Pterygopalatine fossa🧵- inspired by ?s from med students in neuroanatomy lab & a resident w/ case of perineural tumor spread on same day! #meded #FOAMrad #medtwitter #medstudents #radiology #neurorad #HNrad #radres #neurology #ENT #temporalbone #neurosurgery #neuroanatomy
1/22
1/22
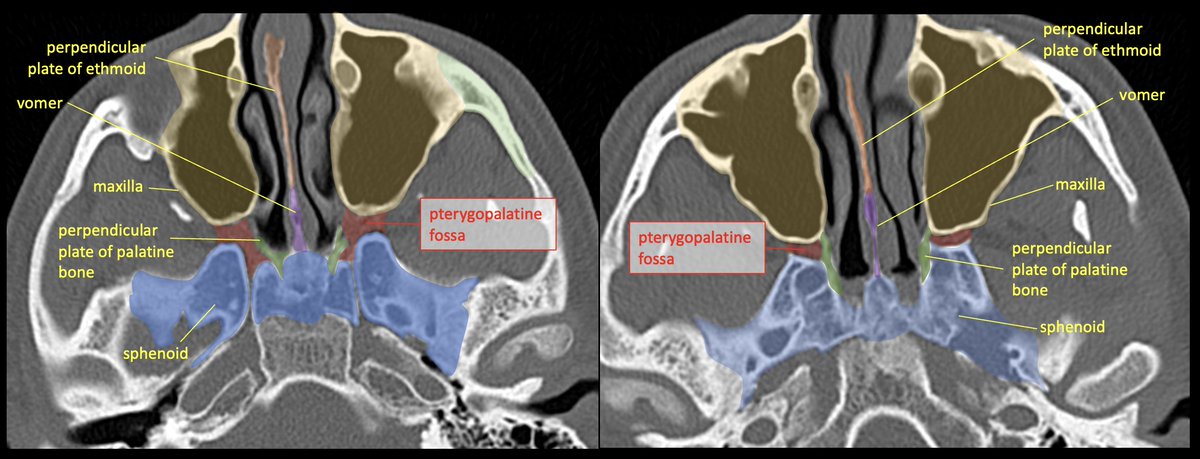
The PTERYGOPALATINE FOSSA (PPF) is a space deep in the face/skull base, bordered anteriorly by the maxilla (max sinus), posteriorly by the pterygoid base of the sphenoid, and medially by the perpendicular plate of the palatine bone. 2/22
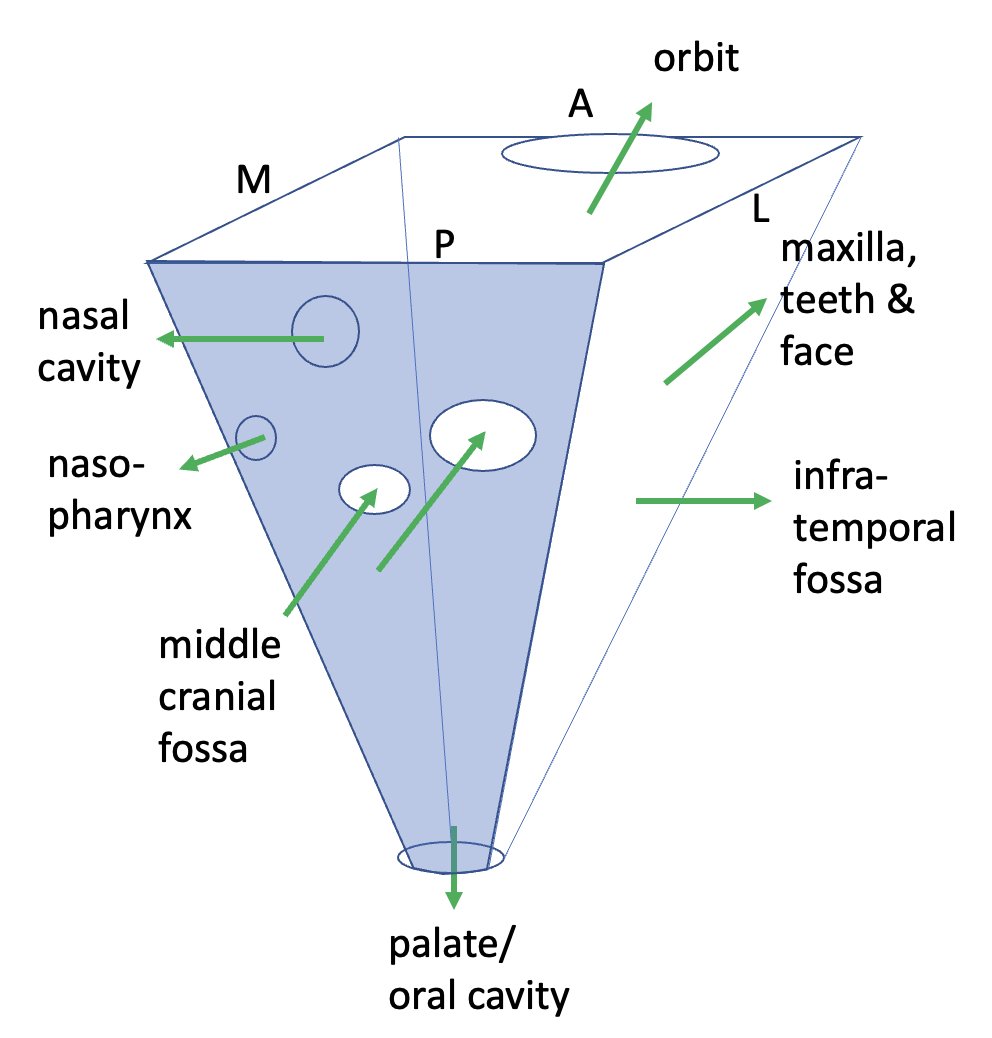
It’s best to think of the PPF as a crossroads/intersection. Think about the roads that lead to and from it, and the cast of characters that pass through.
