
@CTSnetorg Global #COVID19 Grand Rounds starting at 8amPST!
Moderated by Drs. @tomcnguyen @BrianMitzman Chikwe
Featuring Drs. @igeorge1975 @vinodthourani @TomMihaljevicMD et al
Zoom: zoom.us/j/559438750
Hashtag: #CTSNetLive
Live tweet thread to follow below
Moderated by Drs. @tomcnguyen @BrianMitzman Chikwe
Featuring Drs. @igeorge1975 @vinodthourani @TomMihaljevicMD et al
Zoom: zoom.us/j/559438750
Hashtag: #CTSNetLive
Live tweet thread to follow below

/2 The #COVID19 pandemic continues to challenge healthcare. In times of unknown, we need to rely on the collective experience of our #CTSurgery community.
Lets learn together rather than apart #CTSNetLive #TSSMN
Lets learn together rather than apart #CTSNetLive #TSSMN
/3 Make sure to also check out all the fantastic #COVID19 resources compiled by #CTSNetLive @CTSNet ctsnet.org/article/covid-…
/4 CTSNet.org @ctsnetorg is the most comprehensive, heavily trafficked, and reliable online source of information about cardiothoracic surgery available worldwide, and its online community of cardiothoracic surgeons is the largest in the world. #CTSNetLive
/5 #CTSNetLive #COVID19 has overtaken our world by storm and shaping our healthcare systems in ways we have never imagined
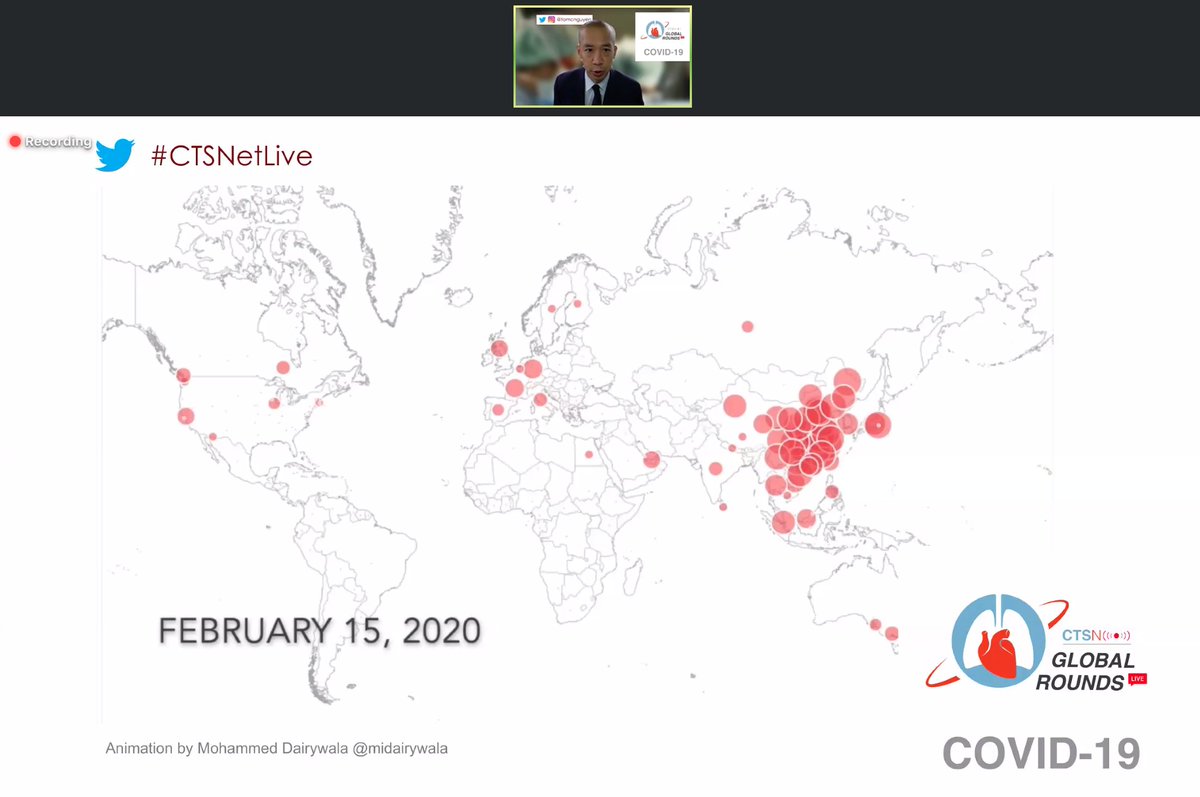
/6 #CTSNetLive Drs. @tomcnguyen @BrianMitzman and Chikwe welcoming us to the Global @ctsnetorg #COVID19 Grand Rounds
/7 #CTSNetLive poll for our audience: What are your greatest challenges
/8 Dr. David Nabarro starting us off with "We're At the Frontline: How Do We Protect Ourselves?" #CTSNetLive
What we know:
- #COVID19 has a capacity to kill depending on healthcare capacity and ability to take care of the patients
- need to identify cases quickly and suppress
What we know:
- #COVID19 has a capacity to kill depending on healthcare capacity and ability to take care of the patients
- need to identify cases quickly and suppress

/9 Dr. David Nabarro: #CTSNetLive on #COVID19
- this is an unseen enemy that is capable of causing enormous problems
Key actions that need to be taken:
- #GetMePPE for your healthcare workers
- early detection, isolation and testing vital given unchecked rapid spread
- this is an unseen enemy that is capable of causing enormous problems
Key actions that need to be taken:
- #GetMePPE for your healthcare workers
- early detection, isolation and testing vital given unchecked rapid spread
/10 Questions for Dr. David Nabarro: #CTSNetLive on #COVID19
Q: Do we need to isolate ourselves from family as healthcare workers? Depends on context, consequences. If high risk exposures or high risk individuals at home -> yes consider isolation at your own risk
Q: Do we need to isolate ourselves from family as healthcare workers? Depends on context, consequences. If high risk exposures or high risk individuals at home -> yes consider isolation at your own risk

/11 Dr. David Nabarro: #CTSNetLive on #COVID19
@WHO actively seeking unique ways to overcome #GetmePPE shortages, ventilator and resource shortages - so calling all physicians to send @WHO links, resources and ideas.
@WHO actively seeking unique ways to overcome #GetmePPE shortages, ventilator and resource shortages - so calling all physicians to send @WHO links, resources and ideas.
/12 Dr. David Nabarro: #CTSNetLive on #COVID19
Q: What will happen with low-and-middle income countries and how to cope with #COVID19? - hope differences in temperature, age of population etc will reduce impact. But ultimately, just don't know. Potential severe consequences
Q: What will happen with low-and-middle income countries and how to cope with #COVID19? - hope differences in temperature, age of population etc will reduce impact. But ultimately, just don't know. Potential severe consequences
/13 Dr. David Nabarro: #CTSNetLive on #COVID19
For isolation - there is potential for people's liberty rights restricted, travel bans and restrictions.
Need to focus on isolation, testing, mitigation, suppression and protection of our frontline workers.
For isolation - there is potential for people's liberty rights restricted, travel bans and restrictions.
Need to focus on isolation, testing, mitigation, suppression and protection of our frontline workers.
