
1a) Welcome to a new #accredited #tweetorial, “MOA and Clinical Trial Data for Novel & Emerging Therapeutic Strategies for #HCM: Can We Target Our Therapy?" 

1b) Our expert (and returning @cardiomet_ce) author is Giuseppe Galati MD, MMSc in Heart Failure, FHFA, @GiuseppeGalati_ , Consultant #Cardiologist #HeartFailure & #Cardiomyopathies

2) @GiuseppeGalati_ is in Milan 🇮🇹 This program is intended for #healthcare professionals & is accredited for 0.75h CE/#CME credit for #physicians #physicianassistants #nurses #nursepractitioners #pharmacists.
3) This program is supported by an educational grant from Bristol-Myers Squibb. Statement of accreditation and author disclosures at cardiometabolic-ce.com. See prior #tweetorial in this series from @MasriAhmadMD, still available for credit, at cardiometabolic-ce.com/hcm1/.

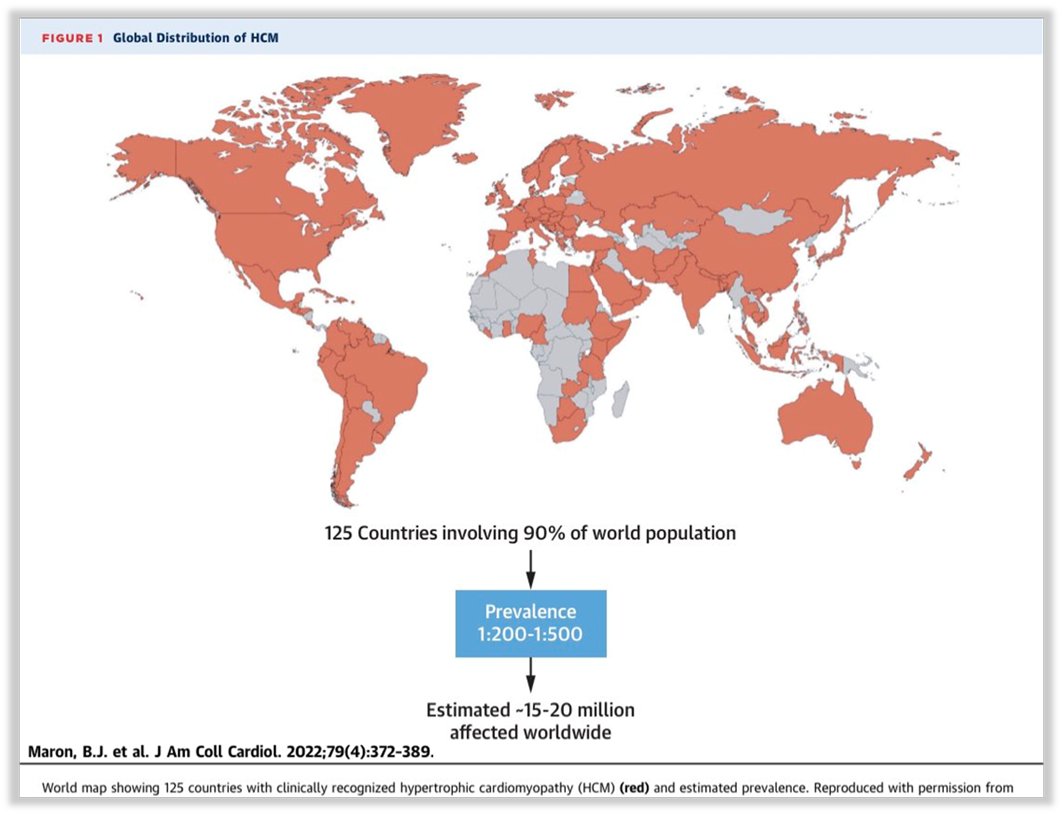
4) #HypertrophicCardiomyopathy (#HCM) is one of the most frequent inherited cardiovascular diseases (Prevalence between 1:200 & 1:500 globally). #HCM inheritance is autosomal dominant, its distribution of HCM is equal by sex, although women and black American are underdiagnosed.
5) Although the natural history of #HCM is benignant in the majority of cases (~70-75% of patients), other patients can develop #SuddenCardiacDeath, #HeartFailure, #AtrialFibrillation and #Stroke and #InfectiveEndocarditis
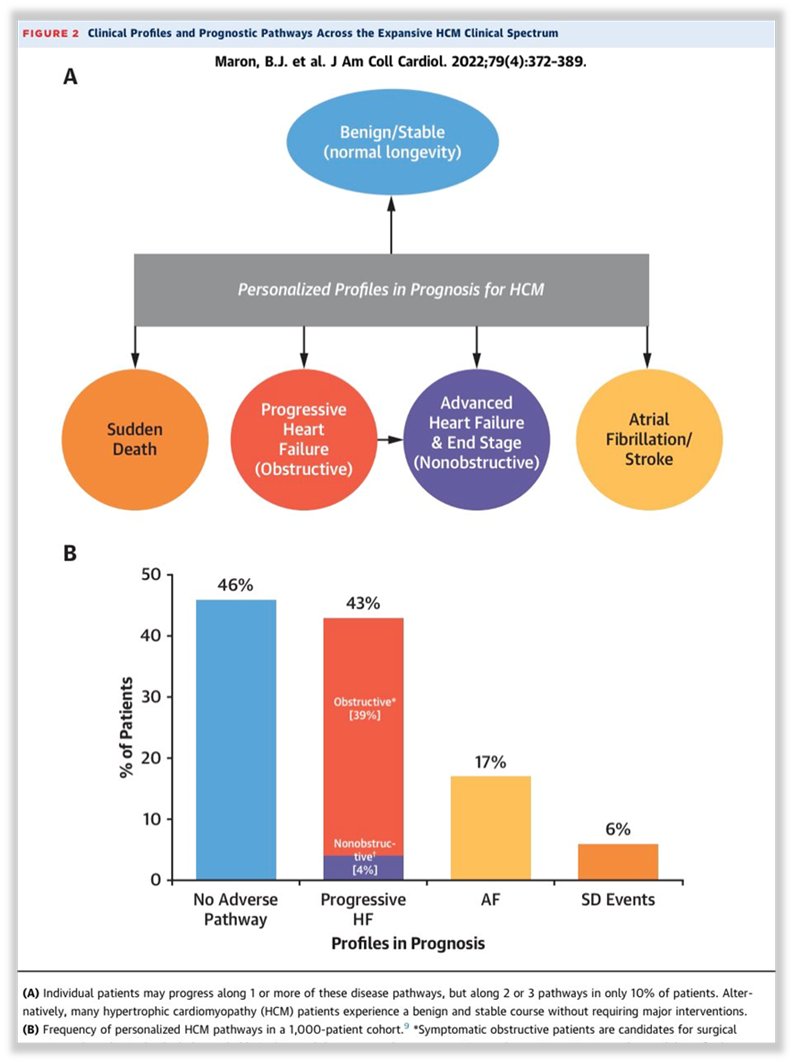
6) #HeartFailure in #HCM has 3 main clinical and morpho-functional profiles:
👉 #HOCM (obstructive)
👉 #HNOCM with #HFpEF (no LVOTO)
👉 #End_StageHCM (#LVEF<50%)
👉 #HOCM (obstructive)
👉 #HNOCM with #HFpEF (no LVOTO)
👉 #End_StageHCM (#LVEF<50%)

7) More than 2/3 of #HCM patients (~75%) have a #LVOTO at rest or during exercise and they are affected by #HOCM (#HypertrophicObstructiveCardiomyopathy). Less than 1/3 are affected by #HNOCM.

8) Two main mechanisms are responsible for #LVOTO & for systolic anterior motion (#SAM) of the anterior leaflet of mitral valve (MV): 1⃣ septal hypertrophy with narrowing of the LVOT, leading to dynamic aspiration (Venturi’s effect) of the MV.

9) 2⃣ anatomic alterations in the MV including longer leaflets as well as anterior displacement of the papillary muscles & MV apparatus. #LVOTO in HCM is dynamic and sensitive to ventricular load and contractility.
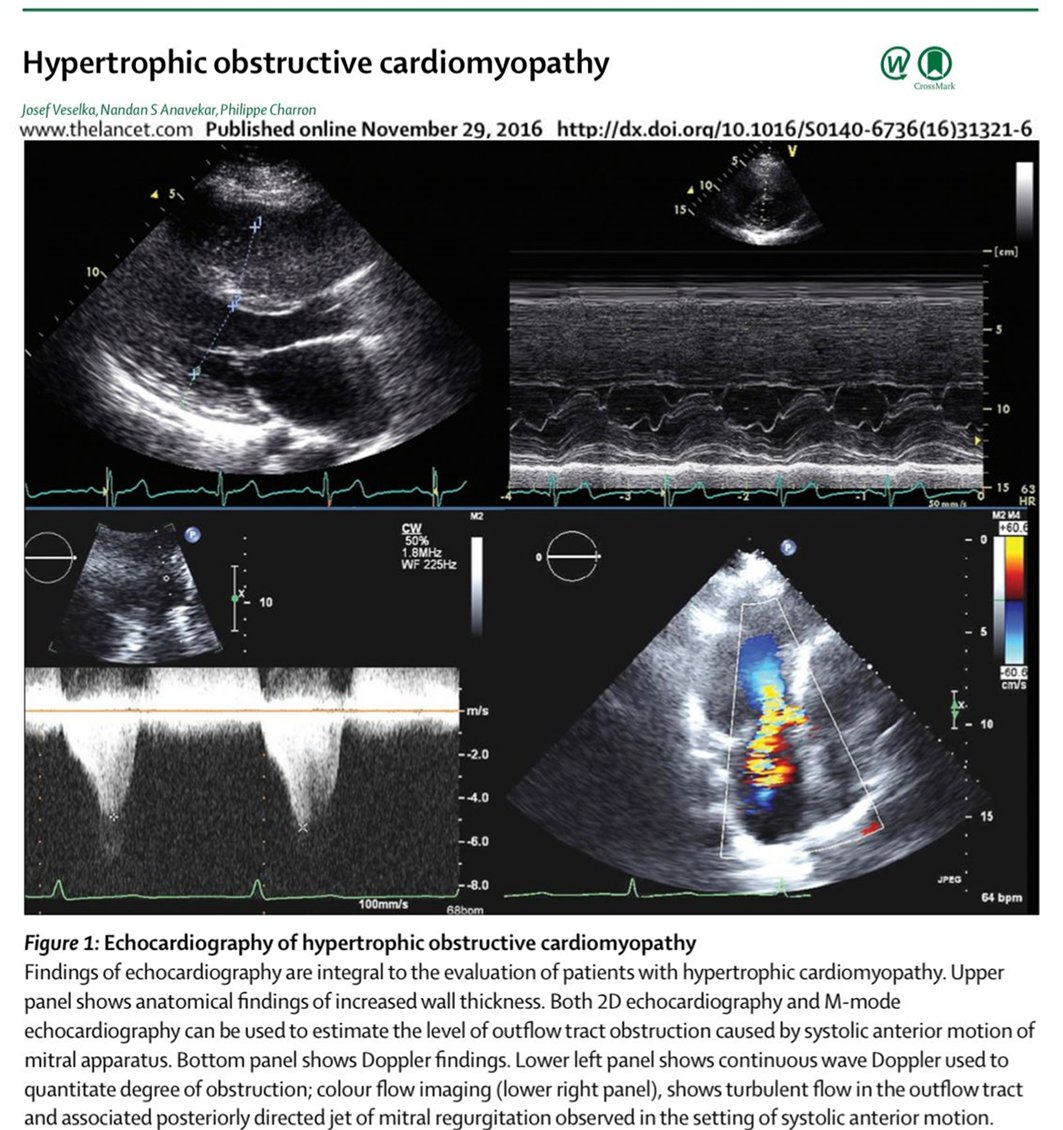
10) By convention, #LVOTO defined as peak Doppler LVOT gradient ≥30 mm Hg at rest or during provocation e.g. Valsalva maneuver standing & exercise. Per last #ESCguidelines a gradient of ≥50 mm Hg is considered to be haemodynamically significant & the threshold for starting tx.