Some like to simplify/visualize the PPF as a cube or inverted pyramid.
3/22
Some like to simplify/visualize the PPF as a cube or inverted pyramid.
3/22
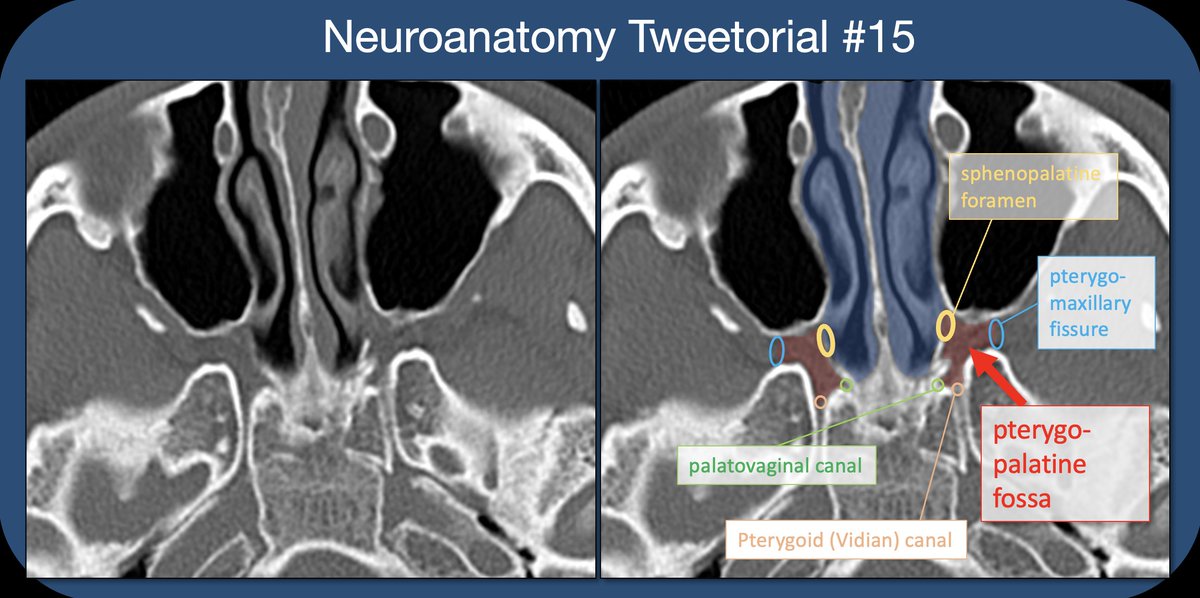
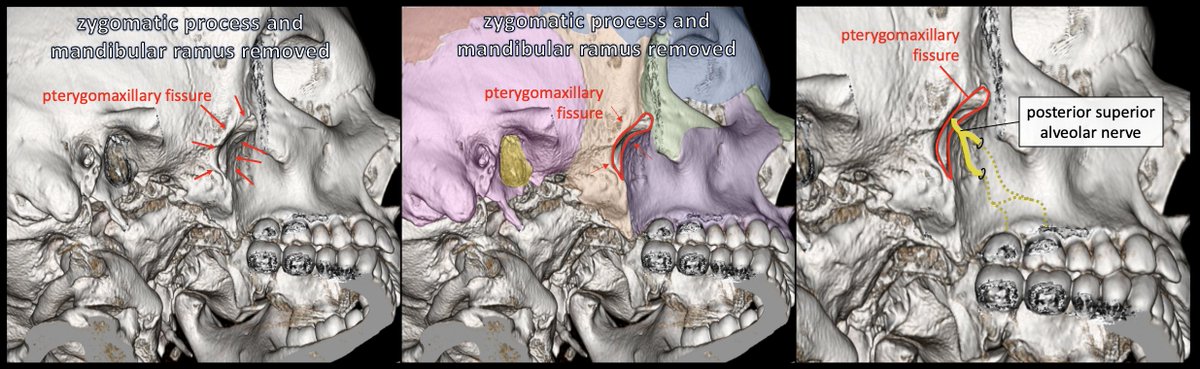
The PPF is accessed from laterally via the PTERYGOMAXILLARY FISSURE (PMF), an open crevasse between the pterygoid base of the sphenoid and the post maxilla. On 3D images, It can be seen deep to the zygomatic process.
4/22
4/22



The PMF is the lateral exit route from PPF; the POST-SUP ALVEOLAR NERVE branches from the INFRAORBITAL nerve & travels along the lateral margin