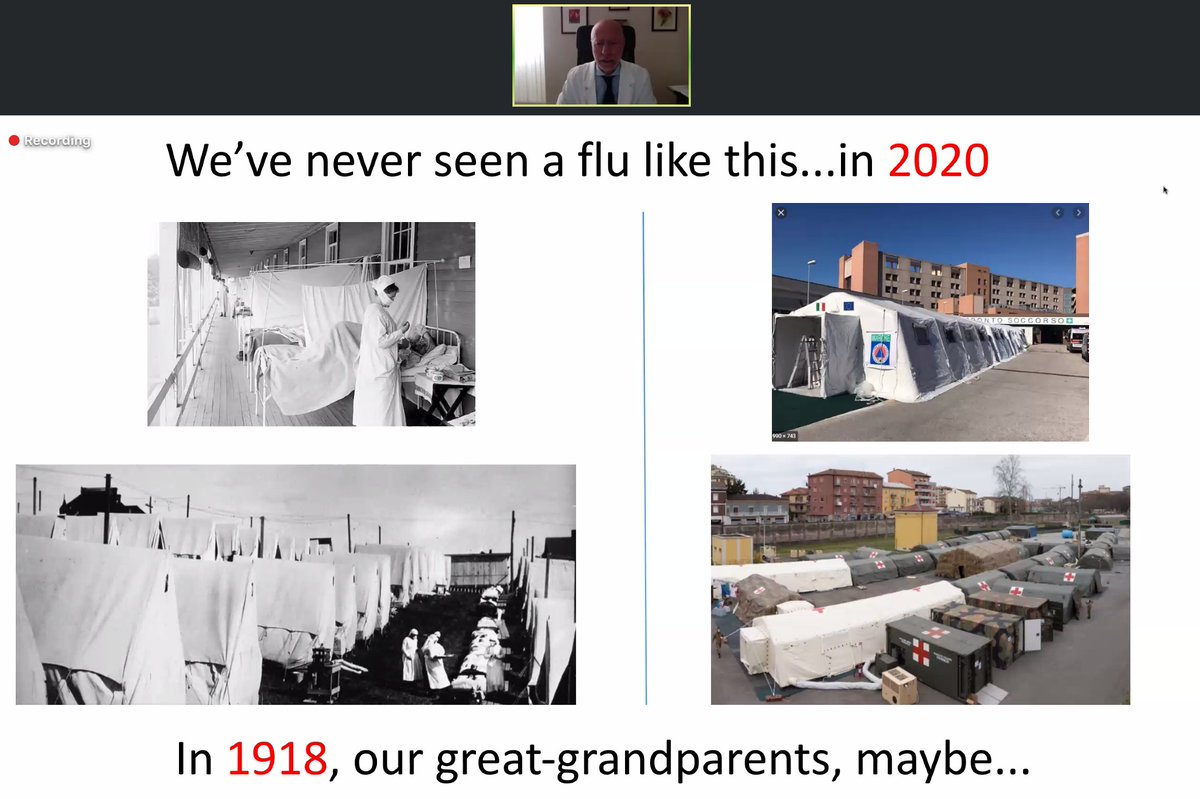
/14 Dr. Marcello Tavio on #CTSNetLive on #COVID19: "
COVID-19 - We're all going to get it, if we don't have it already"
COVID-19 - We're all going to get it, if we don't have it already"

/15 Dr. Marcello Tavio on #CTSNetLive on #COVID19:
#COVID19 is serious and attention needs to be paid to this disease.
#COVID19 is serious and attention needs to be paid to this disease.
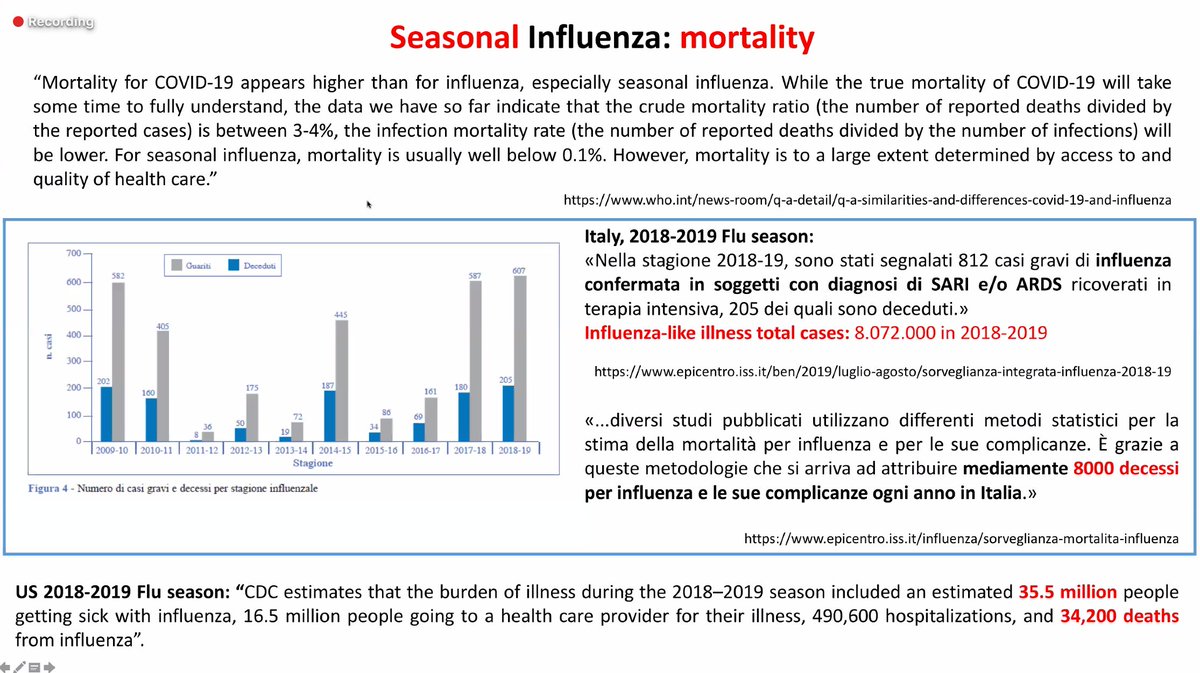
/16 Dr. Marcello Tavio on #CTSNetLive on #COVID19:
#COVID19 mortality is higher than influenza and infectivity is high.
#COVID19 mortality is higher than influenza and infectivity is high.


/18 Dr. Marcello Tavio on #CTSNetLive on #COVID19
Recommendations for the rest of the world, drawing from the Italy experience:
- Testing and protecting your healthcare workers are key
Recommendations for the rest of the world, drawing from the Italy experience:
- Testing and protecting your healthcare workers are key
/19 Dr. Marcello Tavio on #CTSNetLive on #COVID19
Q: If a healthcare worker has an exposure to #COVID19 patient without PPE, what should they do at home? - they should wear PPE
Q: Should all healthcare workers be screened given risk of asymptomatic exposure? -only if symptoms
Q: If a healthcare worker has an exposure to #COVID19 patient without PPE, what should they do at home? - they should wear PPE
Q: Should all healthcare workers be screened given risk of asymptomatic exposure? -only if symptoms
/20 Dr. Marcello Tavio on #CTSNetLive on #COVID19
Q: What is the sensitivity and specificity of current test? 90% sensitive, high specificity. If high suspicion - consider testing twice or treating the patient as #COVID19 positive despite a negative test if symptoamtic
Q: What is the sensitivity and specificity of current test? 90% sensitive, high specificity. If high suspicion - consider testing twice or treating the patient as #COVID19 positive despite a negative test if symptoamtic
/21 #CTSNetLive on #COVID19 with Dr. Isaac George "
I'm a cardiac surgeon and have COVID-19: Now what?"
