1/Controversy in radiology gets tense! The Mt Fuji sign for tension pneumocephalus is under scrutiny.When should you call it?
A #tweetorial about #imaging this important #neurosurgery complication
#medtwitter #FOAMed #FOAMrad #medstudent #neurorad #radres #meded #neurotwitter
A #tweetorial about #imaging this important #neurosurgery complication
#medtwitter #FOAMed #FOAMrad #medstudent #neurorad #radres #meded #neurotwitter

2/Some believe that the peaked, mountain like appearance of the frontal lobes is a critical sign of a life-threatening complication & should be called & reported. Others believe it is too non-specific, is commonly seen when there isn’t tension & should be retired. Who’s right?

3/First, let’s clarify about what the Mt Fuji sign actually is. Most are familiar with the fact that large collections of pneumocephalus can compress the frontal lobes—making them look like the slopes of a mountain. But this isn’t actually enough to call Mt Fuji.

4/You also need to see frontal lobe separation. This means the subdural air tension is greater than CSF surface tension between the frontal lobes--one of the highest liquid surface tensions—so you know pressure is high. This little V is why it looks like Mt Fuji, not any mountain

5/Why do we get tension pneumocephalus? 3 main ways. (1) Upside down coke bottle effect w/a CSF leak. As liquid drips out w/a CSF leak, nature abhors a vacuum, so air rushes in to replace it. If outside pressure is higher than CSF pressure, more air will come in & create tension

6/Here’s a skullbase CSF leak creating pneumocephalus. As CSF leaks out, air replaces it. If air pressure is higher than intracranial pressure, more air will come in. The worst tension pneumocephalus I ever saw was a pt w/an unknown sphenoid sinus skullbase leak they put on CPAP!

7/Next mechanism is the ball valve mechanism. Air gets in through a defect (from trauma, surgery, etc). Increased pressure eventually pushes down on the brain, causing the brain to close the defect so the air can’t escape. This is the same mechanism seen w/tension pneumothorax.

8/Final mechanism is use of nitrous oxide in neuroanesthesia. If the pt has a subdural collection (usually w/air in the operative setting), nitrous oxide enters the subdural 34 times faster than it diffuses out as nitrogen into the blood stream—creating increased pressure/tension

9/This is why nitrous oxide is no longer commonly used in neuroanesthesia. Decreased use of nitrous oxide is also why tension pneumocephalus is less common in the post-operative setting now than it was in the past.

10/So how helpful is the Mt Fuji sign for determining tension pneumocephalus post-operatively (a time when pneumocephalus is common)? Well it turns out, the sign can be seen in 1/3 pts without a neurosurgical emergency. So it is not very specific and can cause overcalling

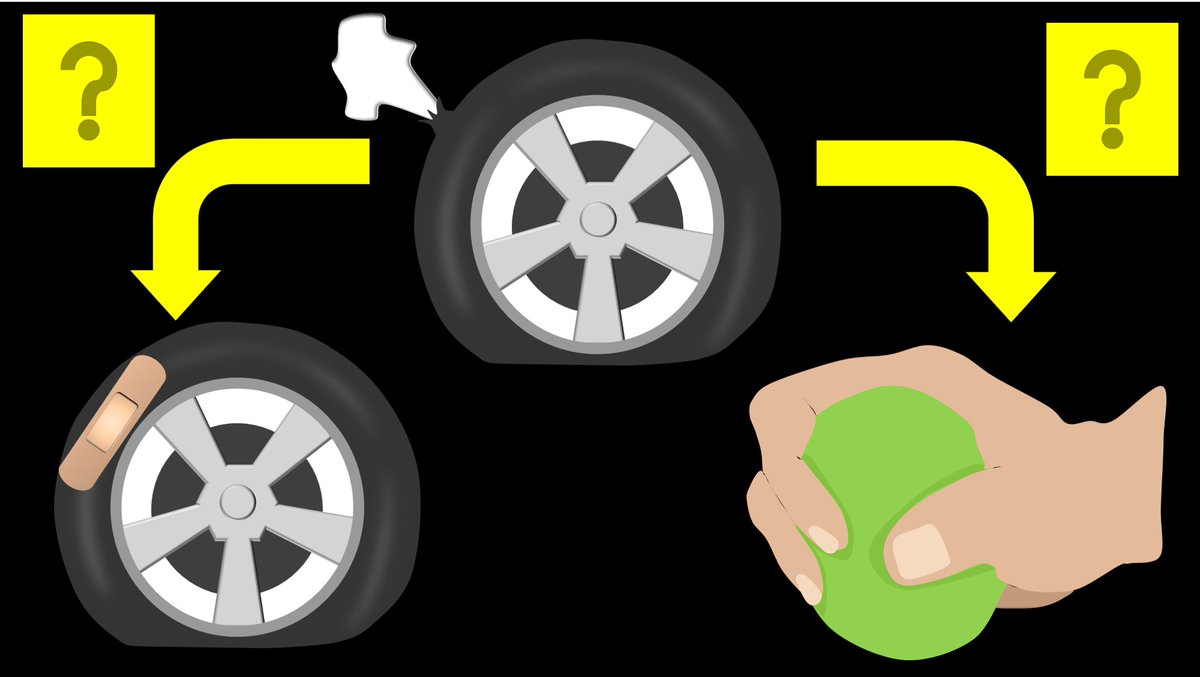
11/More importantly is how the pt is doing clinically. Significant pneumocephalus can be seen post op—but if the pt is not declining, even large amounts of pneumocephalus can be managed by putting the pt on 100% O2--just like w/a pneumothorax--w/good results.

12/So remember it isn’t just one sign—it is the whole picture of how the pt is doing clinically. Don’t lose sight of the forest for the mountain!
• • •
Missing some Tweet in this thread? You can try to
force a refresh