of maxilla before diving into the wall to innervate the maxillary molars (also innervates max sinus and post oral mucosa).
5/22
5/22
Within the PPF lives the PTERYGOPALATINE GANGLION (PPG) which contains post-synaptic parasympathetic cell bodies-->lacrimal gland and sinus/nasal/oral mucosa. Many other sympathetic and somatic nerves travel through the ganglion without synapsing.
6/22
6/22

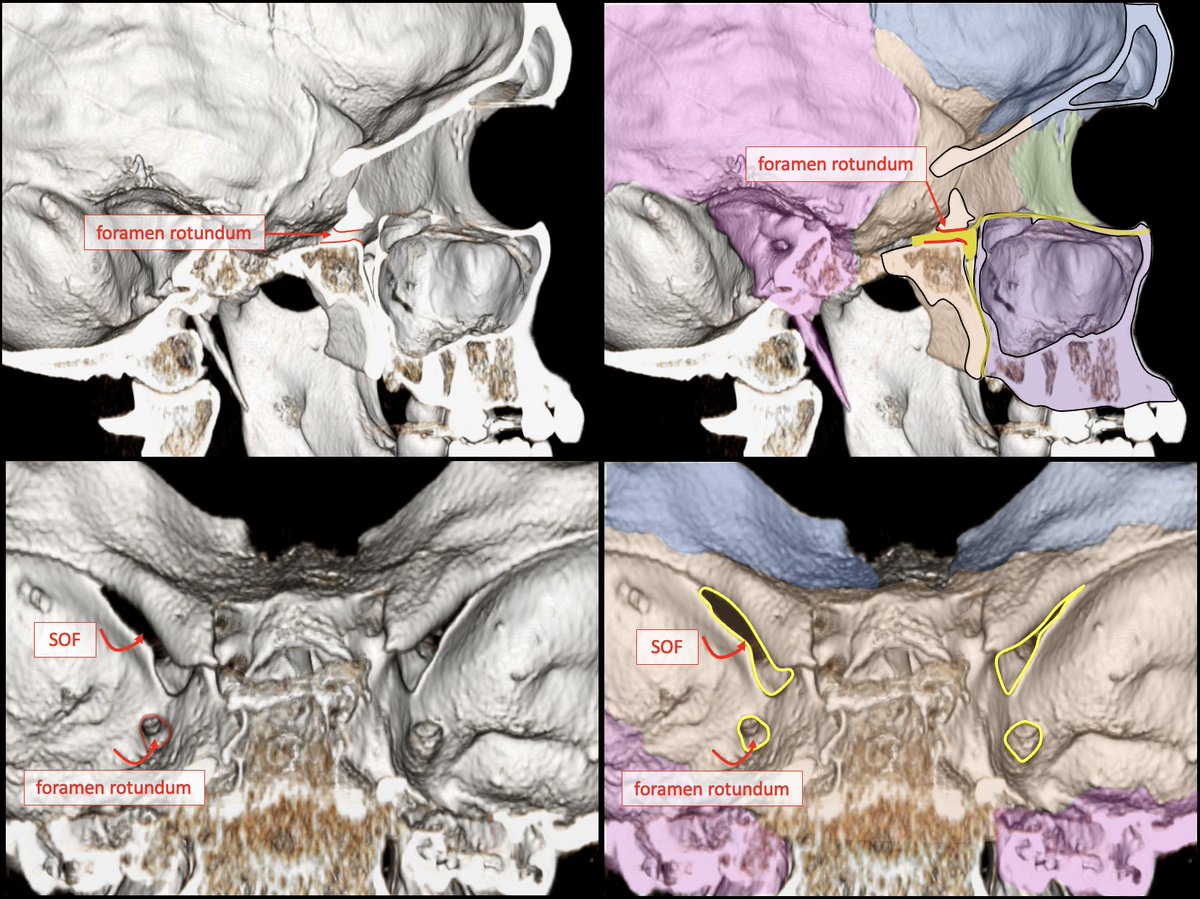
There are two canals which travel in the AP plane through the sphenoid bone, and transmit nerves/vessels from the middle cranial fossa to the PPF: FORAMEN ROTUNDUM and the PTERYGOID (VIDIAN) CANAL. The pterygoid canal is more inf and medial.
7/22
7/22

The FORAMEN ROTUNDUM transmits V2, the MAXILLARY NERVE, from the middle cranial fossa to the PPF in the AP direction. The Maxillary nerve (V2) contains mainly sensory information from the mid-face.
8/22
8/22
The PTERYGOID CANAL transmits the NERVE OF THE PTERYGOID CANAL through the sphenoid from mid cranial fossa (ant to foramen lacerum) to the PPF. Contains preganglionic parasympathetic (from gr sup petrosal n) and post-ganglionic sympathetic (deep petrosal n) from ICA plexus.
9/22
9/22

Anterior/superior exit route from the PPF is the INFERIOR ORBITAL FISSURE (IOF). The IOF is formed by the sphenoid and maxilla, connecting the PPF to the floor of the orbital apex.