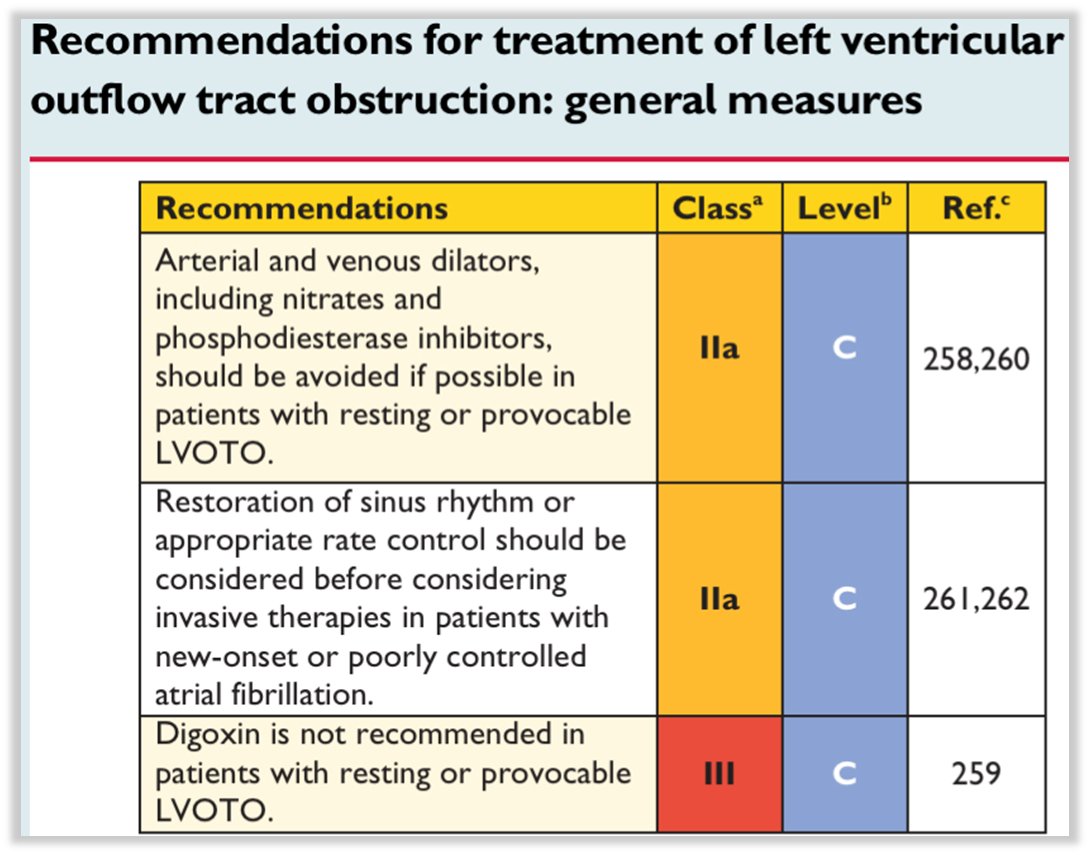
11) The “historical” management endorsed by the last (2014) #ESCguidelines include general maneuvers (such as avoiding specific drugs) and 1st and 2nd line drugs, i.e.: beta-blocker, Ca2+-channels blockers, disopyramide alone or in combination.

12) Similar (nearly identical) recommendations have been endorsed by the last AHA/ACC 2020 guidelines, with the indication extended for the #non_dihydropyridine calcium blocker #diltiazem that has been not mentioned by the @ESCardio guidelines.
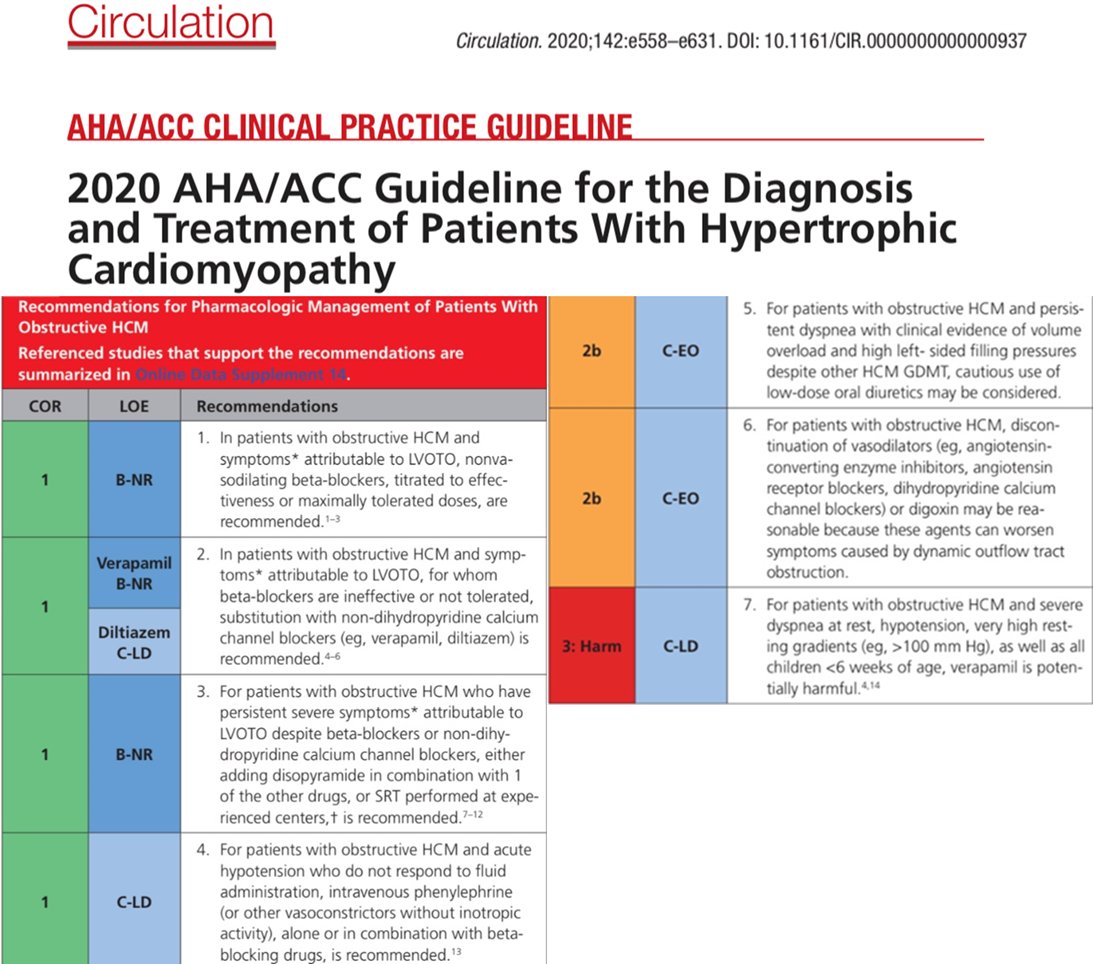
13) Also the therapeutic algorithm endorsed by the American guidelines was very similar to that endorsed by the European guidelines and reflected no significant improvement until 2020 on the management of #HOCM.

14) Although effective, ß-blockers are not w/o side effects, especially in young pts such as those with #HCM. These include: bradycardia, AV blocks, asthenia, hypotension & erectile dysfunction. Ca+ channel blockers can cause: bradycardia, AV blocks & rarely, pulmonary oedema.
15) Finally, #disopyramide (used as 2nd or 3rd line therapy often in association) has as main limitation anticholinergic side-effects e.g. dry eyes & mouth, urinary retention, & constipation. Moreover, #QTc prolongation is not rare & should be monitored during dose up-titration.

16) Therefore, #disopyramide should be avoided in glaucoma, men with prostatism, & patients taking other drugs that prolong the QTc interval. Another caution (as Class IA antiarrhythmic) is #AFib in whom drug-induced enhancement of AV conduction can increase the ventricular rate.

17) Moreover, pharmacological tx can be poorly effective in ⬇️LVOTO, ➡️ #HOCM pts may need #septal_myectomy (SM) or alcohol septal ablation (ASA). A less effective option can be dual chamber pacing: AV sequential pacing w/short AV interval (100+30 ms) to⬆️ RV apex pre-excitation


18a) There are no RCTs comparing SM & ASA, but several meta-analyses have shown that both procedures improve functional status with similar mortality. #SM should be performed at experienced centers for the highest effective therapy.
18b) Complications includes #AVblock, LBBB & more rarely Ventricular septal defects #VSD & aortic regurgitation.
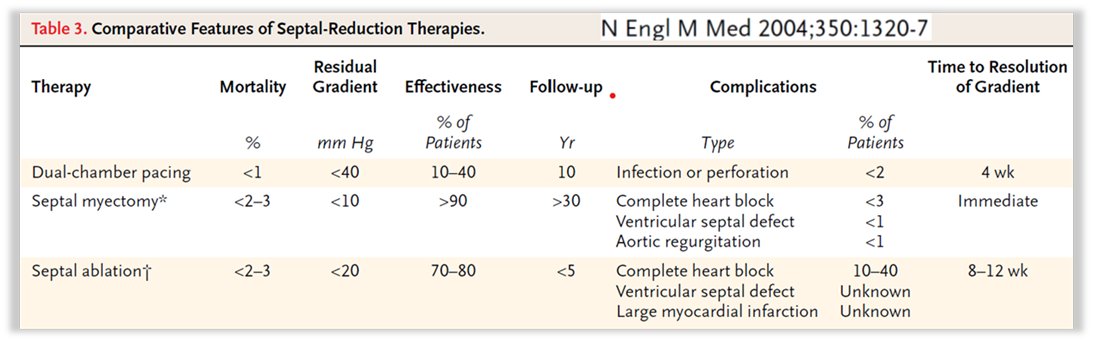
19) ASA is slightly less effective, complications includes the same of SM (no AR & more RBBB than LBBB)+ inefficacy & need for redo, large scars with Ventricular Tachycardia #VTach & End-Stage #HCM evolution. It should also be performed in experienced centers.

