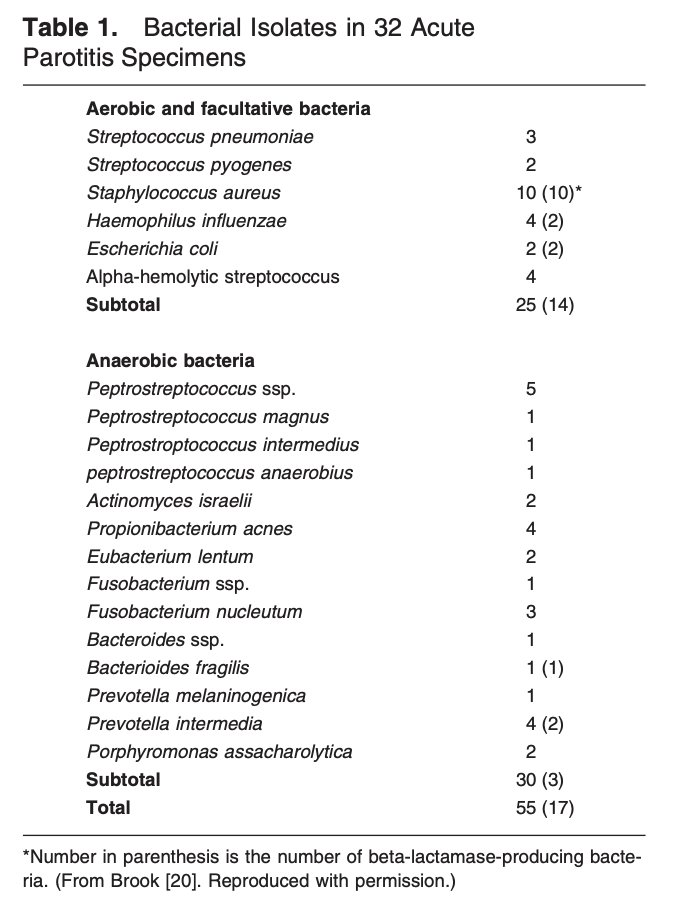
A couple weeks ago I was caring for a patient on the heme-onc service that developed progressive L-sided neck/face swelling over 3-4 hours! He ended up having suppurative parotitis, a diagnosis I have not seen very much in practice. Here are some takeaways #MedTwitter
Risk fxrs for suppurative parotitis include poor PO intake, poor dentition/recent dental work, oropharyngeal malignancies, & intubation (all via impaired stimulation/drainage of salivary ducts). The most common offending bugs are Staph Aureus & anaerobes (pubmed.ncbi.nlm.nih.gov/12544218/)
Apr 12, 2020 • 8 tweets • 4 min read
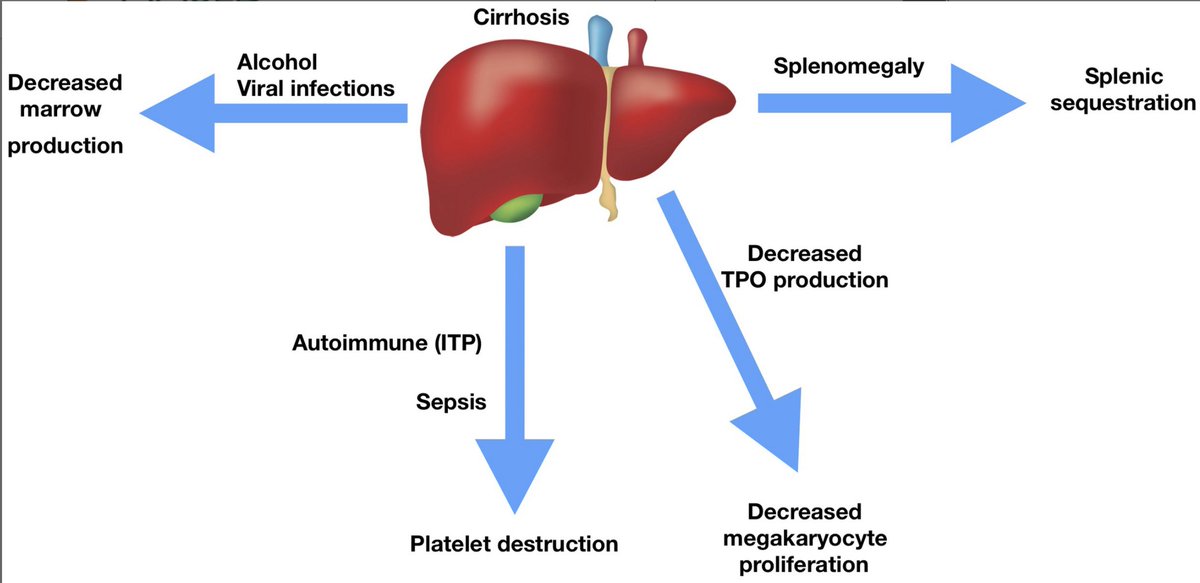
Let's talk about cytopenias in cirrhosis. Many patients with cirrhosis will have at least one cytopenia (sometimes pancytopenia) attributable to their liver disease, let's talk about some of the mechanisms! #medtwitter#hemetwitter
First up, thrombocytopenia! The potential mechanisms are laid out in the image below (aasldpubs.onlinelibrary.wiley.com/doi/full/10.10…):
- decreased thrombopoietin production
- sequestration
- alcohol/viral causes suppressing marrow
- peripheral destruction
Mar 25, 2020 • 5 tweets • 3 min read
An awesome discussion from the @CPSolvers and Drs. Gandhi and Bressman! Here are some thoughts about the pivot point of the case... #SpoilerAlert
Drs. Gotlib and Reiter put an an excellent review discussing myeloid neoplasms with hypereosinophilia (ashpublications.org/blood/article-…), these are some of the salient points for all IM folks to take away
Feb 21, 2020 • 6 tweets • 3 min read
Saw a patient in clinic w/ (likely) refractory ITP and luckily there was an excellent @BloodJournal article by Miltiadous and colleagues published earlier this month! I want to highlight some of the main learning points I took away #medtwitter#hemetwitterashpublications.org/blood/article/…