@igeorge1975 - thank you so much for sharing your personal experience!
I'm a cardiac surgeon and have COVID-19: Now what?"
@igeorge1975 - thank you so much for sharing your personal experience!

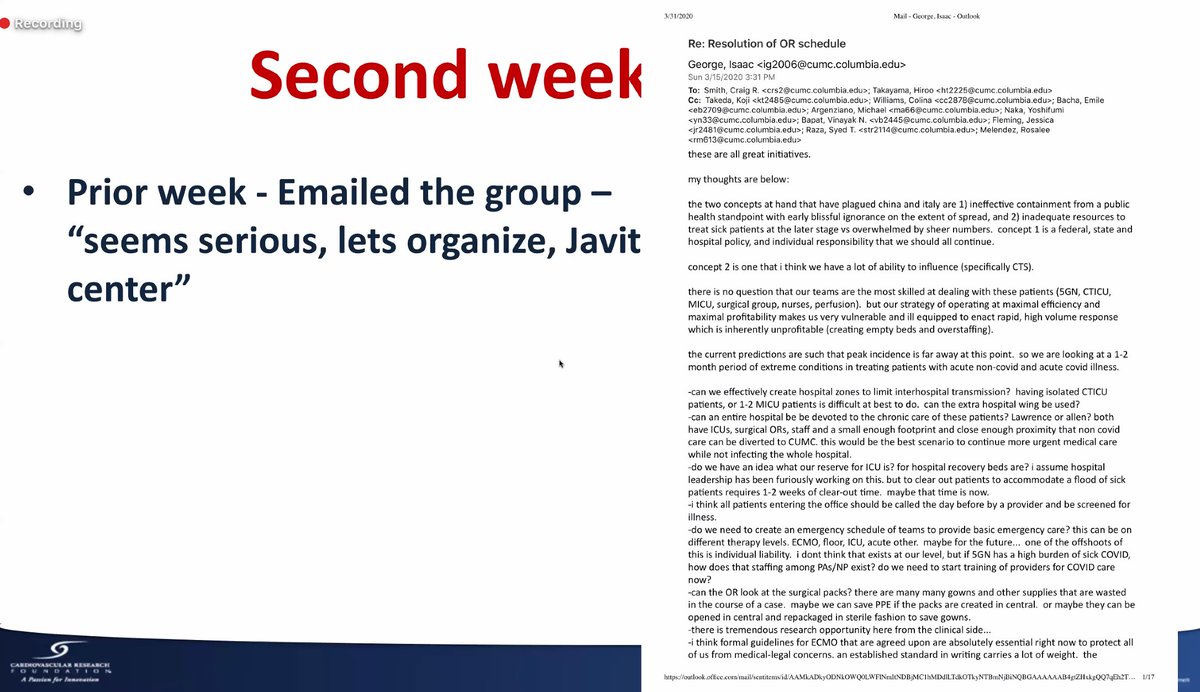
/22 Dr. @igeorge1975 on #CTSNetLive #COVID19
Their hospital-level approach to preparing for #COVID19
Their hospital-level approach to preparing for #COVID19
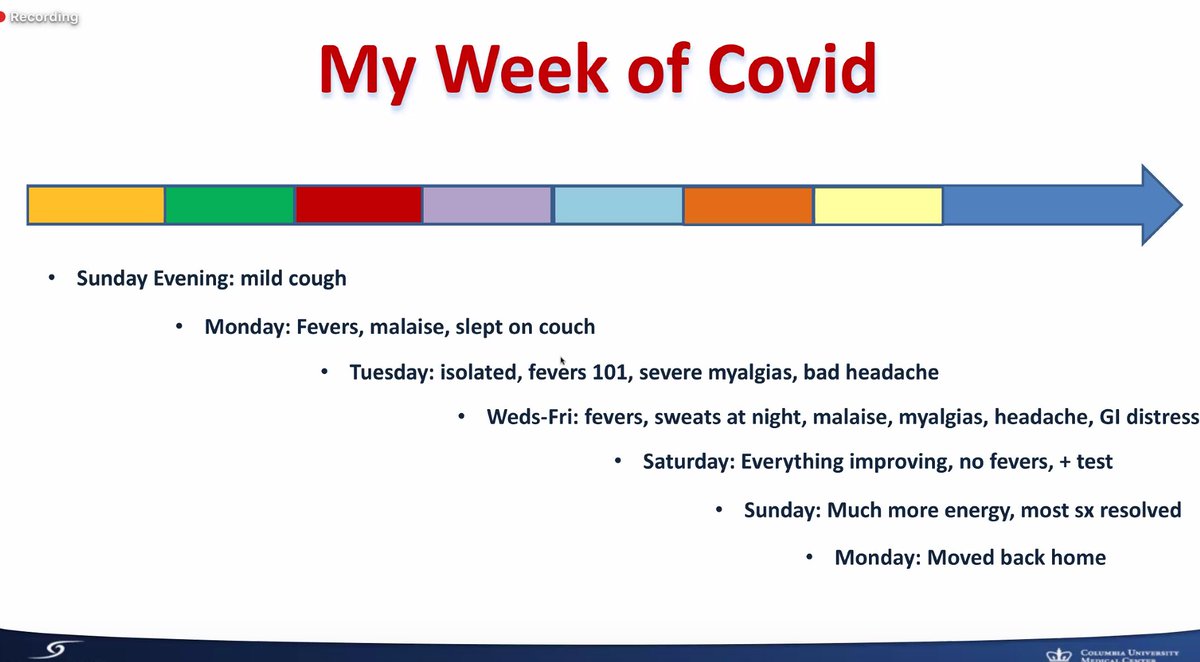
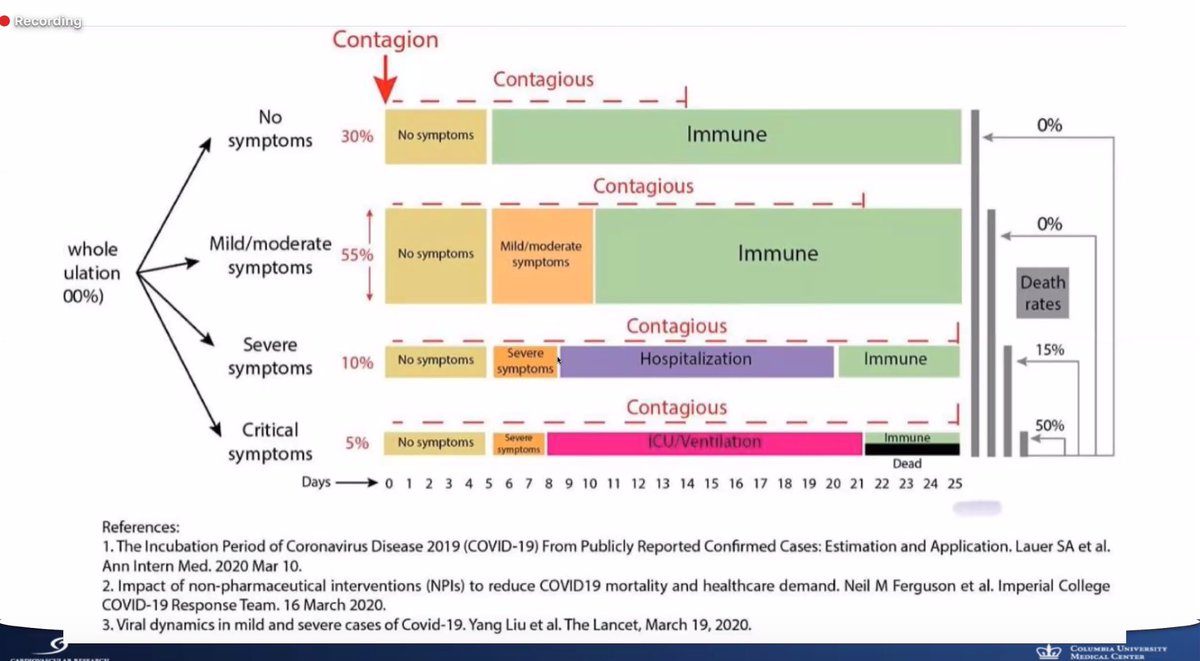
/23 Dr. @igeorge1975 on #CTSNetLive on own experience with #COVID19
Timeline for symptoms with #COVID19 - key takeaway, very constitutional symptoms. Self-isolated from family when symptomatic. Wore PPE at home to protect family.