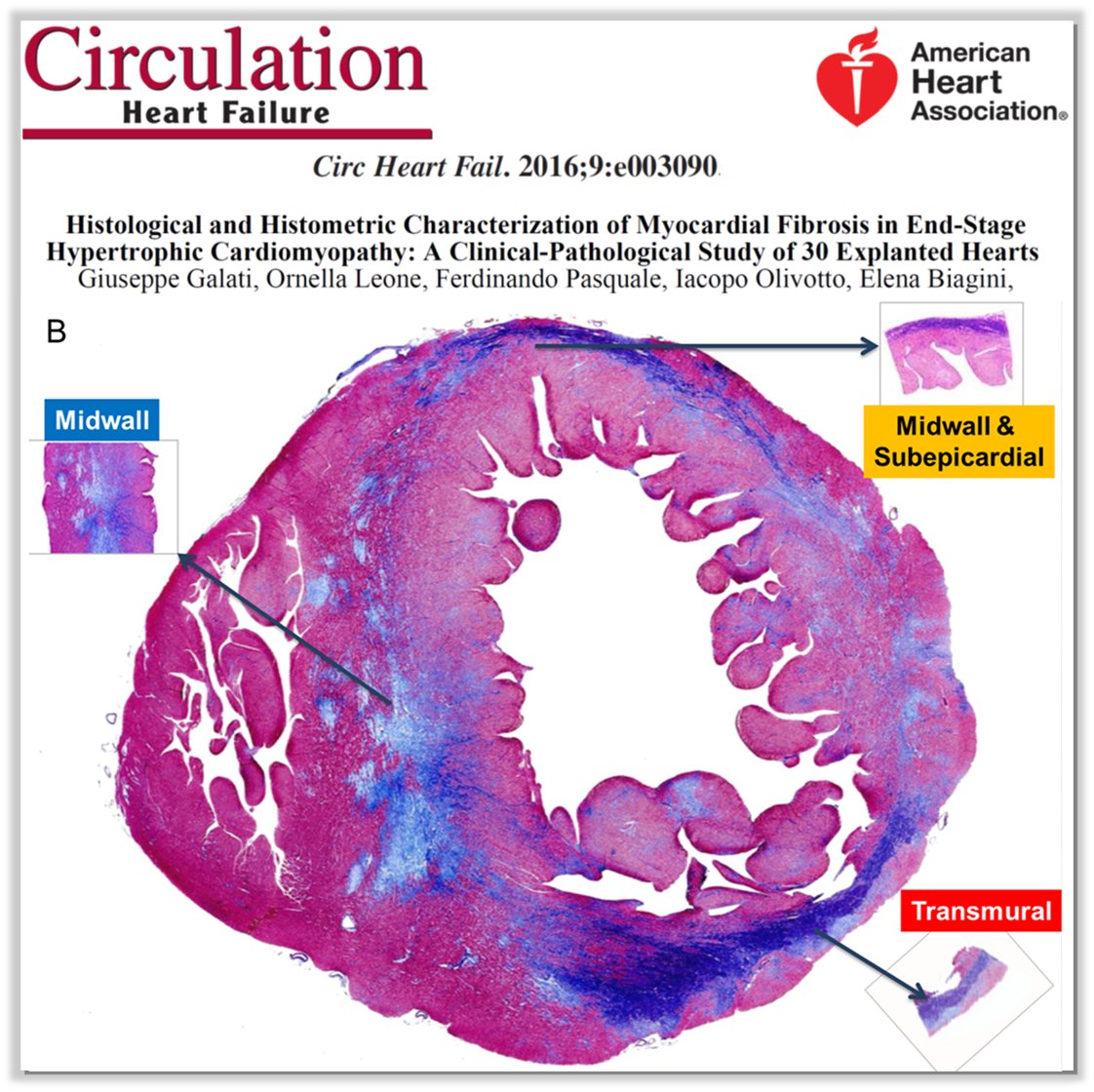
20) #EndStage #HCM evolution (or “burn-out” or hypokinetic) can be a complication of these procedures (mainly of ASA when performed in less experienced centers). This is defined by #HCM w/ #LVEF≤50%, has ⬆️mortality & is characterized by extensive amount of #myocardial_fibrosis
21) SM has as advantage the possibility to correct MV apparatus abnormalities. Historically, it has been coupled to MV replacement, but w/ the need for greater complexity & time of surgery. Recent series show that SM + MV repair w/ secondary chordae cutting is effective & safe

22) Here the recent recommendations from last AHA/ACC @American_Heart / @ACCinTouch Guidelines on #HCM.

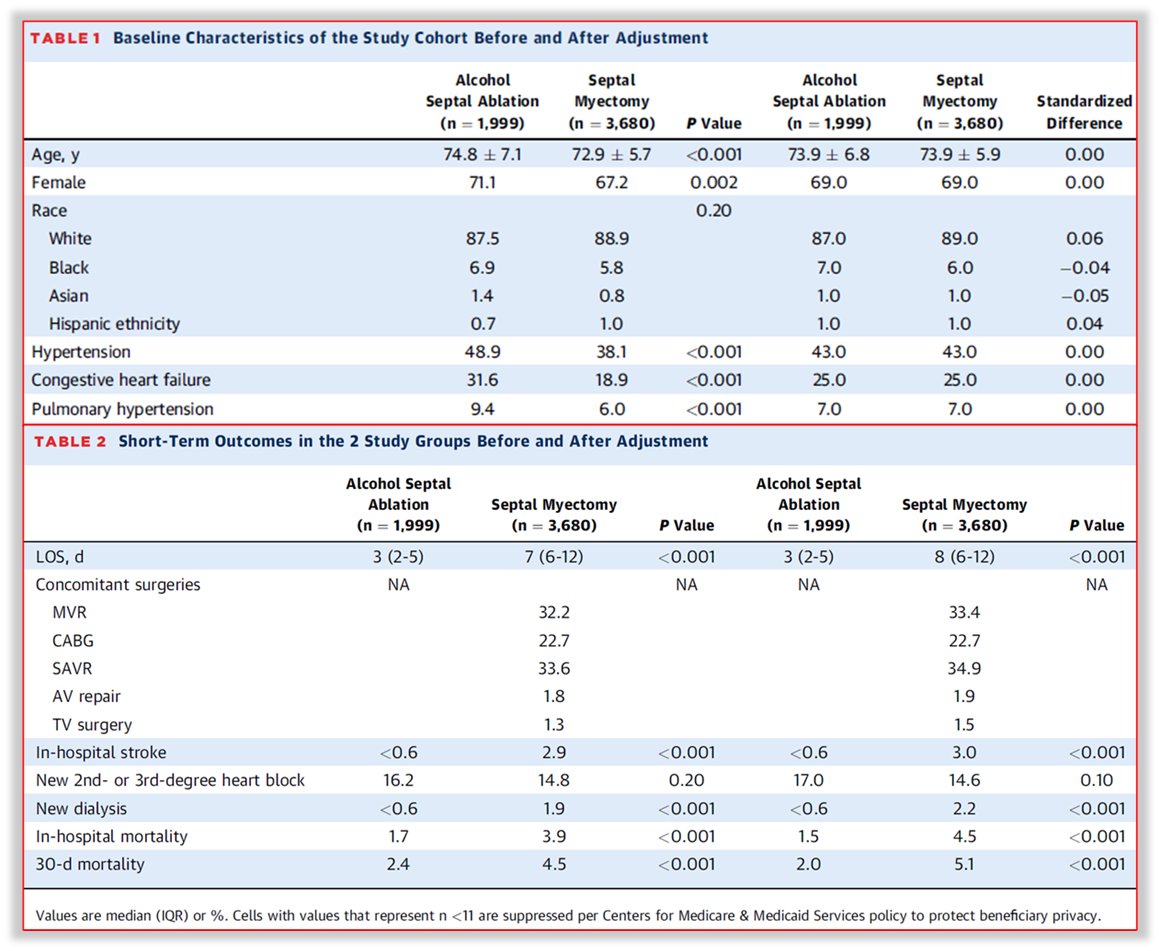
23) A very recent study on 5,679 #HOCM pts reported & compared outcomes in 🇺🇸 centers of SM vs ASA from 2031 to 2019 on old pts (mean age ~ 73 y). They showed good survival for both procedures but⬆️survival for SM at 5 & 6 y. Both procedures⬇️#HF🏥& ASA has higher need for redo.


