
Here goes it! 🎙
Okay for all those non-oncology experts walking into this situation, let’s take a few steps back 🦶 and give a background on ibrutinib 👩🏫📜
Okay for all those non-oncology experts walking into this situation, let’s take a few steps back 🦶 and give a background on ibrutinib 👩🏫📜
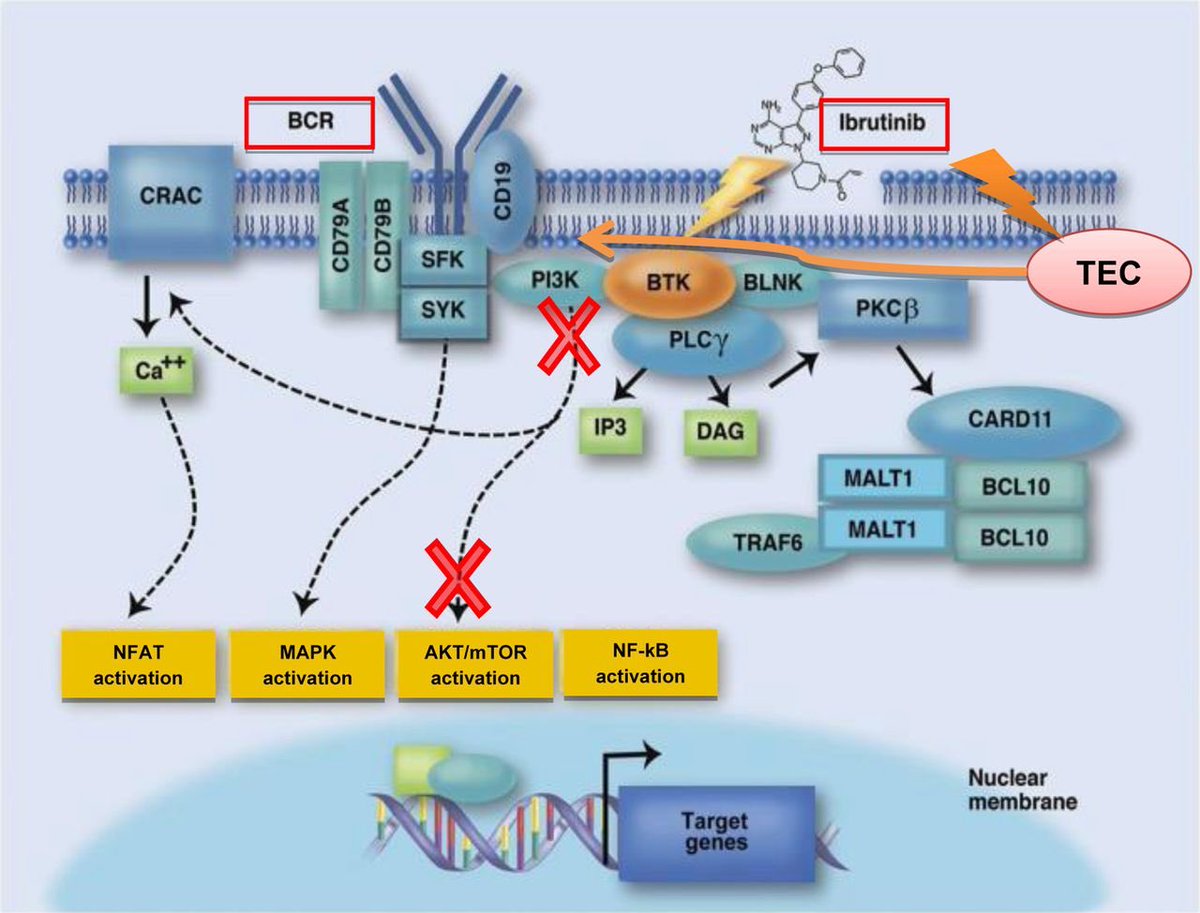
Ibrutinib (Ibruvica®️) is a first in class ORAL 💊 Bruton tyrosine kinase (BTK) inhibitor,
Used for the treatment of a variety of B-cell lymphomas and Waldenstrom macroglobulinemia 🧬
Used for the treatment of a variety of B-cell lymphomas and Waldenstrom macroglobulinemia 🧬
Ibrutinub was a paradigm shift in the management of patients with CLL as initial or relapsed refractory cases
✅improved progression-free survival, ✅overall response rates, and ✅ overall survival
This was compared w/ ofatumumab (AKA rituximabs cousin) & ⚠️ chlorambucil ⚠️
✅improved progression-free survival, ✅overall response rates, and ✅ overall survival
This was compared w/ ofatumumab (AKA rituximabs cousin) & ⚠️ chlorambucil ⚠️
Among many ADEs associated with ibrutinib (diarrhea 🚽 , fatigue 😴 , infections 🦠)cardiovascular are prominent & diverse, ranging from HTN, bleeding, and atrial fibrillation.