Timeline for symptoms with #COVID19 - key takeaway, very constitutional symptoms. Self-isolated from family when symptomatic. Wore PPE at home to protect family.
/24 Dr. @igeorge1975 on #CTSNetLive on own experience with #COVID19
When do we go back to work? @CDCgov recommends 7 days since onset of symptoms or when afebrile for 72 hours (whichever is later).
When do we go back to work? @CDCgov recommends 7 days since onset of symptoms or when afebrile for 72 hours (whichever is later).
/25 Dr. @igeorge1975 on #CTSNetLive on own experience with #COVID19
Key takeaways:
- your risk of #COVID19 transmission can be from the last people you expect (those who are asymptomatic)
Key takeaways:
- your risk of #COVID19 transmission can be from the last people you expect (those who are asymptomatic)
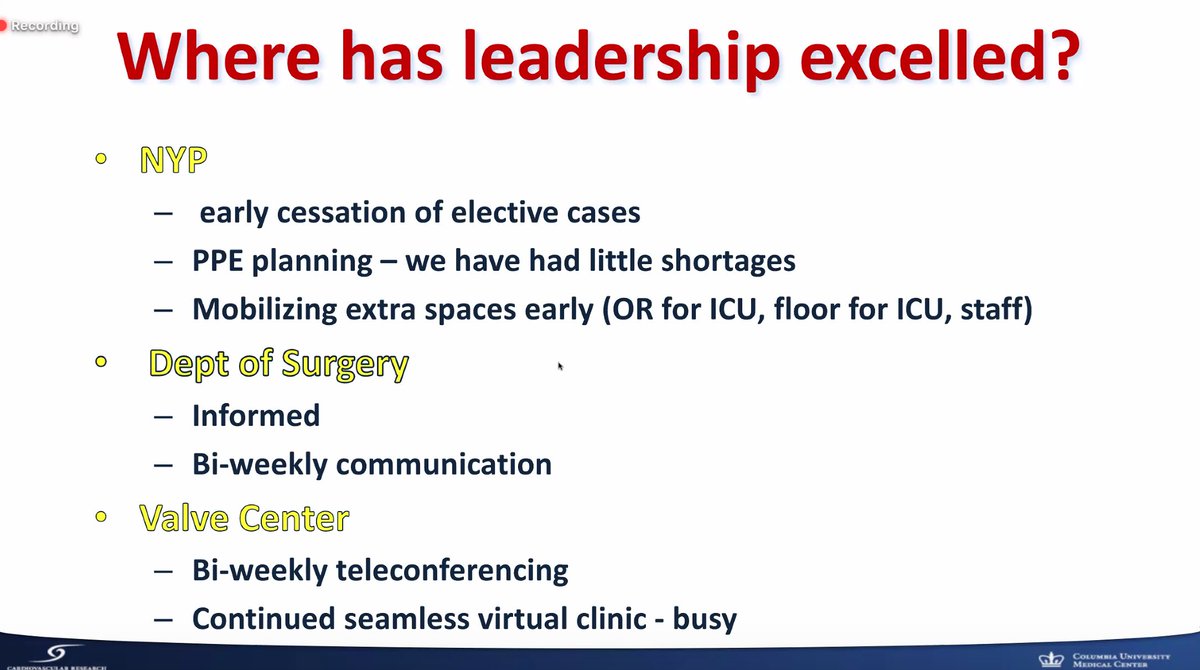
/26 Dr. @igeorge1975 - what can the world learn from the New York #COVID19 experience #CTSNetLive
Key takeaways:
- stop elective cases to conserve PPE, resources and protect healthcare workers
- excellent communication
- utilize telecommunication technologies
Key takeaways:
- stop elective cases to conserve PPE, resources and protect healthcare workers
- excellent communication
- utilize telecommunication technologies
/27 Dr. @igeorge1975 - on New York #COVID19 experience #CTSNetLive
What can be done better?
- mask protocol escalation (no mask -> surgical mask -> N95)
- ambiguous recommendations
- what isolation rooms should be
- testing for healthcare workers
What can be done better?
