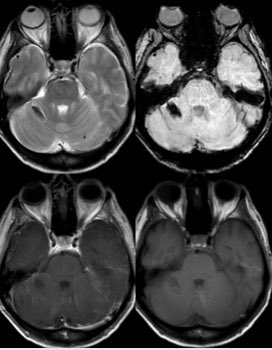
Glioblastoma is the most common variety of astrocytoma
The presence of necrosis is the characteristic feature of glioblastoma
Imaging details in thread #Neurosurgery #neurotwitter #radres #MedTwitter #Neurology @TheASNR
The presence of necrosis is the characteristic feature of glioblastoma
Imaging details in thread #Neurosurgery #neurotwitter #radres #MedTwitter #Neurology @TheASNR




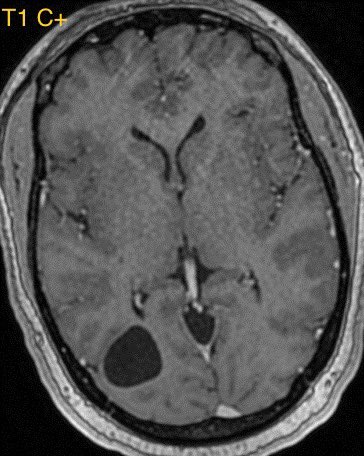
Some correlates for high grade astrocytoma include necrosis, marked mass effect, restricted diffusion (often patchy, eccentric or nodular in glioblastoma), elevated CBV, enhancement, and older age
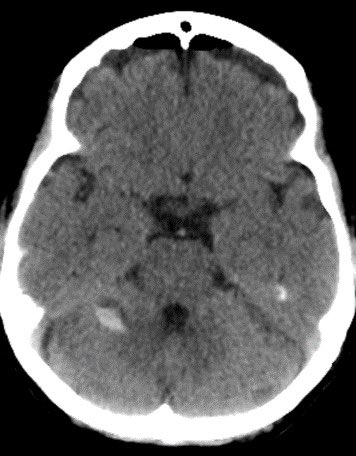
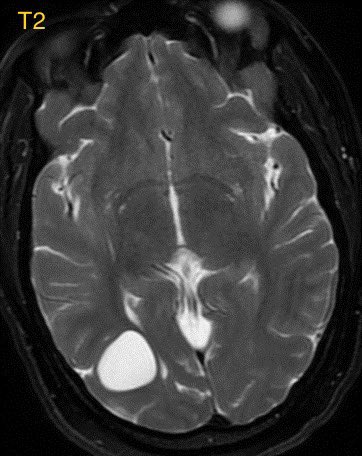
The presence of ependymal spread is another poor prognostic sign (shown below)
The presence of ependymal spread is another poor prognostic sign (shown below)



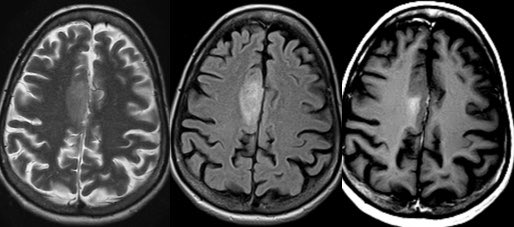
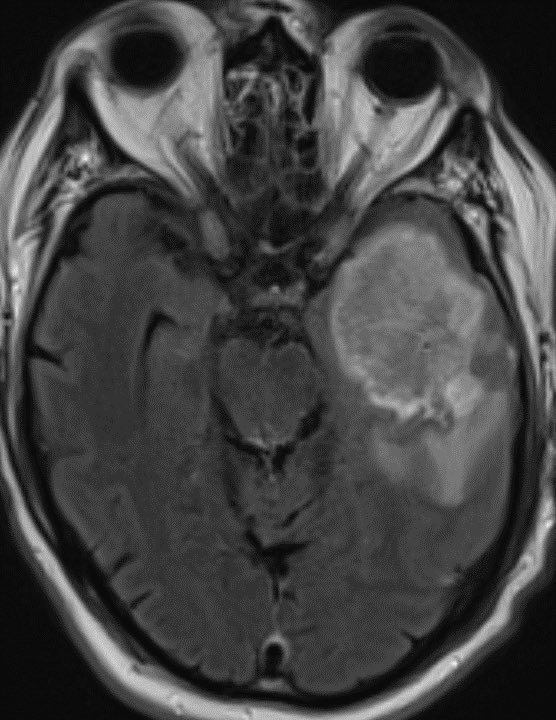
Important learning point: when dealing with glioblastoma, the neoplasm extent is not defined by the area of enhancement but rather by the entire area of T2/FLAIR abnormality. Microscopic infiltrating tumor clearly extends beyond the areas of enhancement. 🧠



When dealing with a known or presumed glioblastoma/high grade astrocytoma, I typically report the area of high T2/FLAIR signal surrounding the necrotic mass as “infiltrating tumor and/or vasogenic edema” knowing that there is a very high probability of microscopic spread

Radiation oncologists treat the entire area of abnormal signal (not just the enhancing portion) with the expectation of infiltrating tumor. Then they typically do a more focused port around the enhancing portion. 🧠
• • •
Missing some Tweet in this thread? You can try to
force a refresh