
1/Raise your hand if you’re confused by the BRACHIAL PLEXUS! I could never quite remember or understand it—but now I do & I’ll show you how
A #tweetorial on #brachialplexus #anatomy!
#medtwitter #meded #neurosurgery #orthotwitter #orthopedics #neurorad #radres #medstudent #FOAMed
A #tweetorial on #brachialplexus #anatomy!
#medtwitter #meded #neurosurgery #orthotwitter #orthopedics #neurorad #radres #medstudent #FOAMed
2/Everyone has a mnemonic to remember brachial plexus anatomy. I’m a radiologist, so I remember one about Rad Techs. But just remembering the names & their order isn’t enough. That is just the starting point--let’s really understand it
3/From the mnemonic, we start with the roots—the cervical nerve roots. I remember which roots make up the brachial plexus by remembering that it supplies the hand. You have 5 fingers on your hand so we start with C5 & we take 5 nerve roots (C5-T1).

4/Next in the mnemonic are the Trunks. Bc Trunks starts w/T, I can remember how they are named. T is Top to bottom. Trunks are named top to bottom: Superior, Middle, and Inferior. But how to remember which nerve roots combine to give you which trunks?

5/Pairing of the nerve roots into the trunks is like pairing off at a dance when there is an odd number. Everyone immediately turns to the person next to them & the person in the middle is left out. For the roots, C7 is in the middle & has to go it alone as the middle trunk

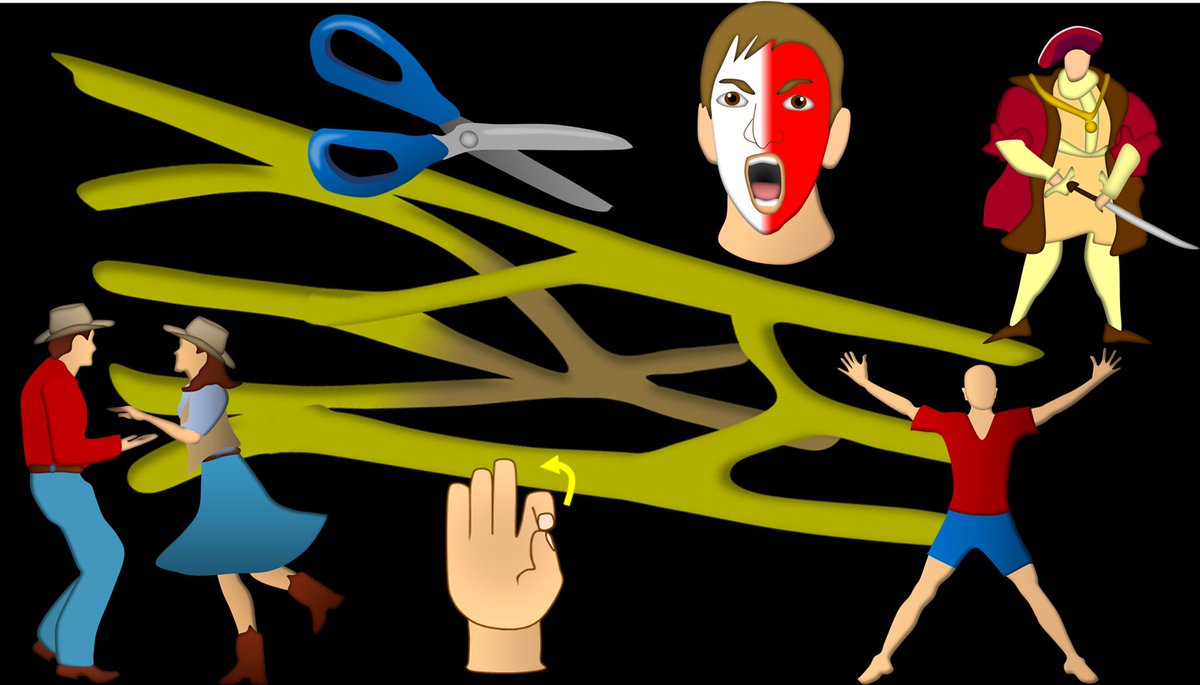
6/Next in the mnemonic are the Divisions. Divisions do what their name implies—they divide the trunks. Each trunk is split or DIVIDED into an anterior & posterior division. Divisions will look like scissors coming off the trunks, helping you to remember they are splitting.