- mask protocol escalation (no mask -> surgical mask -> N95)
- ambiguous recommendations
- what isolation rooms should be
- testing for healthcare workers

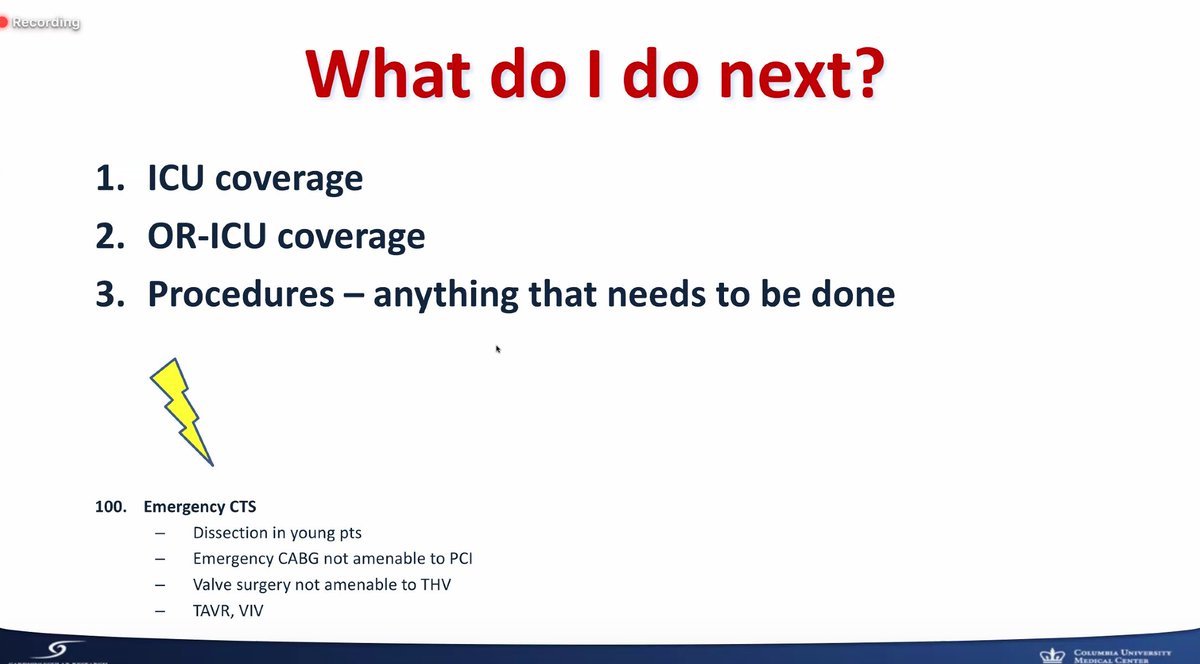
/29 Where Dr. @igeorge1975 goes from here? #CTSNetLive #COVID19 - help out wherever he can + any emergency #CTSurgery
/30 Dr. @igeorge1975 on #CTSNetLive #COVID19:
Re-prioritize what is important in your life
We are all in this together and we will get through this
#BetterTogether
Re-prioritize what is important in your life
We are all in this together and we will get through this
#BetterTogether
/31 Dr. @igeorge1975 on #CTSNetLive #COVID19
Q: Have you been re-tested to be negative prior to returning to work? I have not been re-tested. Serum testing needs to be 14 days out of the infection which would be the next step. (second confirmatory testing)
Q: Have you been re-tested to be negative prior to returning to work? I have not been re-tested. Serum testing needs to be 14 days out of the infection which would be the next step. (second confirmatory testing)
/32 Dr. @igeorge1975 on #CTSNetLive #COVID19
Q: Do you feel empowered with potential immunity against #COVID19? - We do not currently know whether there is immunity and only time will tell.
Q: Do you feel empowered with potential immunity against #COVID19? - We do not currently know whether there is immunity and only time will tell.
/33 Dr. Gino Gerosa on #CTSNetLive #COVID19 on the following topic:
"Hello world, what could we have done differently?"
"Hello world, what could we have done differently?"

/34 Dr. Gino Gerosa on #CTSNetLive #COVID19 sharing his personal experience - had exposure, unprotected, tested and became #COVID19 positive.
Symptoms included high fever and coughing. Stayed home. Need at least 2 negative swabs prior to returning to work at his institution