10/22
10/22



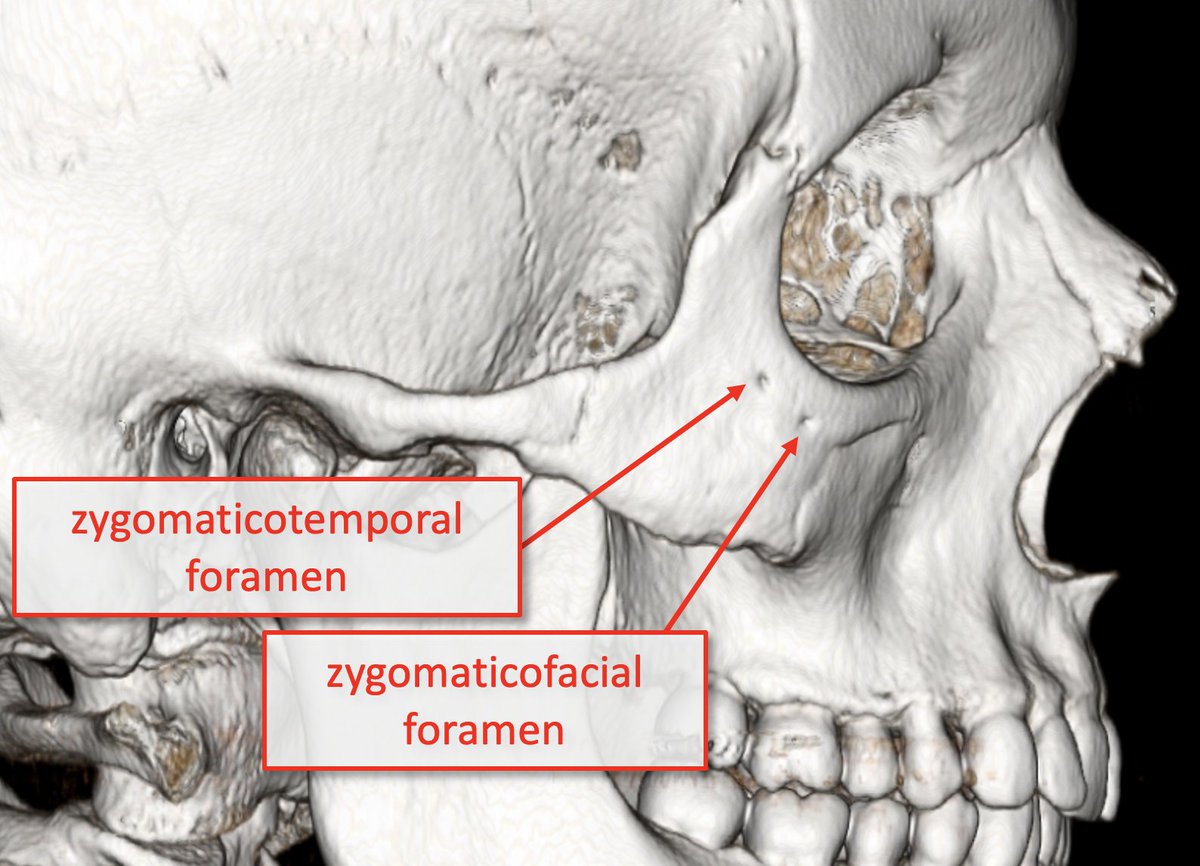
The IOF transmits the ZYGOMATIC and INFRAORBITAL NERVES (V2 branches); ZYGOMATIC n. supplies sensory info from skin over zygomatic/temporal bones (zygomaticotemporal and zygomaticofacial branches) & transmits postganglionic parasympathetic fibers to lacrimal nerve/gland.