# 1: Make sure that the patient truly has primary, refractory ITP! If a patient is not responding as expected with primary ITP-directed therapies, it bears consideration to do a more extensive workup looking for alternative diagnoses
Oct 23, 2019 • 4 tweets • 3 min read
Check out my @hdx case from today: a 62-yo man with chest pain! Thanks to @AnandJag1 for the edits. Below you will find some teaching points about this case #SpoilerAlert#Medtwitter
As part of our patient's PMH, he reported facial nerve palsy. Here is a slide with some teaching points about Bell's Palsy including the differential diagnosis to consider (Eviston et al, 2015)
Oct 15, 2019 • 11 tweets • 4 min read
Hi #MedTwitter, let's talk about the workup of polycythemia and making a diagnosis of polycythemia vera (PV) vs. secondary polycythemia! #mpnsm#tweetorial@MedTweetorials
Based on the WHO guidelines, the following values constitute polycythemia:
In men: Hgb >16.5g/dL or Hct > 49%
In women: Hgb > 16 or Hct > 48%
Polycythemia should be confirmed by a subsequent CBC. Below is an image of the ddx of polycythemia (Keohane et al 2013)
Feb 17, 2019 • 11 tweets • 4 min read
#Tweetorial Just finished 4 weeks on the leukemia service at @UCCancerCenter. We saw a number of patients present with a new diagnosis of acute leukemia and hyperleukocytosis, our index of concern for the development of leukostasis was dependent on if they had AML or ALL.
In 1982 Lichtman et al wrote about hyperleukocytic leukemias. The leukocrit (packed WBC volume) was described in AML, ALL, and CLL. Due to the larger mean cell volume of myeloblasts, a higher leukocrit was observed in AML compared to ALL and CLL.