Symptoms included high fever and coughing. Stayed home. Need at least 2 negative swabs prior to returning to work at his institution
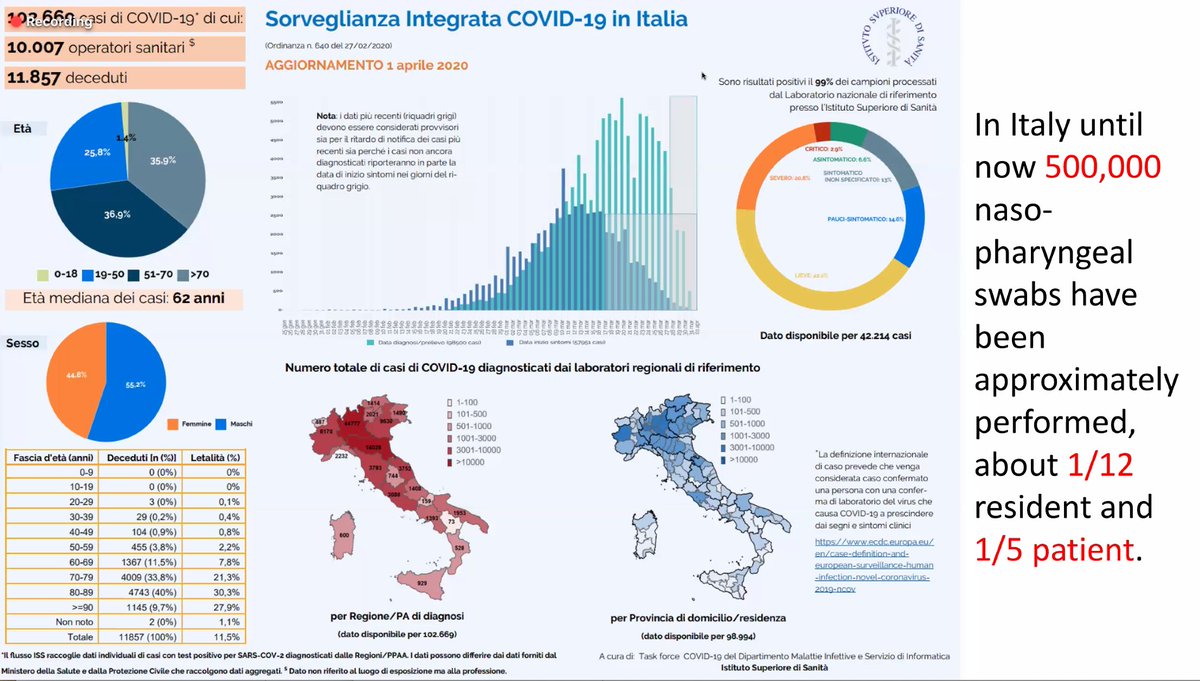
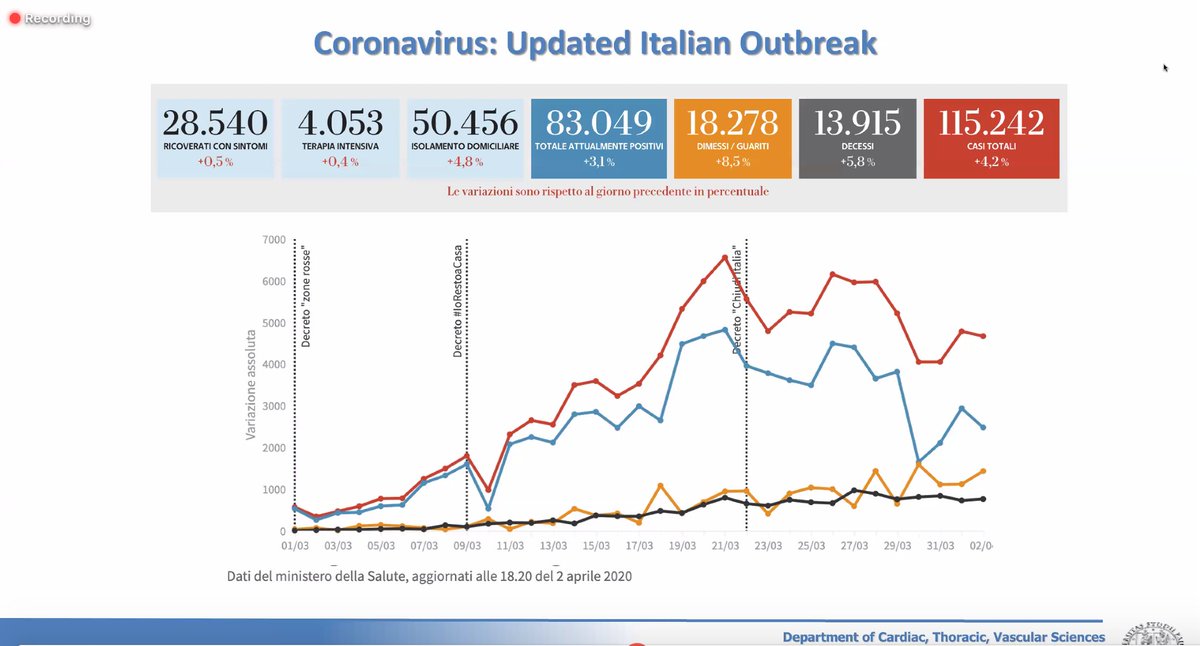
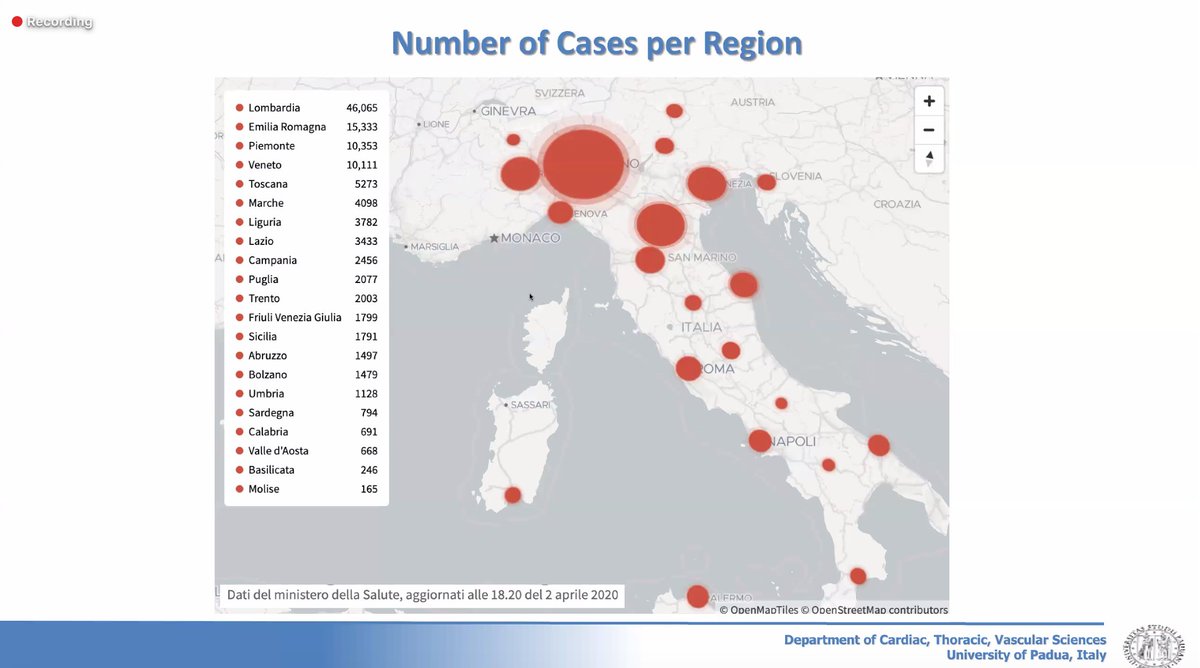
/35 Dr. Gino Gerosa on #CTSNetLive #COVID19
Italy has truly been on the forefront of the pandemic.
What we learned:
- testing key to combat #COVID19 -> quarantine the infected
- #GetMePPE vital to protect healthcare workers -> so far 80 doctors have died
Italy has truly been on the forefront of the pandemic.
What we learned:
- testing key to combat #COVID19 -> quarantine the infected
- #GetMePPE vital to protect healthcare workers -> so far 80 doctors have died
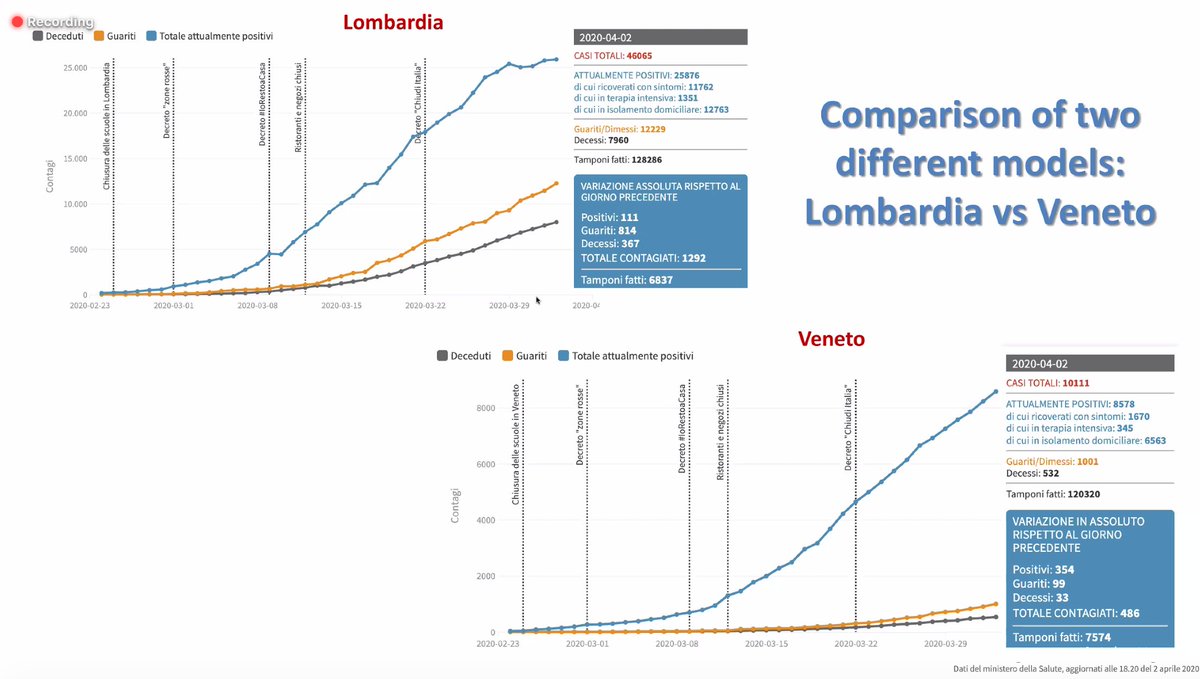
/36 Dr. Gino Gerosa on #CTSNetLive #COVID19
Lessons from the Italy experience:
- have COVID dedicated hospital
- close follow-up of patients as outpatients to keep them out of hospital
- isolate dead patients serum antibodies for testing and determine disease prevalence
Lessons from the Italy experience:
- have COVID dedicated hospital
- close follow-up of patients as outpatients to keep them out of hospital
- isolate dead patients serum antibodies for testing and determine disease prevalence
/37 Dr. Gino Gerosa on #CTSNetLive #COVID19
Q: Why did Italy become the epicenter for #COVID19? Did not isolate and test those with exposures. This likely led to lots of community transmission with the lack of social distancing and quarantine.
Q: Why did Italy become the epicenter for #COVID19? Did not isolate and test those with exposures. This likely led to lots of community transmission with the lack of social distancing and quarantine.
/38 Dr. Gino Gerosa on #CTSNetLive #COVID19
Q: What is the morale now in Italy? Social distancing very seriously enforced in Italy with most non-essential services closed.