11/22
11/22
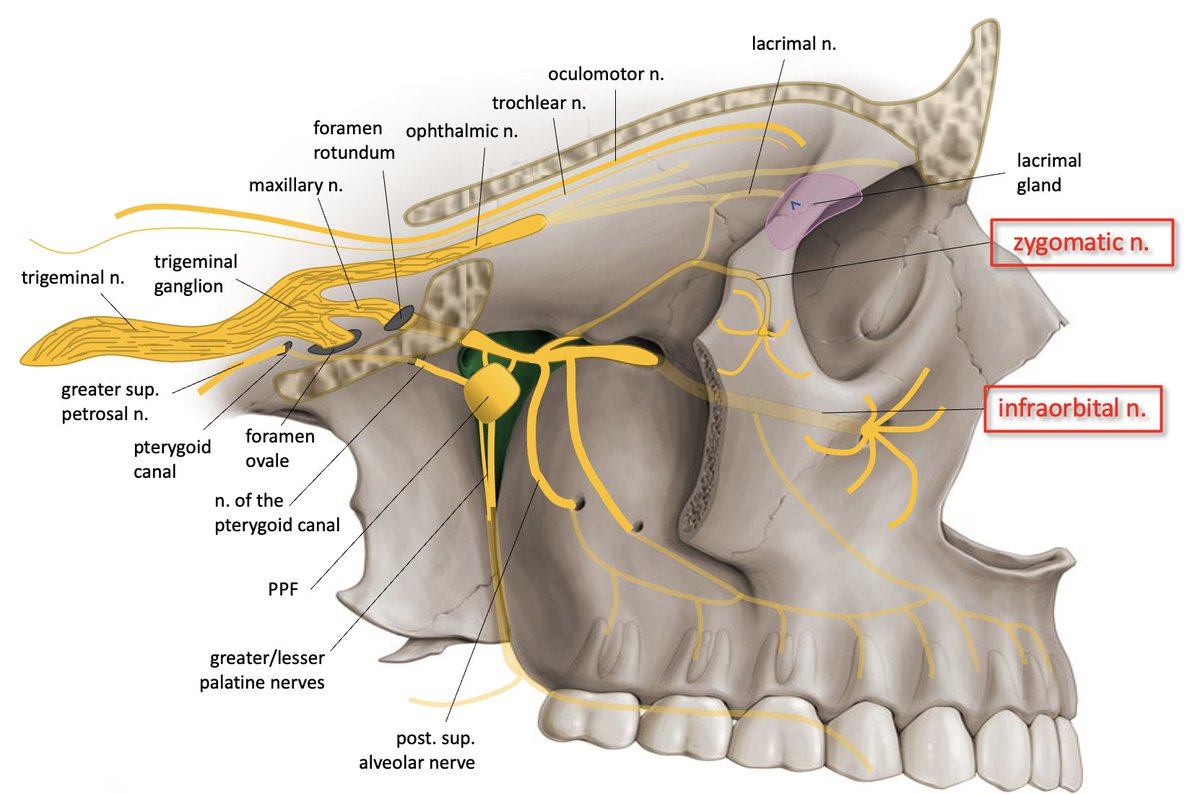
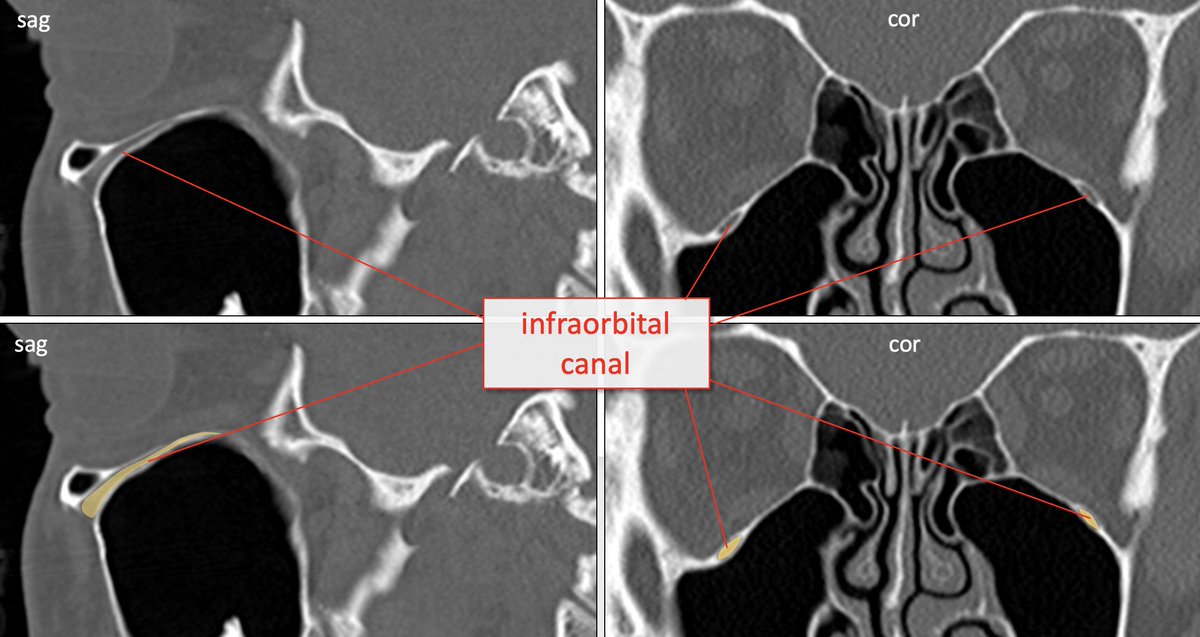
The INFRAORBITAL NERVE branches from V2 in the PPF➡️goes through IOF➡️extends anteriorly➡️ infraorbital groove/canal at orbital floor➡️exits INFRAORBITAL FORAMEN of the maxilla; supplies sensory to skin of cheek/lower eyelid.
