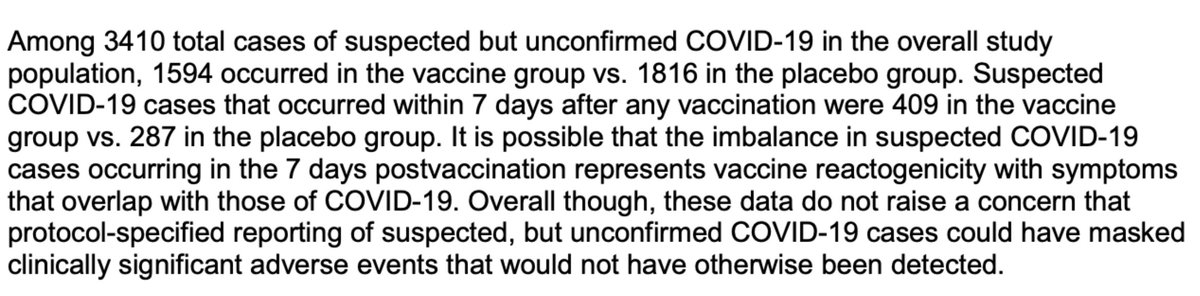
Of course, in reality one must include the confirmed COVID-19 cases as well, which would yield:
VE = ((1816+162)-(1594+8))/(1816+162) = 19.0%
So overall, we have strong reasons to believe that the vaccine might be just 19% effective in preventing COVID-19, but...
VE = ((1816+162)-(1594+8))/(1816+162) = 19.0%
So overall, we have strong reasons to believe that the vaccine might be just 19% effective in preventing COVID-19, but...
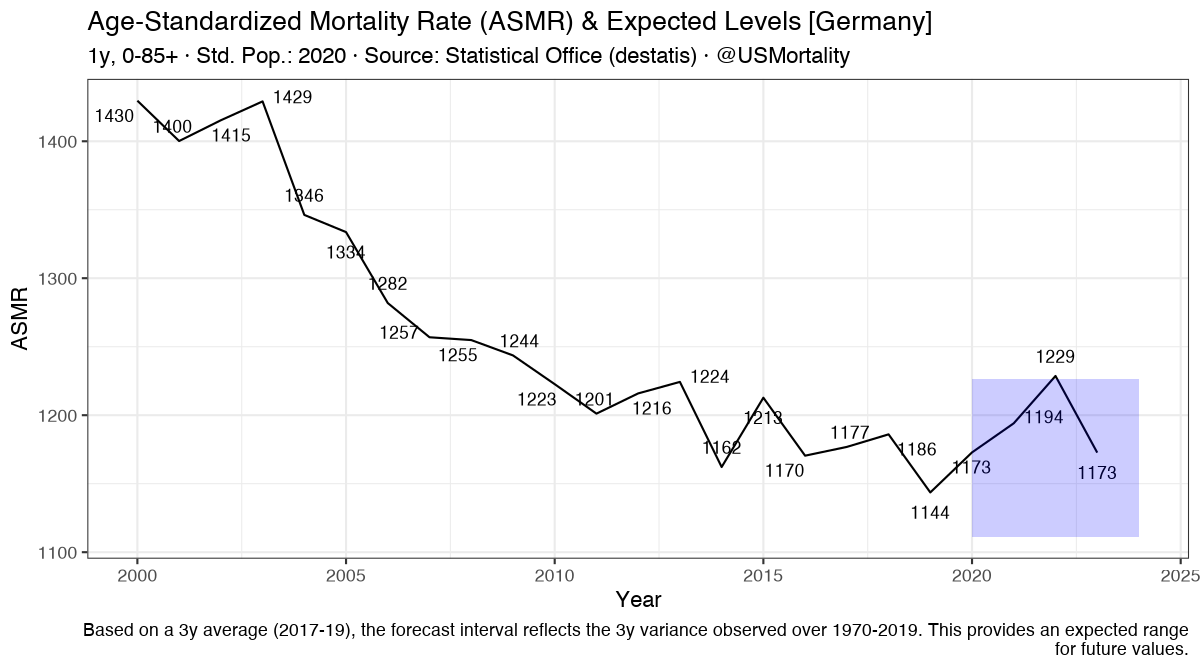
A recent study from Germany's top hospital Charité Berlin, revealed that about 0.8% of vaccinated suffer "severe long-term side effects".
https://twitter.com/USMortality/status/1521656145257156614?s=20&t=QrneNuoDw6nQkPTMuQdgnQ
So it becomes quite clear that the cost/benefit overall is very likely there, given the fairly large chance of severe side effects, compared to other vaccines!
Sources:
phmpt.org/pfizers-docume…
cdn.pfizer.com/pfizercom/2020…
blogs.bmj.com/bmj/2021/01/04…
Sources:
phmpt.org/pfizers-docume…
cdn.pfizer.com/pfizercom/2020…
blogs.bmj.com/bmj/2021/01/04…
H/t to @justin_hart for providing some of the links and screenshots!
Small addendum & correction, since Twitter still doesn't have an edit button:
3. post: "Pfizer did NOT test patients for COVID-19 *up to 7 days after vaccination*, unless the investigator suspected COVID-19, and not vaccine side effects."
3. post: "Pfizer did NOT test patients for COVID-19 *up to 7 days after vaccination*, unless the investigator suspected COVID-19, and not vaccine side effects."
7. post: "So it becomes quite clear that the cost/benefit overall is very likely *NOT* there,"
Summarized:
Pfizer encouraged to generally not test for COVID-19 up to 7 days after each vaccination.
It would have just taken 154 patients to bring VE to 0%.
That represents just 3.1% ( `(162-8)/(2421+2627)` ) of vaccinated patients that experienced any vaccine side effect!
Pfizer encouraged to generally not test for COVID-19 up to 7 days after each vaccination.
It would have just taken 154 patients to bring VE to 0%.
That represents just 3.1% ( `(162-8)/(2421+2627)` ) of vaccinated patients that experienced any vaccine side effect!
And here's part 2:
In this thread Jikky explains another vector of evidence that proofs that the vaccinated arm also got infected (but since not tested, undetected):
In this thread Jikky explains another vector of evidence that proofs that the vaccinated arm also got infected (but since not tested, undetected):
https://twitter.com/Jikkyleaks/status/1529076970486923264
• • •
Missing some Tweet in this thread? You can try to
force a refresh