Q: What advice do you have for the rest of the world? Social distancing and testing key.
Q: What is the morale now in Italy? Social distancing very seriously enforced in Italy with most non-essential services closed.
Q: What advice do you have for the rest of the world? Social distancing and testing key.

/41 #CTSNetLive #COVID19
For heart transplants, less donors due to:
- Social distancing (less accidents)
- #COVID19 patients taking up ICU beds and hospital resources
- need to test donors and recipients to be #COVID19 negative prior to transplantation
For heart transplants, less donors due to:
- Social distancing (less accidents)
- #COVID19 patients taking up ICU beds and hospital resources
- need to test donors and recipients to be #COVID19 negative prior to transplantation
/42 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19:
"When (if) the COVID dust settles, what will be the long-term impact to economies and health care institutions?"
"When (if) the COVID dust settles, what will be the long-term impact to economies and health care institutions?"
/43 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
- tripled hospital and ICU capacity in anticipation for the wave
- social distancing in place (one of the first states in the US)
- tripled hospital and ICU capacity in anticipation for the wave
- social distancing in place (one of the first states in the US)
/44 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
What to expect after #COVID19 pandemic:
- increased utilization of telemedicine
- increased ambulatory care
- hospital care reserved only for those who truly need it
- care for healthcare workers
What to expect after #COVID19 pandemic:
- increased utilization of telemedicine
- increased ambulatory care
- hospital care reserved only for those who truly need it
- care for healthcare workers
/45 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
The following would be emphasised post #COVID19
- Increased appreciation for healthcare workers, social life, leadership, integrated healthcare systems and what truly matters
- shared resources / care
The following would be emphasised post #COVID19
- Increased appreciation for healthcare workers, social life, leadership, integrated healthcare systems and what truly matters
- shared resources / care
/46 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
What to see after #COVID19
- More integrated healthcare systems
- Centralization of care and resources
- Decline in small isolated healthcare systems
- We are #bettertogether
- Larger role for central payer
What to see after #COVID19
- More integrated healthcare systems
- Centralization of care and resources
- Decline in small isolated healthcare systems
- We are #bettertogether
- Larger role for central payer
/47 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
What to see after #COVID19
- Lifelong partnership between patients and providers
- Meet needs of patients with digital technology
- Emphasis of data-driven care and preparation for disasters
What to see after #COVID19
- Lifelong partnership between patients and providers
- Meet needs of patients with digital technology
- Emphasis of data-driven care and preparation for disasters
/48 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
How to live with the pandemic?
- Help those in need
- Expect serious economic downturn