24a) So what have you learned? #HOCM has an established historical management encompassing both pharmacological & not pharmacological therapeutic options.
24b) What are the implications for patients?
a) None, the problem is solved
b) They are both effective but with several limitations
c) There is a need for improving the #HOCM management
d) B + C correct
a) None, the problem is solved
b) They are both effective but with several limitations
c) There is a need for improving the #HOCM management
d) B + C correct
25) Enter your response & return TOMORROW for the correct answer & the remainder of this #accredited #tweetorial! 👍to @GoggleDocs @DrMarthaGulati @BiykemB @mmamas1973 @SABOURETCardio @iamritu @gcfmd @hvanspall @JJheart_doc @gbiondizoccai @ValleAlfonso
26a) Welcome back! I am @GiuseppeGalati_ and we are talking about management of #HCM. You are earning 0.75hr 🆓CE/#CME. Follow us for your only source of #accredited #cardiometabolic education delivered wholly on Twitter. Always expert 🎓authors, always 🆓
26b) Yesterday's knowledge ✔️? Scroll back up to 25) & answer if you didn't already! The answer is D, both B & C. Both are effective but with limitations & there’s an unmet need for medical #HOCM management covered today by #macacamtem & perhaps in the future also by #aficamtem.
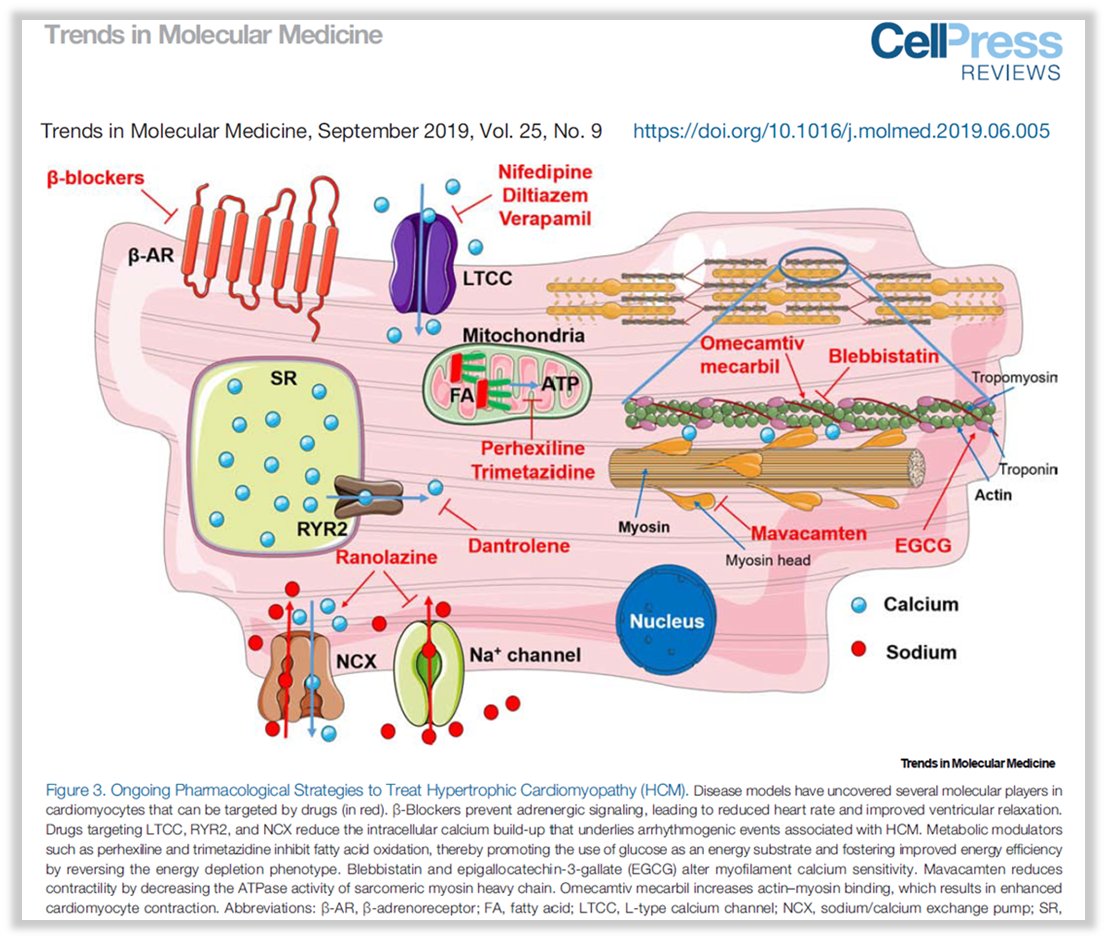
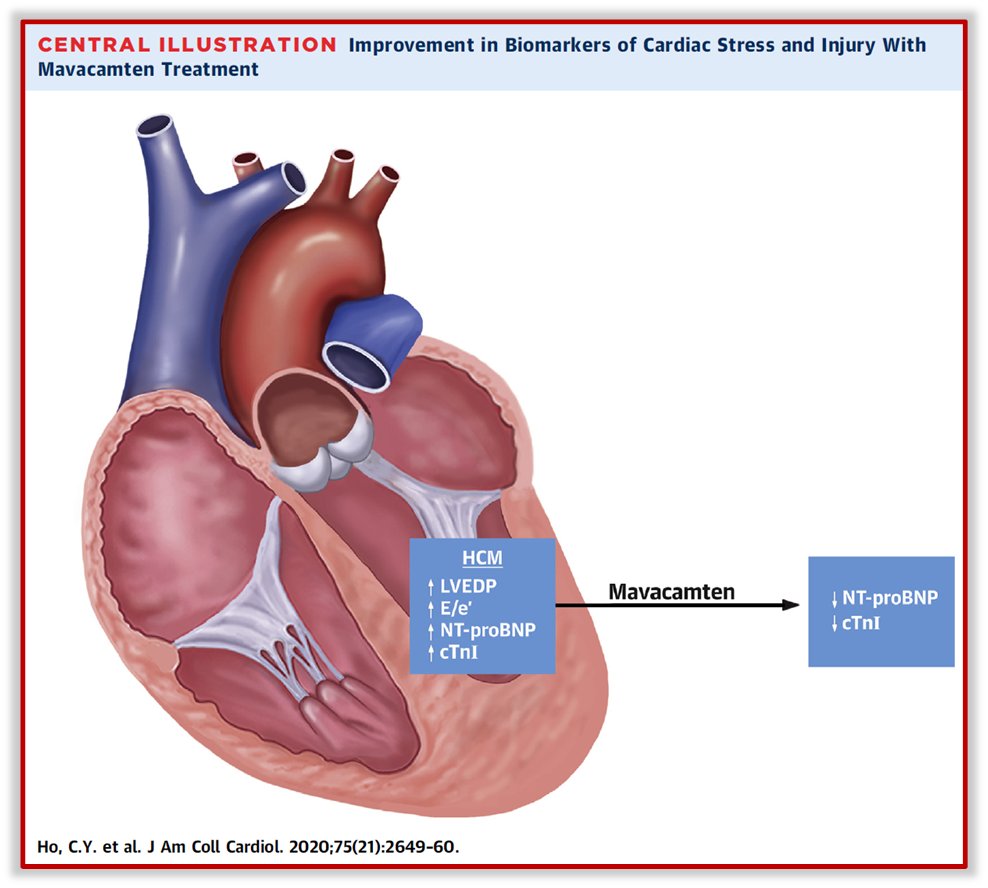
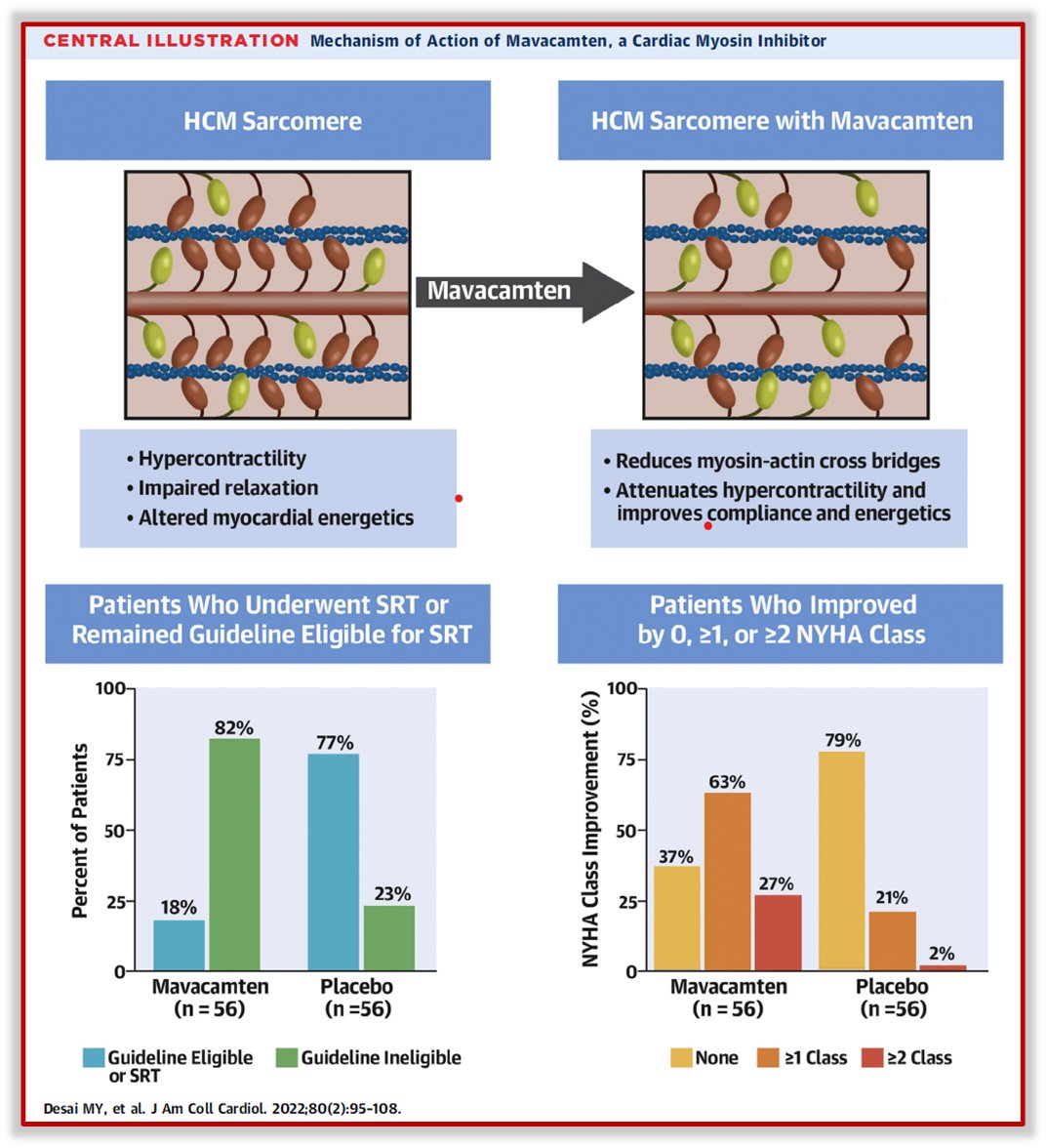
27a) #Mavacamten is the 1st cardiac myosin inhibitor that ⬆️ the super-relaxed state of myosin. It ⬇️ hypercontractility & ⬆️ compliance & myocardial energetics. It prevents hypertrophy & ⬇️ #myocardialfibrosis & myocyte disarray in #HCM.