12/22
12/22
The middle and ant sup alveolar nerves variably branch from the infraorbital nerve to supply sensory information from the maxillary teeth.
13/22
13/22
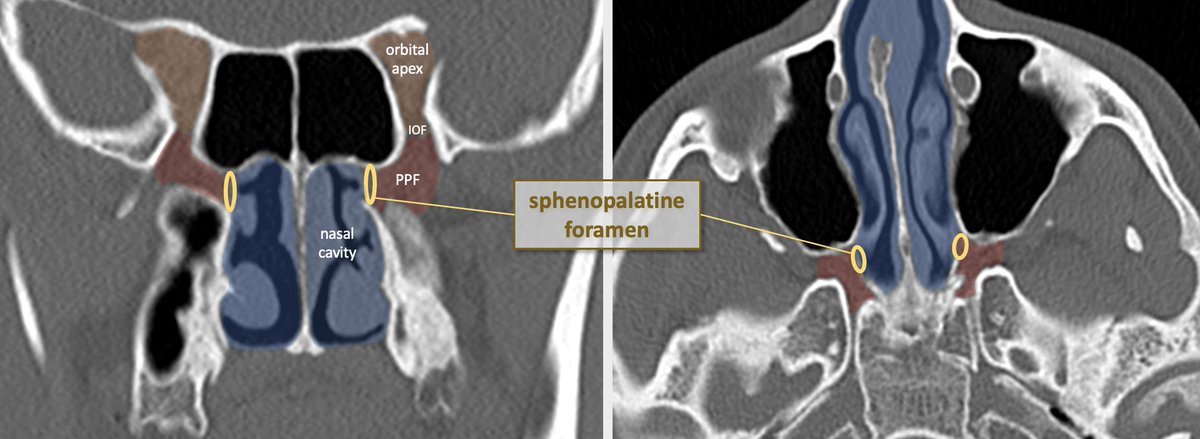
The medial exit route of the PPF leads to the nasal cavity via the SPHENOPALATINE FORAMEN which is formed by the palatine and sphenoid bones. It transmits the NASOPALATINE NERVE, posterior superior nasal nerves, and sphenopalatine artery/vein.
14/22
14/22

The NASOPALTINE NERVE branches from V2 in PPF (just after from f. rotundum)➡️traverses sphenopalatine foramen➡️courses within nasal septum anteroinferiorly➡️goes through INCISIVE FORAMEN of the maxillary palate (somatic sensory & autonomic supply to nasal mucosa).
15/22
15/22

The POST SUP NASAL NERVES also branch from V2 in PPF, traverse sphenopalatine foramen, and supply posterior nasal septum and lateral nasal wall.
16/22
16/22
Posteriorly and medially, the PHARYNGEAL NERVE (branch of V2) exits the PPF to the nasopharynx via the PALATOVAGINAL CANAL. It contains somatic sensory info and autonomic motor supplying the sup nasopharyngeal mucosa.
17/22
17/22

Inferiorly, the GREATER and LESSER PALATINE NERVES exit the PPF via the GREATER and LESSER PALATINE FORAMINA to the greater/lesser palatine canals:
18/22
18/22

The greater palatine foramen is located at the lateral suture between the maxillary palate and palatine bone; lesser canals are within the horizontal plate of the palatine bone. Nerves contain somatic sensory and autonomic innervation to the palate and oral cavity.
19/22
19/22


Thats the PPF! Important because so many functions, (including including midface sensation, sinonasal and pharyngeal sensation, pharyngeal/sinonasal mucus and saliva production, and lacrimation) all pass through this small anatomic space.
20/22
20/22
Importantly, mucosal tumors such as squamous cell CA and adenoid cystic CA love to spread along the nerves (perineural spread). Staging of pharynx, palate, sinus, salivary gland tumors requires knowledge of nerve pathways; knowing the PPF is imperative!
21/22
21/22
Clinical Case: adenoid cystic CA of the left palate, with associated perineural spread involving the palatine nerves, PPF, post/sup alveolar n, infraorbital n, maxillary n, mandibular n, and Meckel's cave.
22/22
22/22

• • •
Missing some Tweet in this thread? You can try to
force a refresh