How #COVID actively suppresses and evades your immune system [Part 1]
This thread highlights multiple methods that the virus uses to help keep reinfecting people including MHC-I and interferon suppression, evasion of Natural Killer (NK) cells, and reprogramming of monocytes.🧵1/
This thread highlights multiple methods that the virus uses to help keep reinfecting people including MHC-I and interferon suppression, evasion of Natural Killer (NK) cells, and reprogramming of monocytes.🧵1/

An unrolled one-page web view for this long thread that may be easier to read or share can be found here (
https://twitter.com/jeffgilchrist/status/1611332995012595712). 2/
COVID has been doing this to varying degrees since the beginning which further reinforces that a vaccine only policy is not enough to stop the cycle of sickness, long term disability, and death. 3/
Some people have the privilege of clean drinking water so they do not have to boil their own water for it to be safe because the infrastructure was put in place to clean the water. 4/
We need similar changes in infrastructure now to provide clean indoor air for people, not just from pathogens but from other pollutants as well (
https://twitter.com/jeffgilchrist/status/1607379781892575234). 5/
First some simplified background info, CD8+ T-cells and Natural Killer (NK) cells are both immune system cells with similar goals to kill (cytotoxic) infected and transformed cells but their recognitions and memory mechanisms are very different ( ncbi.nlm.nih.gov/pmc/articles/P… ). 6/
Cells express MHC-I molecules on their surface as a surface recognition element to signal the cell's physiological state to immune cells such as T-cells and NK cells ( pubmed.ncbi.nlm.nih.gov/11256571/ ). 7/
When a cell is infected for example, it will present parts of the virus (antigen) on the surface using MHC-I as a way to alert the immune system for help. 8/
The T-cells look for specific antigens they have been "trained" to find and will bind to a cell that matches and then activate their response such as killing the cell. 9/
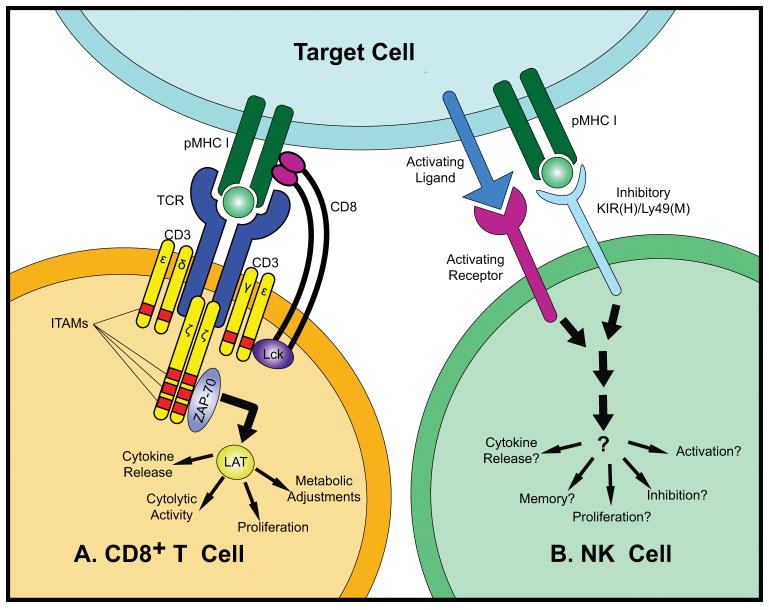
With NK cells however, there is no single dominant receptor for NK cell recognition but they express an array of innate activating and inhibitory receptors to sense their environment and respond to alterations caused by infections, stress, and transformation. 10/

Innate immunity cells are the first responders to sites of infection and NK cells are much quicker to establish a robust response than CD8+ T-cells ( ncbi.nlm.nih.gov/pmc/articles/P…). NK cells can also recruit T-cells and other adaptive responders to the sites of infection. 11/
You can learn more watching this @VirusesImmunity "Immunology 101 for non-immunologists video" ( ) and @Kurz_Gesagt "How your immune system actually works video" ( ). 12/
Now that you have a little background, how does the COVID virus try to avoid the immune system? The newer Omicron variants exhibit an even greater ability to suppress surface MHC-I expression in cells the virus infects ( biorxiv.org/content/10.110… ). H/T: @VirusesImmunity 13/
That means CD8+ T-cells can't as easily "dock" with the infected cell and kill it. The study found multiple variants BA.1, BA.2.12.1, BA.4, and XAF all had significantly higher MHC-I suppression than the original WA1 strain but had no impact in MHC-I on the surrounding cells. 14/

This allows infected cells to be more "invisible" to CD8+ T-cells that otherwise would have been able to find and destroy the cell which lets the virus continue to replicate. 15/
Another study found that COVID virus also suppresses the danger signals that are supposed to help NK immune cells recognize (with their NKG2D receptor) and kill infected cells ( cell.com/cell-reports/f… ). H/T: @m_janelee 16/

COVID virus causes NK cells to exhibit poor cytotoxic (killing) responses to infected cells and instead preferentially target and kill uninfected bystander cells. 17/
The researchers found that NK cells are actually really good at killing COVID infected cells before the virus has had a chance to replicate and suppress NKG2D-L compared to 48 hours after infection (
https://twitter.com/m_janelee/status/1607791318230523906). 18/