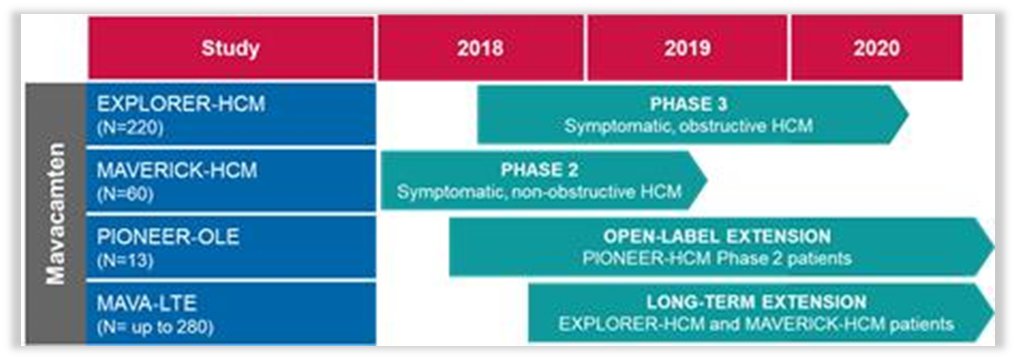
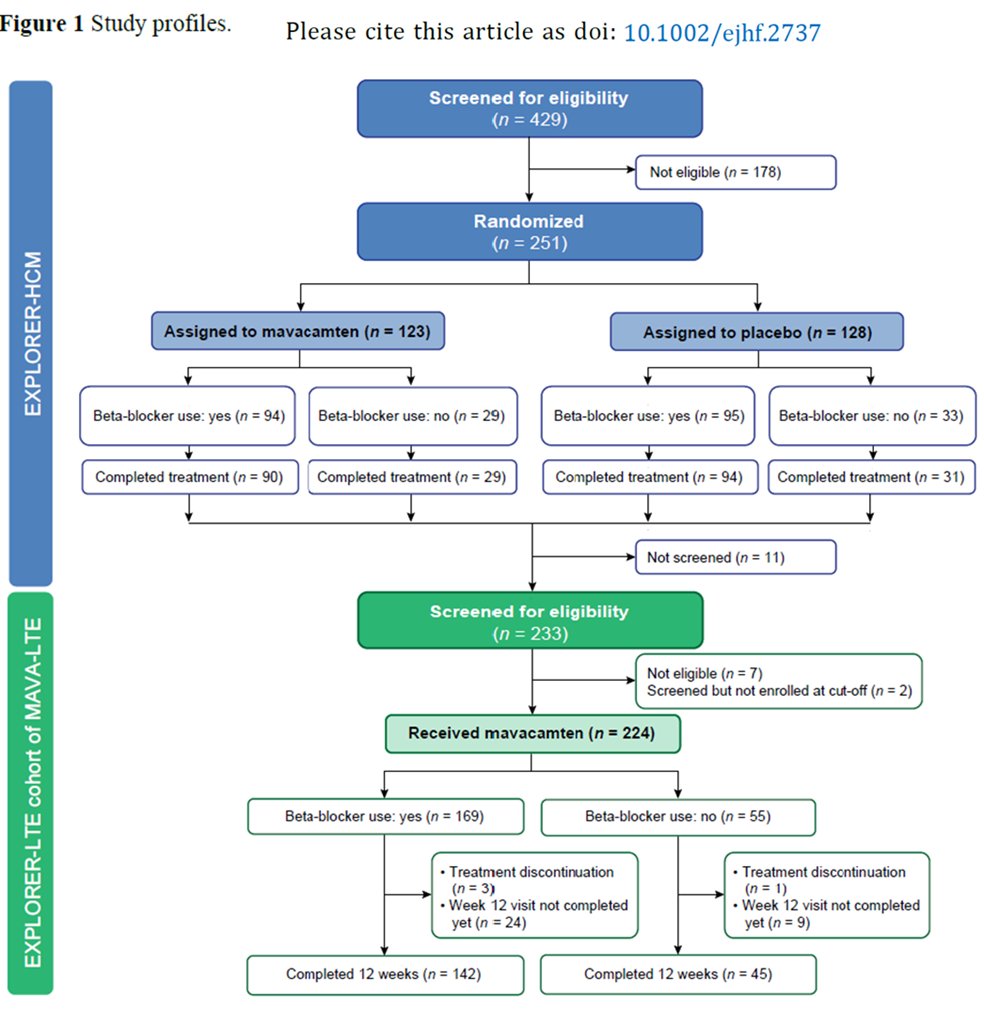
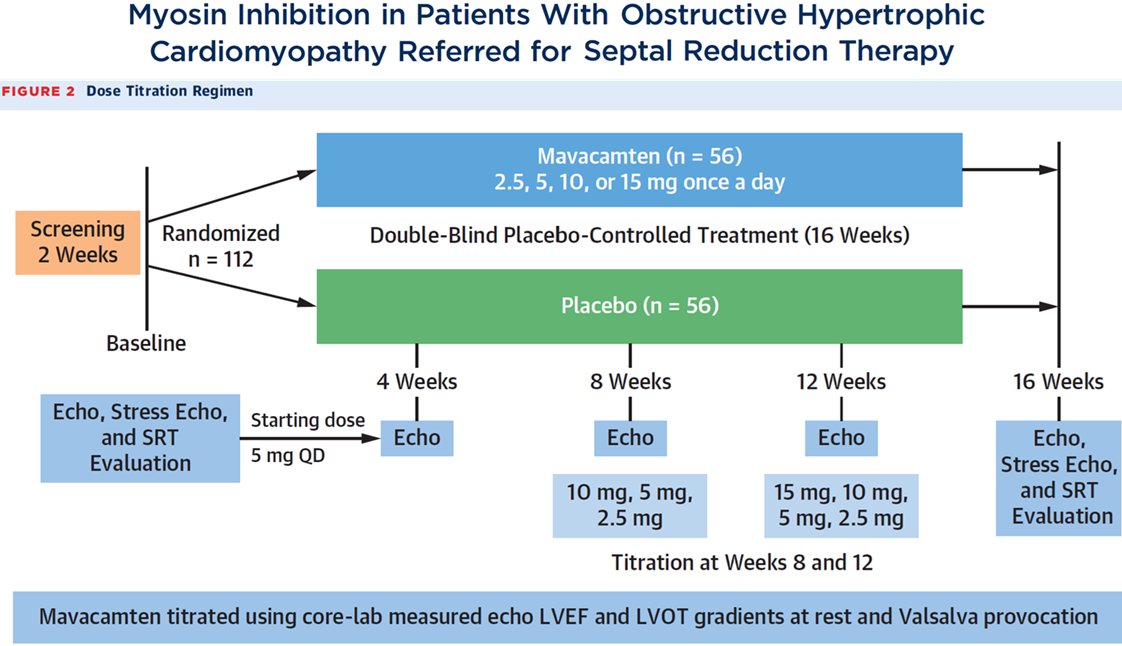
28) #EXPLORER_HCM enrolled 251 pts with the following characteristics ⤵️. #Mavacamtem has been added on top of a beta-blocker (75%) or of a Ca+ channel blocker (16.7%) and has been up-titrated from 2.5 mg to a maximum of 15 mg per day (OD).

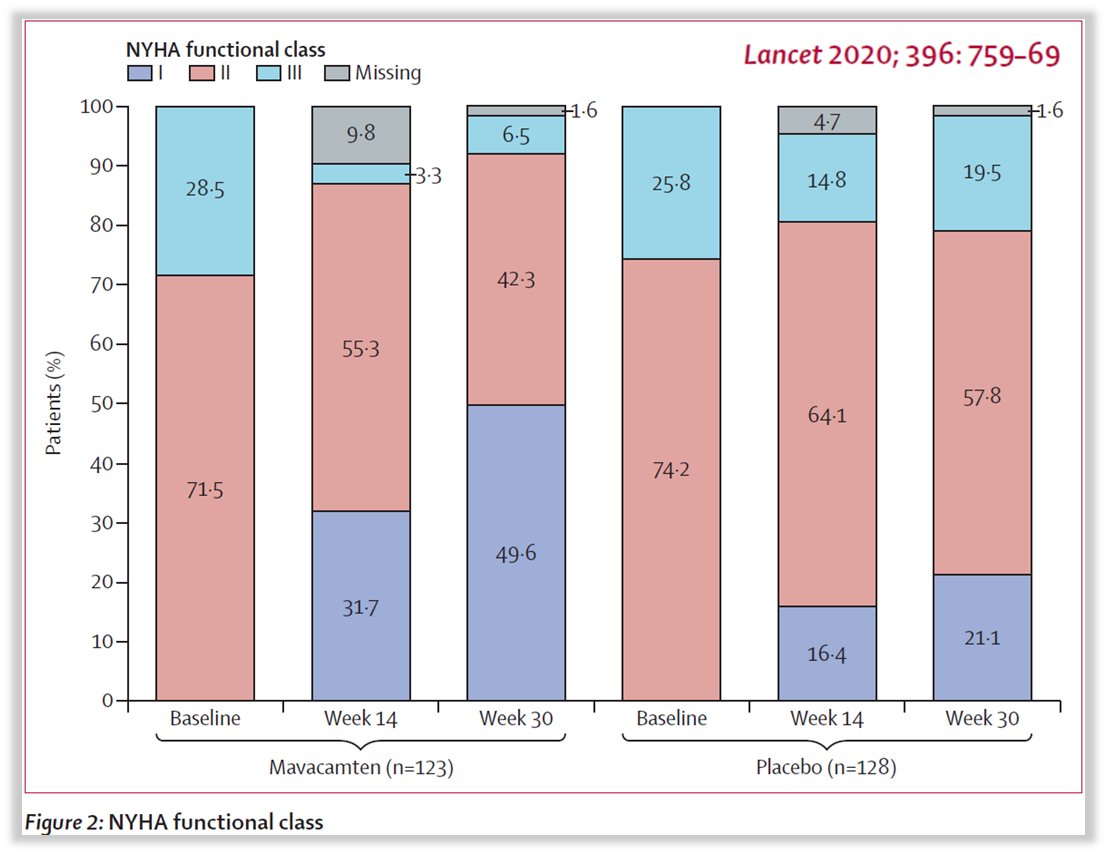
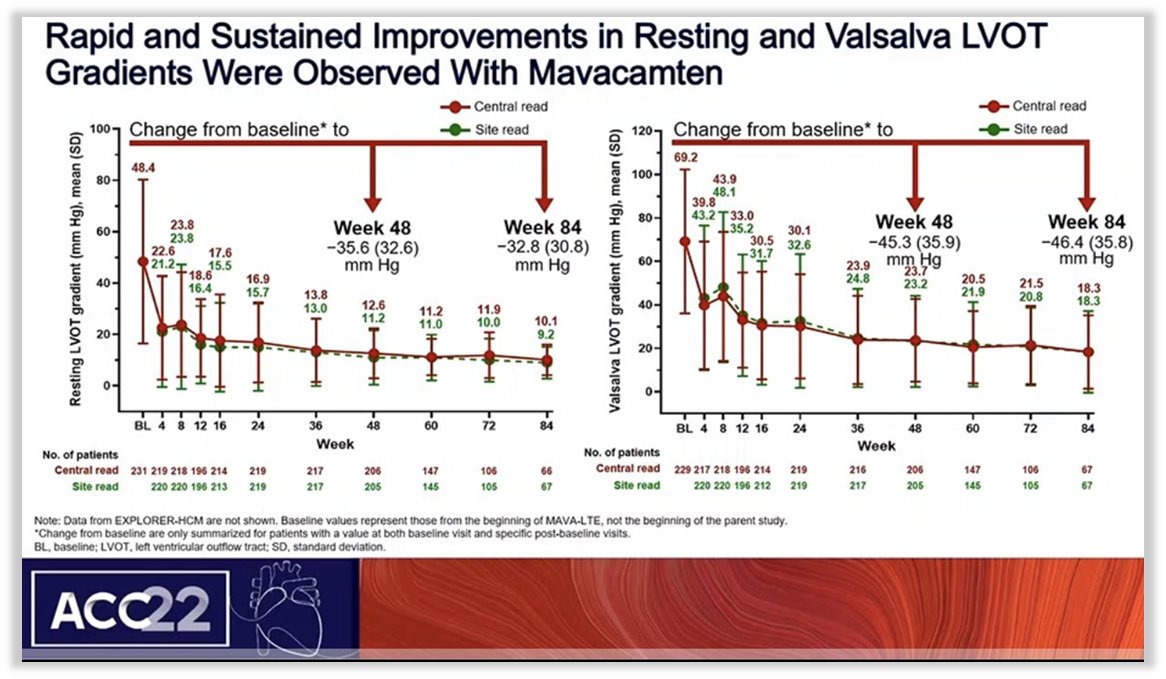
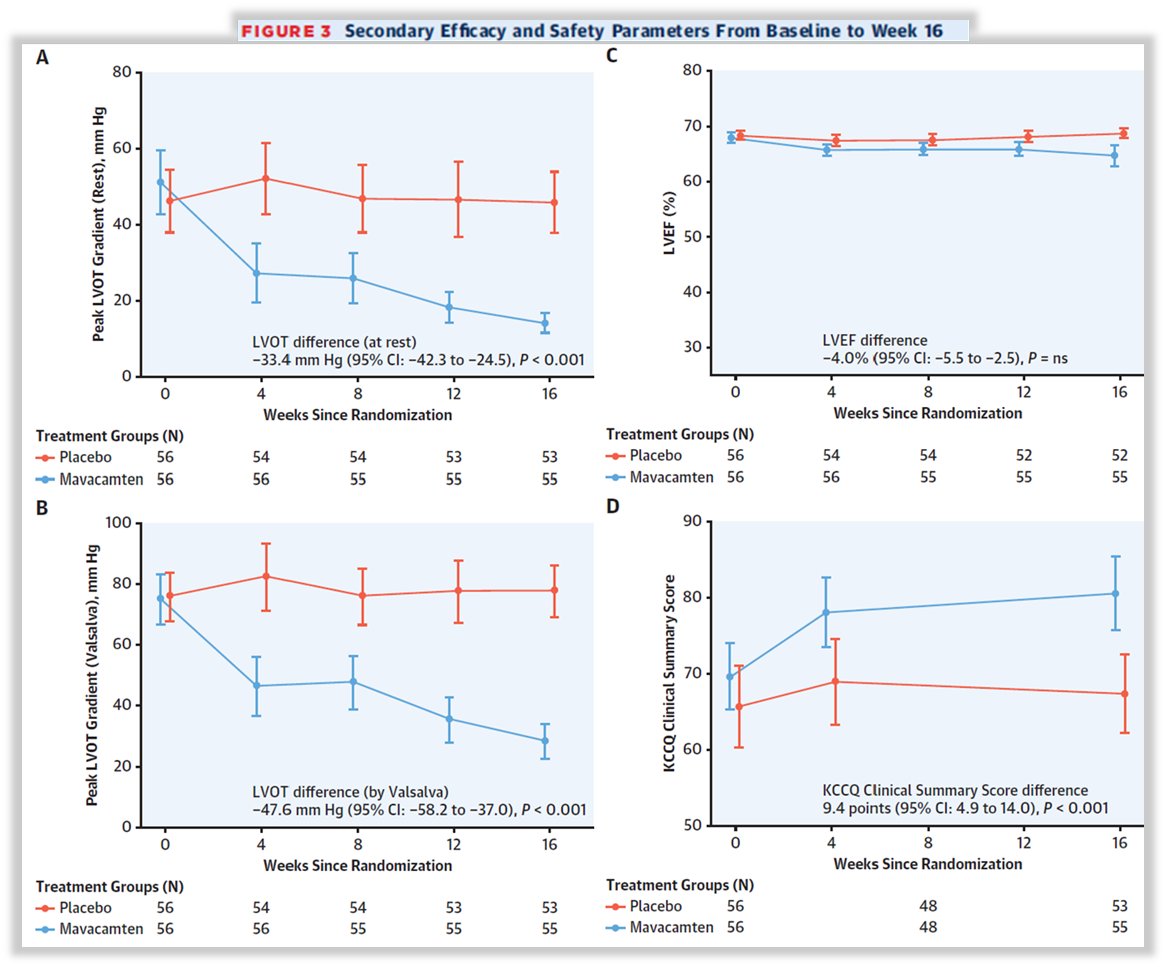
29) In #EXPLORER_HCM #mavacamtem was shown to significantly improve both Primary EPs (peak VO2 as determined by #CPET & an improvement of ≥ 1 NYHA class) & Secondary EPs (⬇️LVOT gradient,⬇️NYHA class,⬆️#QoL measured by #KCCQ). Moreover, it⬇️#NTproBNP & #hs_TnI