In clinical trials the incidence of AF with ibrutinib was ~4-6%
HOWEVER as @PamelaPLN mentioned, studies assessing patients with longer follow up (28 months) the incidence rose as high as 16% 😟
HOWEVER as @PamelaPLN mentioned, studies assessing patients with longer follow up (28 months) the incidence rose as high as 16% 😟
How does ibrutinib cause afib? 🤔
BTK is expressed in ❤️ tissue & ibrutinib has off target effects on other kinases in cardiac tissue that play a role in maintaining sinus rhythm Therefore, it is plausible that ibrutinib ↗️ vulnerability to AF by ⬇️regulation of these pathways
BTK is expressed in ❤️ tissue & ibrutinib has off target effects on other kinases in cardiac tissue that play a role in maintaining sinus rhythm Therefore, it is plausible that ibrutinib ↗️ vulnerability to AF by ⬇️regulation of these pathways
AF in patients on ibrutinib raises unique challenges
Let’s first take a dive into anticoagulation...
Traditional risk scoring tools to assess the need for AC (CHADS2VASC) have NOT been validated in cancer patients
Let’s first take a dive into anticoagulation...
Traditional risk scoring tools to assess the need for AC (CHADS2VASC) have NOT been validated in cancer patients
AND cancer itself is a prothrombotic disease and associated with 2-fold higher risk of thromboembolism and 6-fold increased risk of heart failure 💔
Can I get a #cardioonc consult on this 😅
Can I get a #cardioonc consult on this 😅
healio.com/hematology-onc… however, evolving data suggests we may be able to use the Italian Risk score!
Pts w/cancer are typically thrombocytopenic/anemic
&to make things more complicated
ibrutinib downregulates glycoprotein expression on platelets which ⬇️ adhesion to von willebrand 👉🏻 ↗️ bleeding risk even w/o AC (~up to 44%!) & risk is only further↗️ when AC is required🤯
&to make things more complicated
ibrutinib downregulates glycoprotein expression on platelets which ⬇️ adhesion to von willebrand 👉🏻 ↗️ bleeding risk even w/o AC (~up to 44%!) & risk is only further↗️ when AC is required🤯
HOWEVER ibrutinib is NOT a contraindication to AC, so which agent do we choose?
Ibrutinib: CYP3A4 substrate, P-gp inhibitor
❌Dabigatran (p-gp substrate)
✅rivaroxaban & apixaban
⚠️Warfarin (N/V & ⬇️oral intake can lead to alterations in INR and↗️bleeding: less preferred)
Ibrutinib: CYP3A4 substrate, P-gp inhibitor
❌Dabigatran (p-gp substrate)
✅rivaroxaban & apixaban
⚠️Warfarin (N/V & ⬇️oral intake can lead to alterations in INR and↗️bleeding: less preferred)
Studies have evaluated low dose AC, though the data is scare
Initial ⬇️ dose followed by approved maintenance doses based on tolerability has been suggested
BUT does not account for ↗️ bleeding risks when using full therapeutic doses
jhoponline.com/jhop-issue-arc…
Initial ⬇️ dose followed by approved maintenance doses based on tolerability has been suggested
BUT does not account for ↗️ bleeding risks when using full therapeutic doses
jhoponline.com/jhop-issue-arc…
Now for rate/rhythm control, main concern also stems from drug-drug interactions
1st for rate control:
✅BB preferred
❌Diltiazem & verapamil👉🏻 potent CYP3A4 inhibitors ↗️ ibrutinib toxicity
On the other hand ibrutinib ↗️
❌Digoxin concentrations through 🚫 of p-gp substrate
1st for rate control:
✅BB preferred
❌Diltiazem & verapamil👉🏻 potent CYP3A4 inhibitors ↗️ ibrutinib toxicity
On the other hand ibrutinib ↗️
❌Digoxin concentrations through 🚫 of p-gp substrate
Levels of dig CAN be monitored but only to use if BB are ineffective alone
Pearl: controlling HTN with BB can help ⬇️ risk of AF! Thanks @PharmDickerson ashpublications.org/blood/article-…
Pearl: controlling HTN with BB can help ⬇️ risk of AF! Thanks @PharmDickerson ashpublications.org/blood/article-…
At last, we have amiodarone
Amiodarone is fraught by many DDI with both anticoagulants and nodal blocking agents and based on the above noted info, would increase concentrations of ibrutinib for as long as amio remains in the system (~60 days 😅)
Amiodarone is fraught by many DDI with both anticoagulants and nodal blocking agents and based on the above noted info, would increase concentrations of ibrutinib for as long as amio remains in the system (~60 days 😅)