The part of the virus that suppresses NKG2D-L to prevent NK cells from killing the cells they infect is Non-Structural Protein 1 (Nsp1). 19/
The researchers found that just putting Nsp1 inside the cell without any other part of the virus was enough to both suppress NKG2D-L and stop NK cells from killing it. 20/
When they tried using various other components of the virus instead, the NK cells kept killing the cells, with most increasing the chance of the cell being killed. 21/
This is yet another way for COVID to get around the immune system with methods to make infected cells more "invisible" to both immune CD8+ T-cells and NK cells. 22/
The researchers point out that the Nsp1 protein in the virus is highly conserved and needed for viral replication so it may make a good target for therapeutics against other families of coronaviruses as well. 23/
Due to genetic variation about 4% of a population studied lacked the NKG2C receptor on NK cells and 30% have the receptor only partially available which had a significant impact on the development of severe COVID infections ( gimjournal.org/article/S1098-… ). H/T: @0bj3ctivity 24/
The study found people without the NK receptor or having a partial receptor were significantly overrepresented in hospitalized patients, particularly in patients requiring intensive care compared to those with mild symptoms. 25/
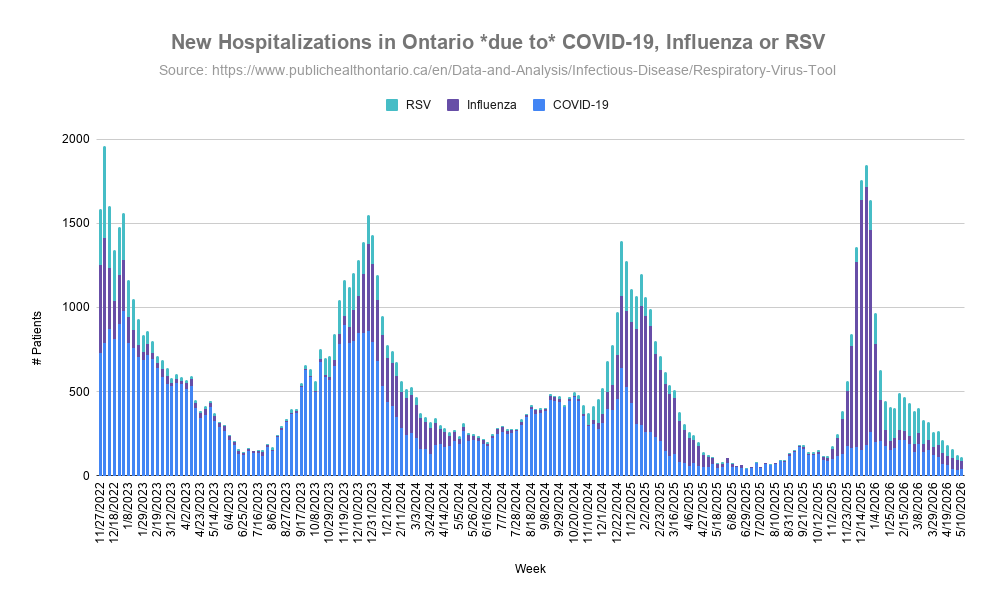
These multiple methods of immune suppression and evasion by COVID help explain why viral loads can get high enough again in people that are previously infected/vaccinated to become contagious and transmit the virus to others before the body can get the infection under control.26/
Part 2 will look at how the COVID virus reprograms innate immune functions such as white blood cells (monocytes) that increase the risk of blood clots and suppresses innate immunity to other viruses and bacteria increasing risk of secondary infections. 27/
To add some context to tweet 26/ for people who are vaccinated or previously infected, even though your immune system has seen a COVID variant before and you already have T-cells that can recognize the virus... 28/
...the new variant you are exposed to can suppress the mechanism that those T-cells (and NK cells) use to identify and kill COVID infected cells giving the virus time to replicate a lot before other parts of the immune system notice and start fighting off the virus. 29/
That is why people can't "vax and relax" forgoing all other precautions because exposure again can still give the new virus infection a chance to replicate enough to cause trouble in your own body and also potentially infect other people too. 30/
Some people are asking, why does this immune suppression happen to people who have been vaccinated and never infected before as well as people who have been infected already? Click "Show replies" 👇 to continue. 31/
It is happening to all people because the mechanism to evade and suppress the immune system that I describe in this thread is the ability of the virus itself to turn off/reduce the ability of CD8+ T-Cells and NK immune cells from detecting the cells it has infected. 32/
This allows the virus to fly under the radar, vaccinated or not. If you get infected, among many things, your body develops T-cells that recognize the virus Spike protein. When you get vaccinated, you also develop T-cells but without getting attacked by a functional virus. 33/
When you get infected again (or first time after vaccination) those T-Cells are trying to specifically hunt down and kill COVID infected cells it already learned about but they can't easily find them and kill them because... 34/
...the new virus infection is blocking the ability for the T-cell to do that. So this happens in both scenarios. 35/
Without needing to know about the COVID virus specifically, immune NK cells also try to hunt down and kill any infected cells, but again COVID developed a way to prevent NK cells from finding them and doing this effectively. 36/
The evasion is a property of the virus itself so it happens with all people who get exposed, the virus hides from the immune system whether you are vaccinated or not, previously infected or not. 37/
Think of the COVID virus as a Ninja, it can sneak into your castle and hide even if the guards have seen Ninja before and defeated them. The guards can't fight them unless they know they are there in the first place and where to find them. 38/

Part 2 which looks at how mild and moderate #COVID infection reprograms white #blood cells (#monocytes) to reduce #innate #immune functions and how it evades the mucus layer in our #nose is now available (
https://twitter.com/jeffgilchrist/status/1612066649934290946). 39/
• • •
Missing some Tweet in this thread? You can try to
force a refresh