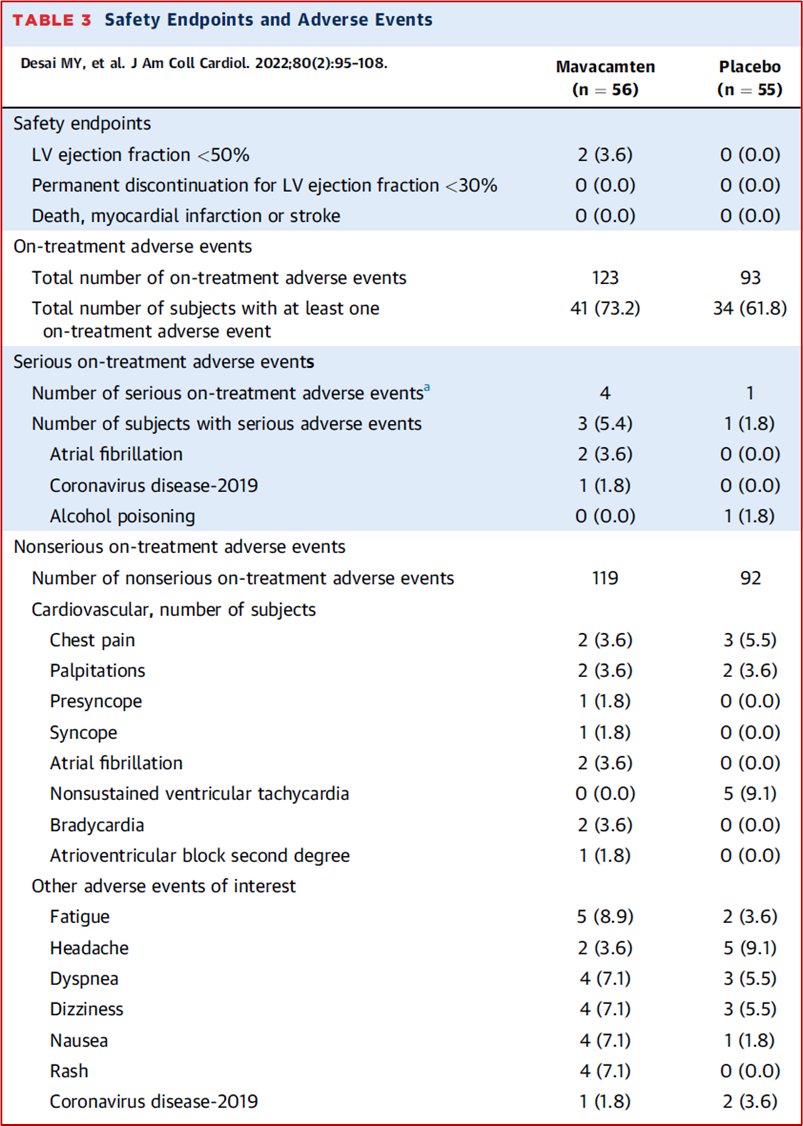
30) The safety profile of #mavacamtem in #EXPLORER_HCM was high, as reported in the table related to the #AdverseEvents (#AEs) ⤵️

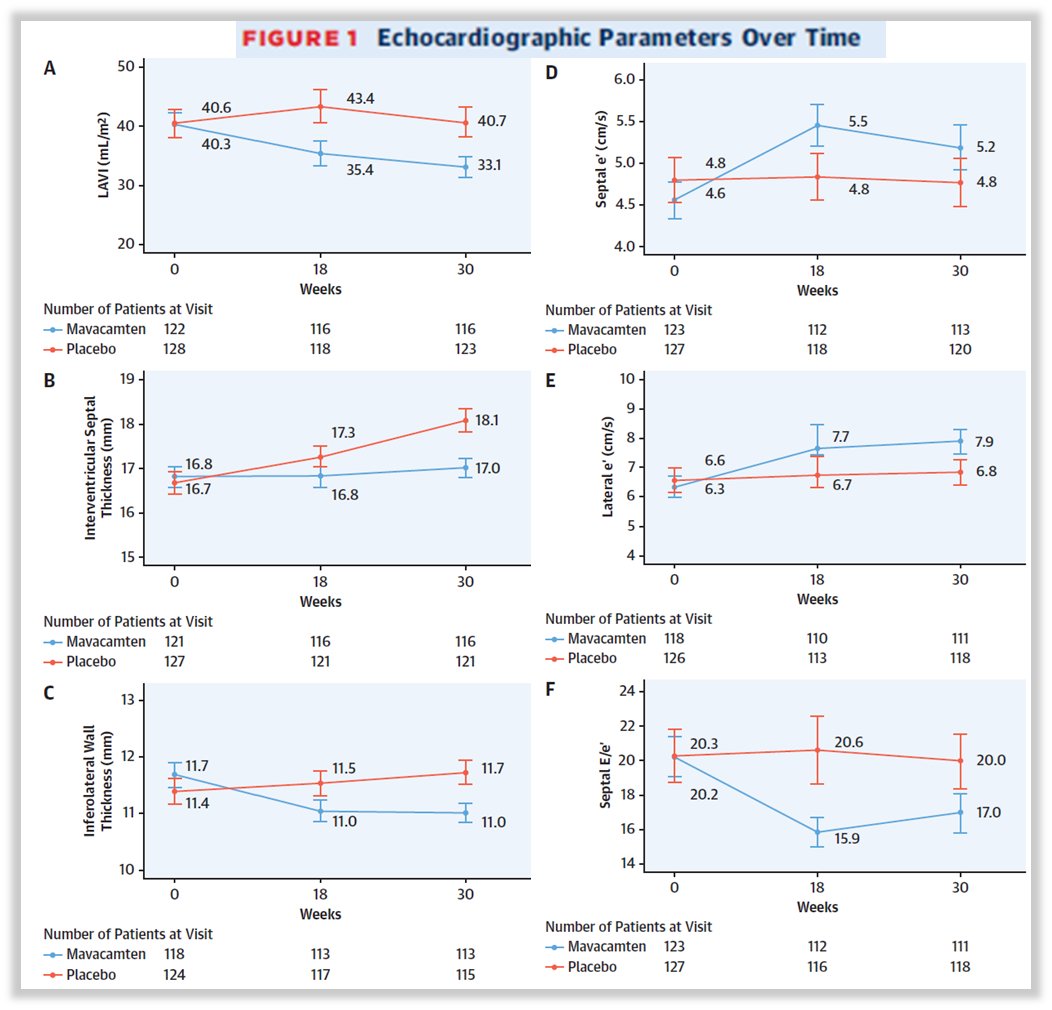
31) An #EXPLORER_HCM ECHO substudy showed beyond the significant reduction of #LVOTO (see above) a slight ⬇️ of #LVEF a ⬇️of ventricular hypertrophy & ⬆️of diastolic function.


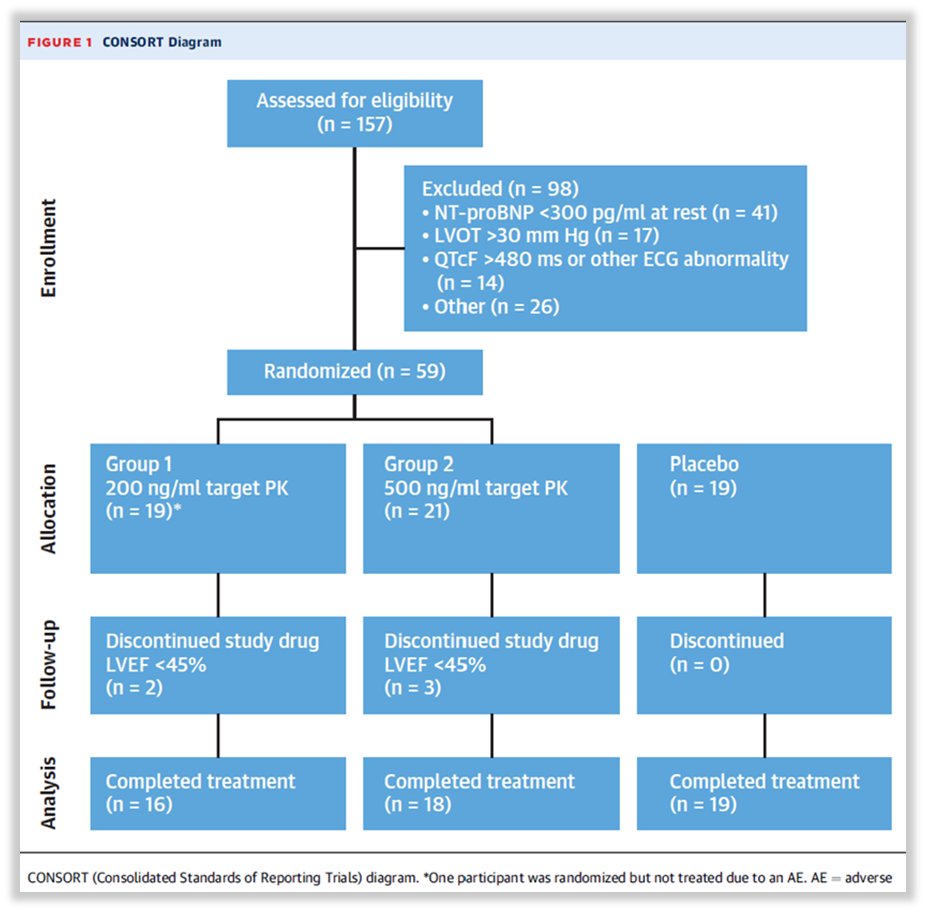
32) In 2020 #MAVERICK, a Ph 2 #RCT dedicated to #HCM without #LVOTO, confirmed significant biomarkers⬇️&⬆️of diastolic function. 8% of pts on #mavacamtem discontinued the drug because of LVEF⬇️. Considering that was a Ph 2 RCT safety & efficacy were good, but we wait for Ph 3 RCT