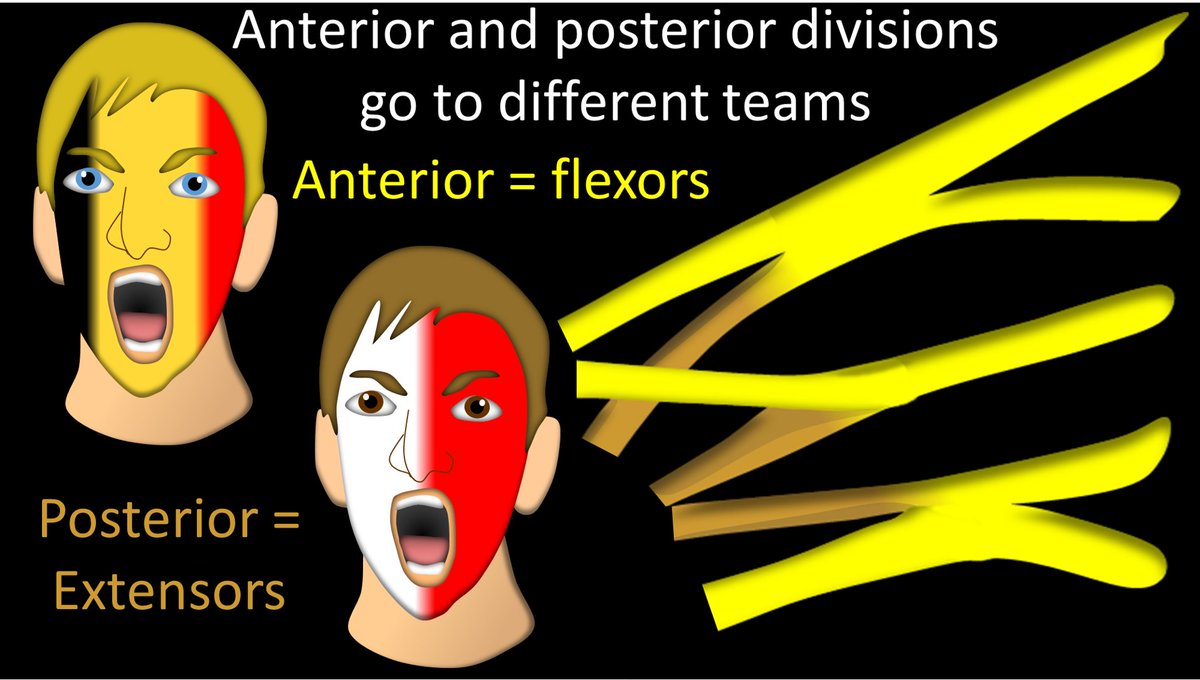
7/This division causes a fundamental change in the nerves—anterior divisions will supply flexors & posterior divisions will supply extensors. This is an important dividing line. Like rabid soccer fans, once they have chosen a team, they will never mix w/fans of the other team
8/After the split of the divisions, the nerves come back together as the cords. It is kind of like doing jumping jacks—they open up and then close back up again. I remember that they come back together as the Cords bc Cords and Combine both start with C

9/It’s like a toll road. The road widens to let more cars get to the toll booths. Once they have paid the toll, road narrows again. This is what happens w/the divisions—but instead of paying a toll, they are organizing into flexor & extensor groups & coming back together again.

10/But it’s more like going through a worm hole than toll booth. When you go through a wormhole, you are fundamentally changed when you come out the other side (or so I read on the internet). Once cords emerge from divisions, they’re either team flexor or extensor & can’t go back

11/So when they form the cords, anterior divisions (team flexor) will only combine w/other ant divisions. Similarly, post divisions (team extensor) will only combine w/other post divisions. It makes sense that post is extensor & ant is flexor, bc muscles are arranged this way too

12/Divisions combine to form 2 ant. cords & 1 post. cord. Why the inequality? Well, the fundamental purpose of the arm is to flex (pick up things), unlike the leg (which is to extend/stand up). So bc it’s more important to flex, remember 2 cords to flexors & 1 to extensors

13/All post divisions go to the 1 post cord
How do you remember which ant divisions go into which cord? Remember, divisions come from sup, middle & inf trunks. Superior or even middle class don’t combine w/inferior things. So sup & mid divisions combine. Poor inferior is alone
How do you remember which ant divisions go into which cord? Remember, divisions come from sup, middle & inf trunks. Superior or even middle class don’t combine w/inferior things. So sup & mid divisions combine. Poor inferior is alone

14/Names of the cords are based on their relationship to the axillary artery. Posterior cord (extensors) is posterior to it. The flexor cord made of the superior & middle divisions is lateral. Flexor cord made from the lonely inferior division is medial

15/But this is hard to remember. So I remember that the flexor cord made from the poor inf division is looked down upon, so it is given the worst seat—at the armpit. In anatomic positioning, closest to the armpit is medial, so it's the medial cord.

16/Now the final division into branches. Remember posterior cord only supplies extensors & is the only extensor cord. So when it branches, it needs to innervate extensors all along the arm (elbow, forearm, hand). So it gives off axillary to the upper arm & radial to the lower arm

17/Now the branches of the flexor cords. As expected from their names, MEDIAL cord gives a branch for flexors/sensation to MEDIAL forearm/hand (in anatomic position = PINKY side, so ulnar nerve), & LATERAL cord gives a branch for motor/sensation to LAT. forearm (musculocutaneous)

18/Usually superior/middle class look down on inferiors (why inf division travels alone as medial cord). But eventually the rich will have, ahem, liaisons w/inferiors.
So it is w/cords. High-class lateral cord finally mingles w/low-class armpit medial cord, making median nerve
So it is w/cords. High-class lateral cord finally mingles w/low-class armpit medial cord, making median nerve

19/Now move beyond mnemonics. Remember, brachial plexus splits & recombines like jumping jacks w/a very palindromic 5-3-6-3-5 pattern.
The names tell you if they are splitting or combining (Trunk=Together, Division=Divide, Cord=Combine, Branch=break)
The names tell you if they are splitting or combining (Trunk=Together, Division=Divide, Cord=Combine, Branch=break)

20/Now all you need is to recall 1 fact @ each stage
Trunk: C7 left out
Div: Ant flexors don’t mix w/post extensors
Cord: Sup/mid class don’t mix w/inferiors
Br: Each cord gives a branch to region its name describes (post, med, lat) &rich give in to inferiors to form median nerve
Trunk: C7 left out
Div: Ant flexors don’t mix w/post extensors
Cord: Sup/mid class don’t mix w/inferiors
Br: Each cord gives a branch to region its name describes (post, med, lat) &rich give in to inferiors to form median nerve

21/Now you know--and understand--the basic anatomy of the brachial plexus.
I know this was too detailed for some & not enough detail for others, but you have to start somewhere!
Next up--the appearance of the brachial plexus on imaging!
I know this was too detailed for some & not enough detail for others, but you have to start somewhere!
Next up--the appearance of the brachial plexus on imaging!
• • •
Missing some Tweet in this thread? You can try to
force a refresh




