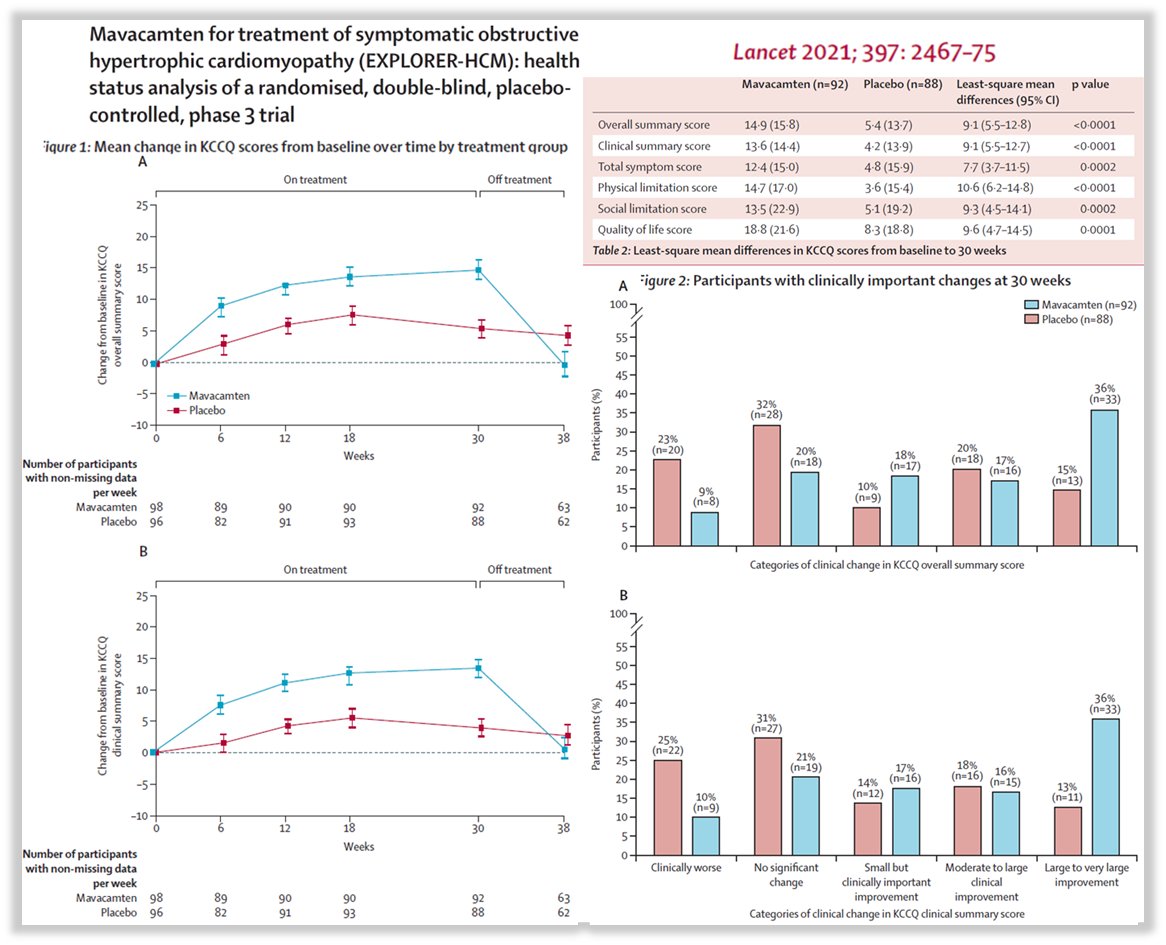
33) A health status analysis of #EXPLORER_HCM showed significant ⬆️ #QoL measured by #KCCQ with clinical improvement from moderate to large and to very large. These improvements started immediately after the start of the drug & lasted for all the observational follow-up (30 wks)
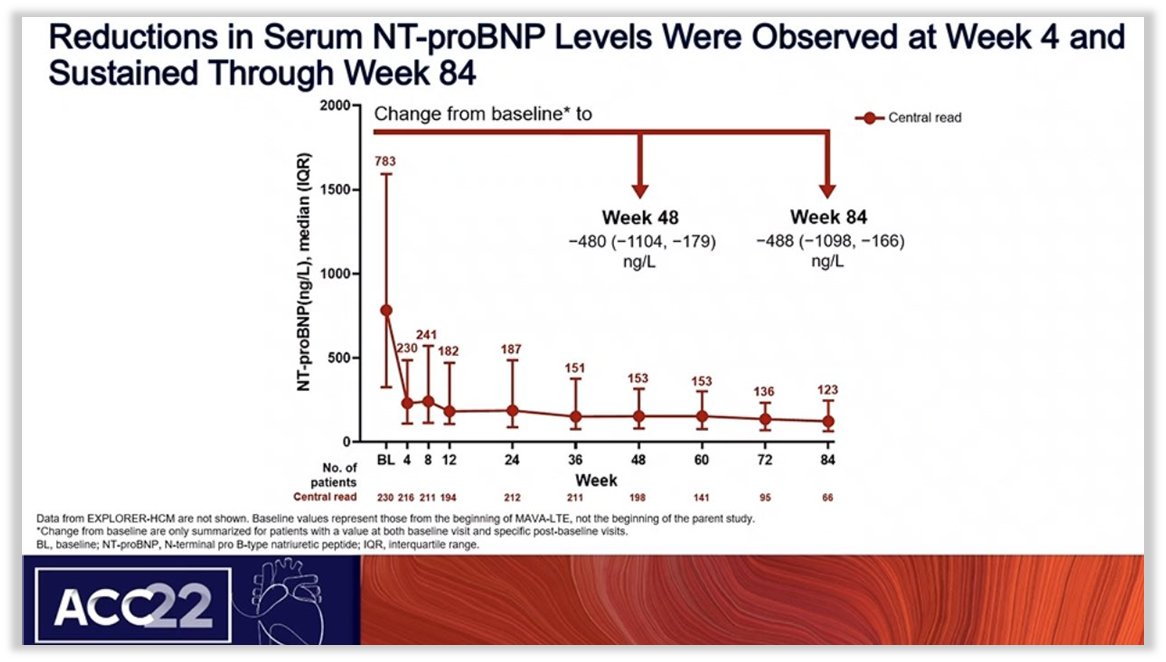
34) An interim analysis of #EXPLORER_LTE part of #MAVA_LTE at last #ACC22 confirmed #mavacamtem benefits at a median follow-up of 62 w. The drug confirmed a good safety profile 11% of pts discontinued the drug because of AEs & 5% because of⬇️LVEF<50%
👉 shorturl.at/oUZ24
👉 shorturl.at/oUZ24


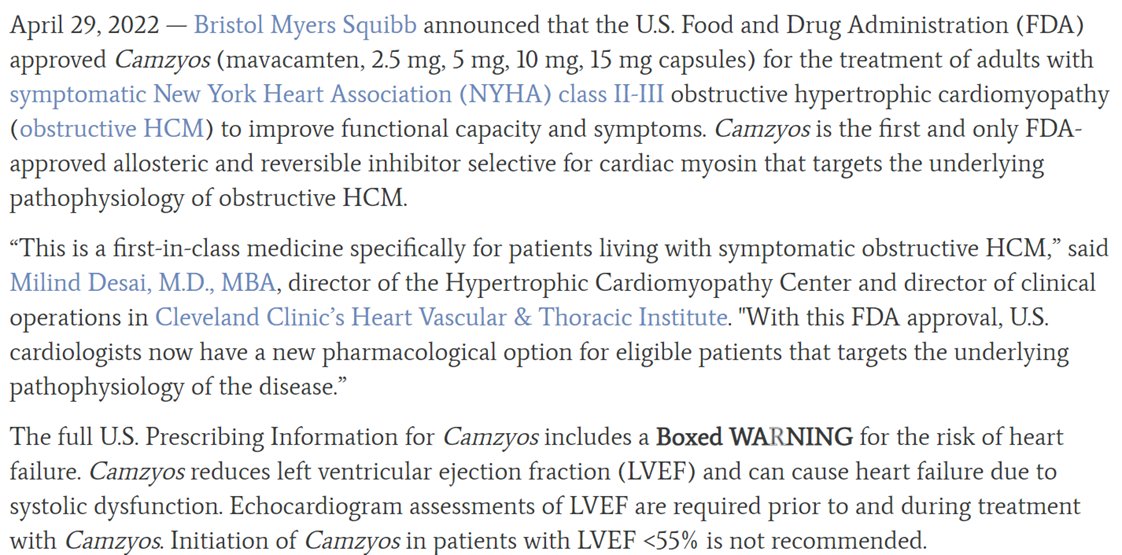
35) In April 2022, based on these data, @US_FDA approved #mavacamtem in #NYHA II-III #HOCM to improve functional capacity & symptoms at a 5mg dose once daily with subsequent doses with titration (max 15mg OD). @EMA_News approval is expected soon.

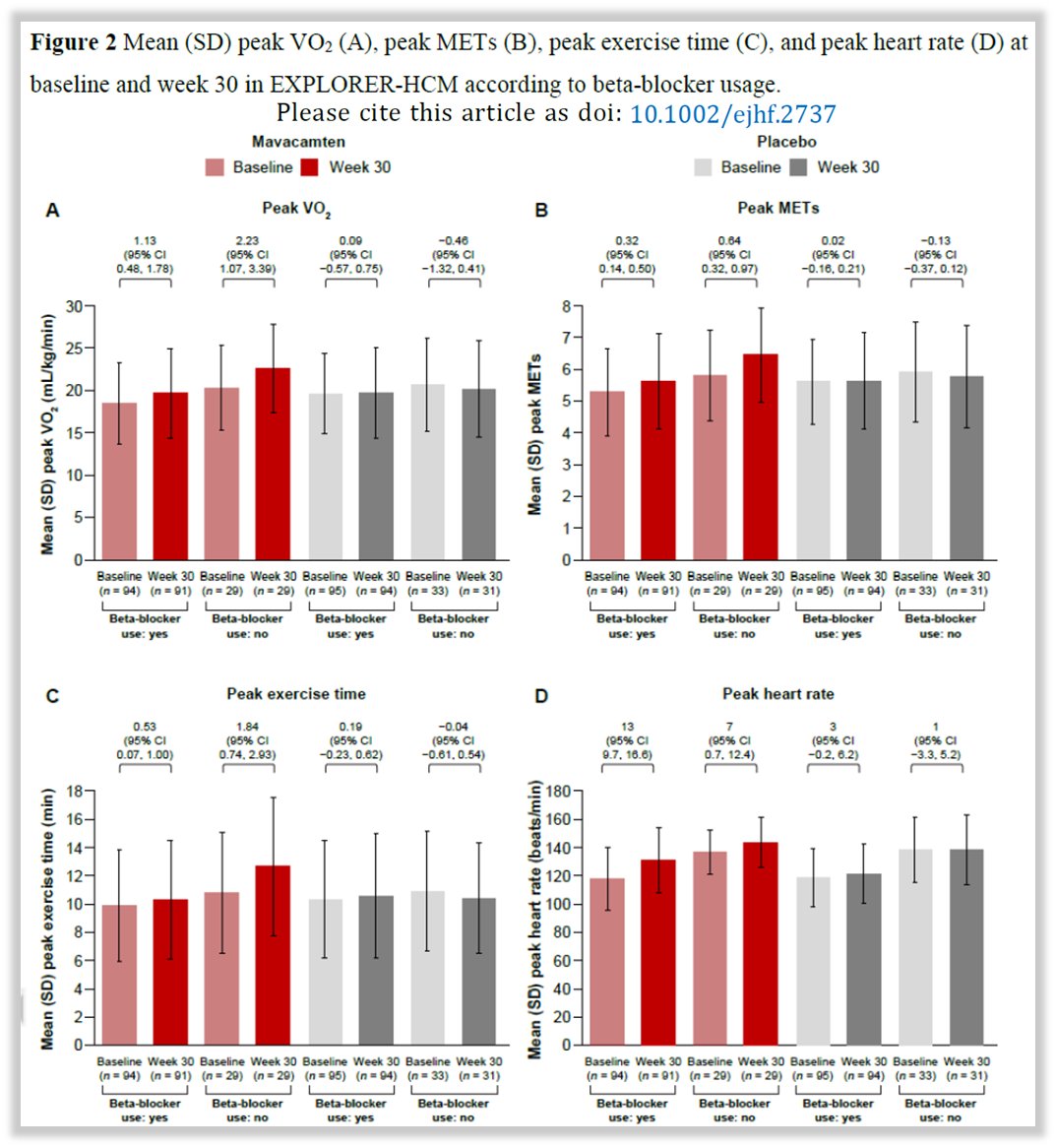
36) A recent analysis of #EXPLORER_HCM showed that the effects of #mavacamtem on #HOCM are independent of the use of beta-blockers. Therefore, they can be used on top of them or as an alternative (for example if BBs are not tolerated).


37) #VALOR_HCM demonstrated even more important result of #mavacamtem in #HOCM, Indeed it significantly reduced the need for #SeptalReductionTherapy. The previous benefits has been confirmed as the safety profile.
👉 shorturl.at/aim05
👉 shorturl.at/aim05
38) Moreover, 10% pts were on #disopyramide & there were no safety signals when the 2 drugs have been coadministered. #VALOR_HCM

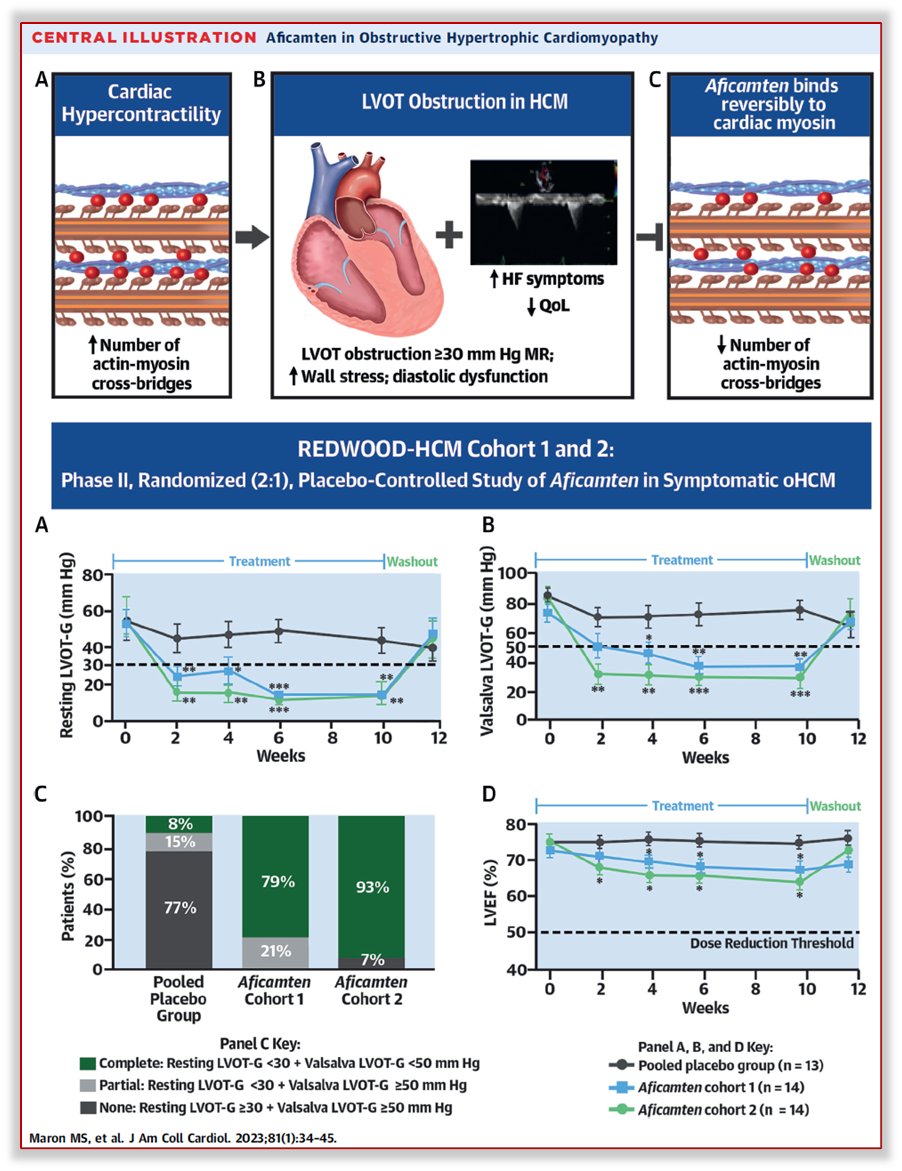
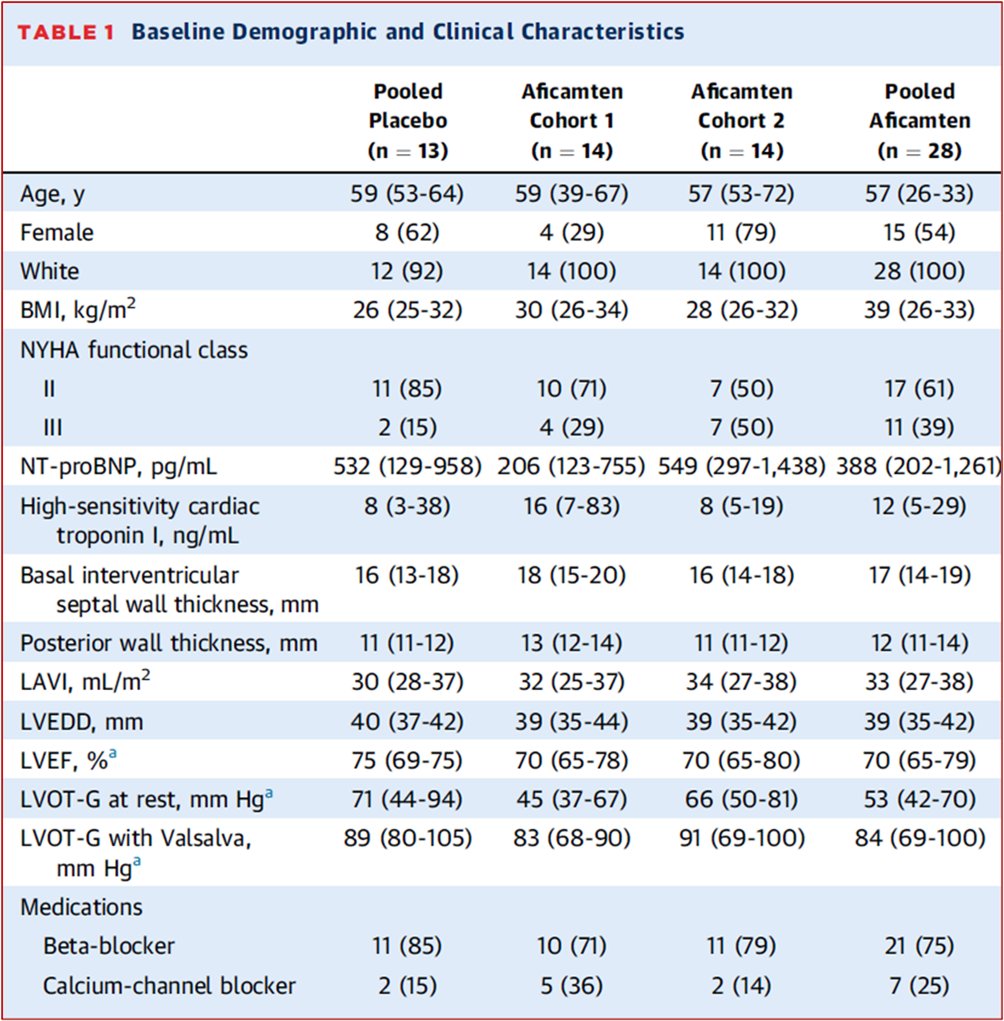
39) Recently another new drug #aficamtem showed significant benefits similar to that of #mavacamtem in a phase 2 RCT #REDWOOD_HCM. However, further confirmation will come from the ongoing Ph 3 RCT #SEQUOIA_HCM, which is enrolling 270 #HOCM pts.


40) So what is the primary #MOA of #mavacamten?
a. inhibits myosin interaction with actin
b. selective and reversible inhibitor of the cardiac myosin ATPase
c. positive inotropy
d. a & b
a. inhibits myosin interaction with actin
b. selective and reversible inhibitor of the cardiac myosin ATPase
c. positive inotropy
d. a & b
41) It's d, a & b. And now you have great insight 👁️into contemporary management of #HCM/#HOCM. Grab your 🆓CE/#CME at cardiometabolic-ce.com/hcm2/ and stay tuned 📺to @cardiomet_ce for more expert-led education. ✔️out @ckd_ce too! I am @GiuseppeGalati_ and I 🙏for joining!
• • •
Missing some Tweet in this thread? You can try to
force a refresh