- Beware of deferred care
- Need to consider sustainability
How to live with the pandemic?
- Help those in need
- Expect serious economic downturn
- Beware of deferred care
- Need to consider sustainability
/49 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
Takeaways:
- Scale up digital technology
- Seek partnerships
- Predictive modelling+artificial intelligence to tailor approach to pandemic
- Know your data
- Work with worse case scenario -> Prepare for this
Takeaways:
- Scale up digital technology
- Seek partnerships
- Predictive modelling+artificial intelligence to tailor approach to pandemic
- Know your data
- Work with worse case scenario -> Prepare for this
/50 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
Takeaways:
- Educate+reassign healthcare providers where they are needed
- Support and protect your people #GetMePPE
- Communication is key to empower your team and the public
- Complete transparency
- Listen
Takeaways:
- Educate+reassign healthcare providers where they are needed
- Support and protect your people #GetMePPE
- Communication is key to empower your team and the public
- Complete transparency
- Listen
/51 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
Q: What will be the new norm with PPE? With greater availability of testing, we can taillor our response. But at this time, need PPE. Some will be here to stay as the new norm.
Q: What will be the new norm with PPE? With greater availability of testing, we can taillor our response. But at this time, need PPE. Some will be here to stay as the new norm.
/52 Dr. @TomMihaljevicMD from @CleClinicMD on #CTSNetLive #COVID19
Q: What has been the role of advanced care providers in #COVID19? Ensure people are educated and well-supported in their new / altered roles with oversight by a multidisciplinary team.
Q: What has been the role of advanced care providers in #COVID19? Ensure people are educated and well-supported in their new / altered roles with oversight by a multidisciplinary team.
/53 Dr. @TomMihaljevicMD on #CTSNetLive #COVID19
Q: What is the financial sustainability of healthcare systems with #COVID19? We will always have losses because we have suspended our non-essential clinical activity along with delayed reimbursement with fixed HCW costs
Q: What is the financial sustainability of healthcare systems with #COVID19? We will always have losses because we have suspended our non-essential clinical activity along with delayed reimbursement with fixed HCW costs
/54 Dr. @TomMihaljevicMD on #CTSNetLive #COVID19:
"Stay calm and carry on" ... this pandemic will accelerate into some sort of good in medicine.
"Stay calm and carry on" ... this pandemic will accelerate into some sort of good in medicine.

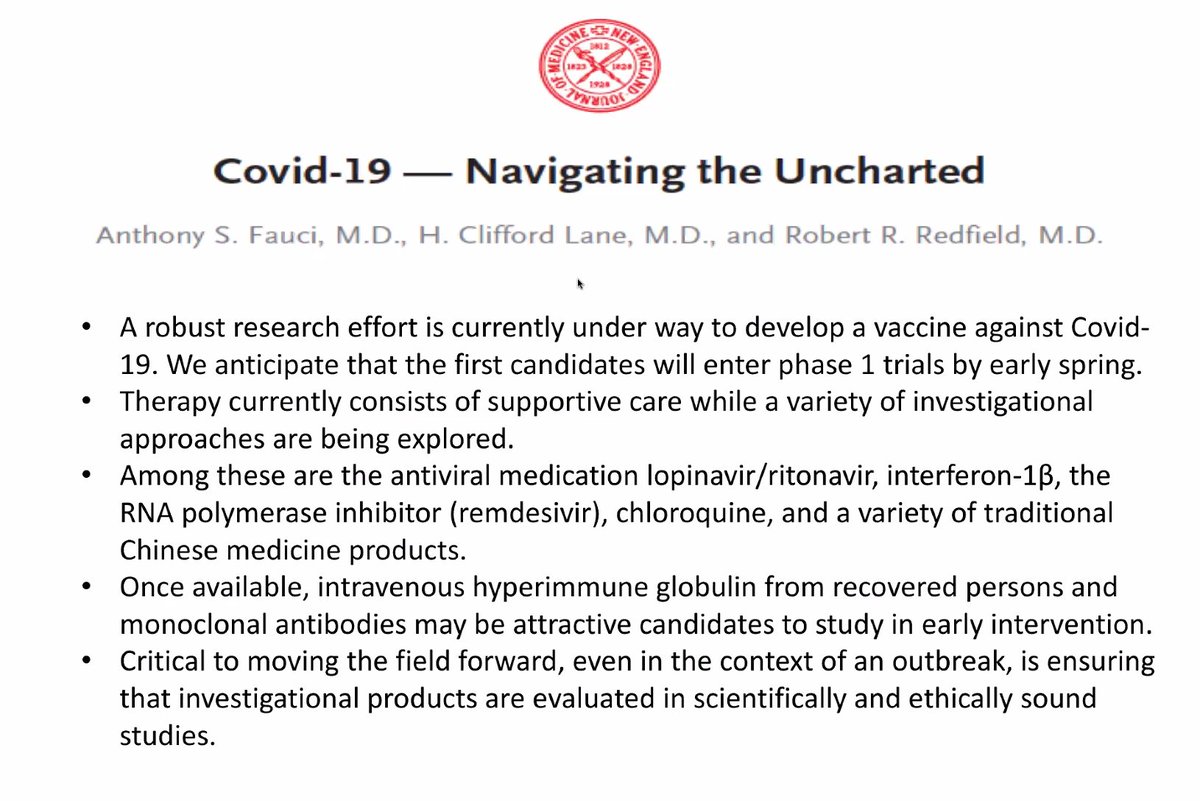
/56 Dr. @VinodThourani on #CTSNetLive #COVID19:
We are at a place where we do not have all the answers for, unlike #CTSurgery
- Critical to evaluate therapies in a scientific evidence-based manner
- Remain grounded -> patient safety first
- Scientifically and ethically sound
We are at a place where we do not have all the answers for, unlike #CTSurgery
- Critical to evaluate therapies in a scientific evidence-based manner
- Remain grounded -> patient safety first
- Scientifically and ethically sound
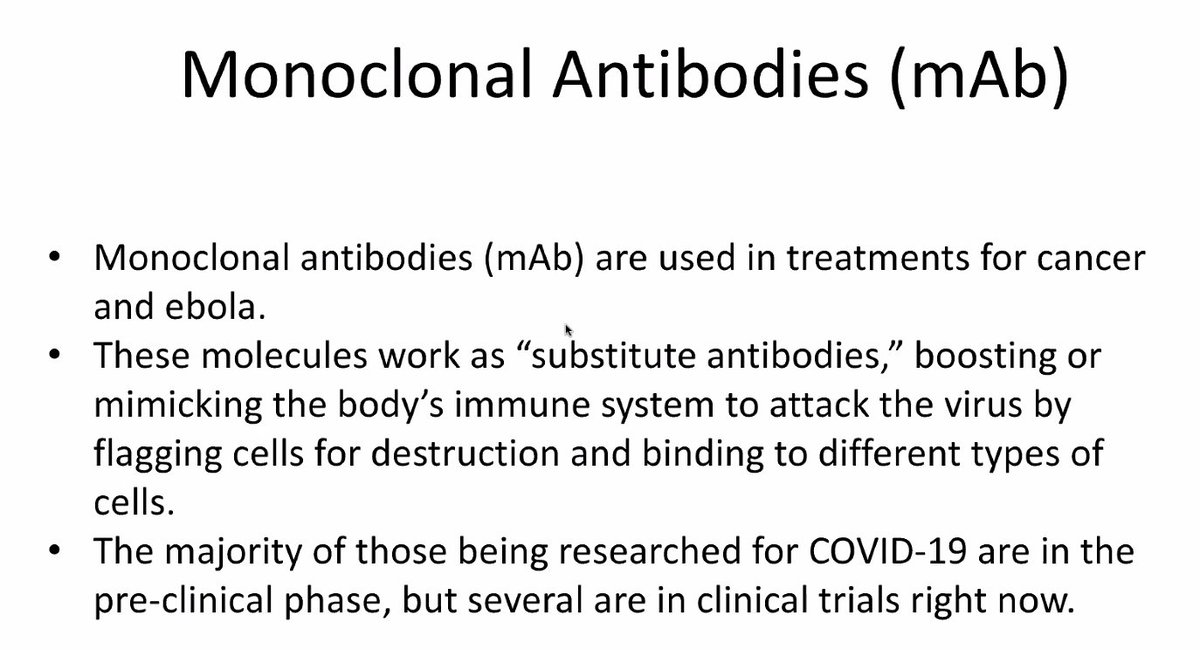
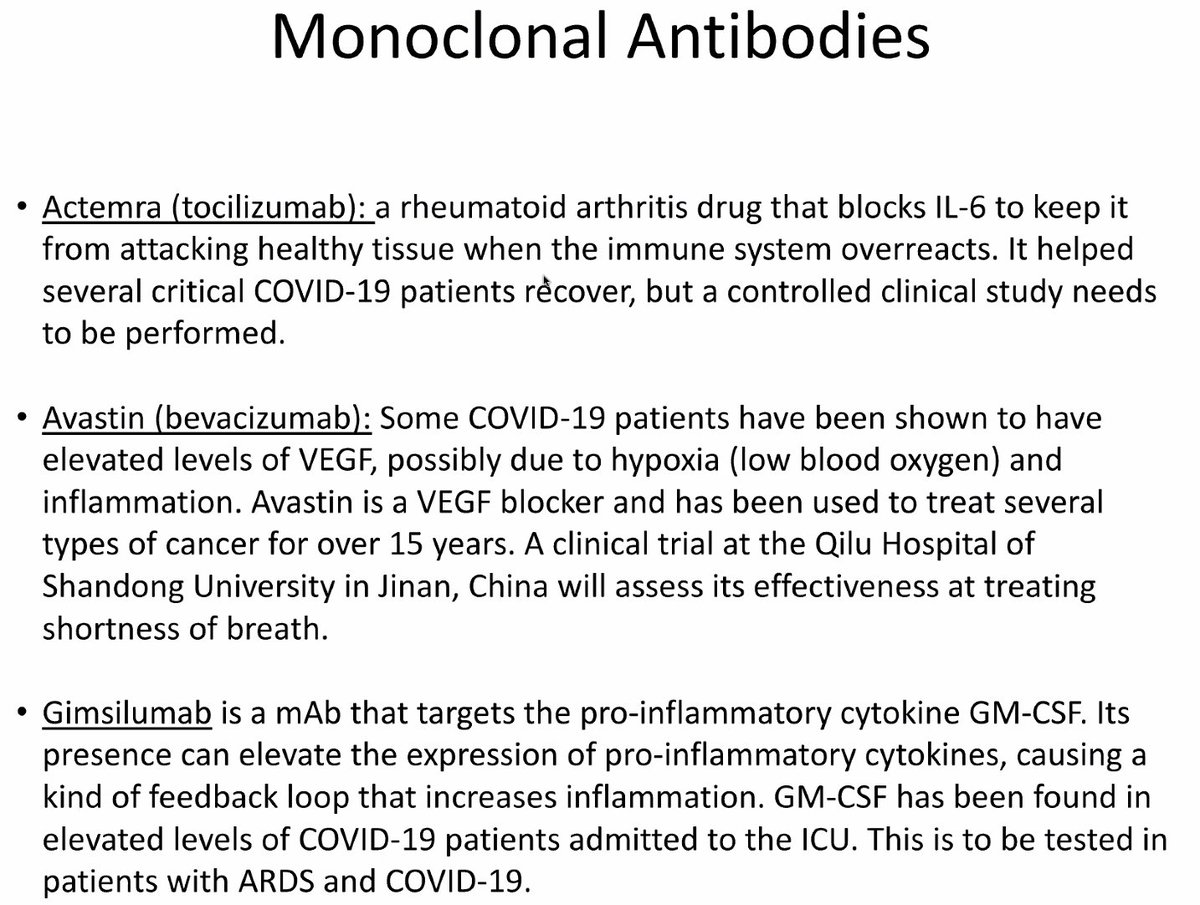
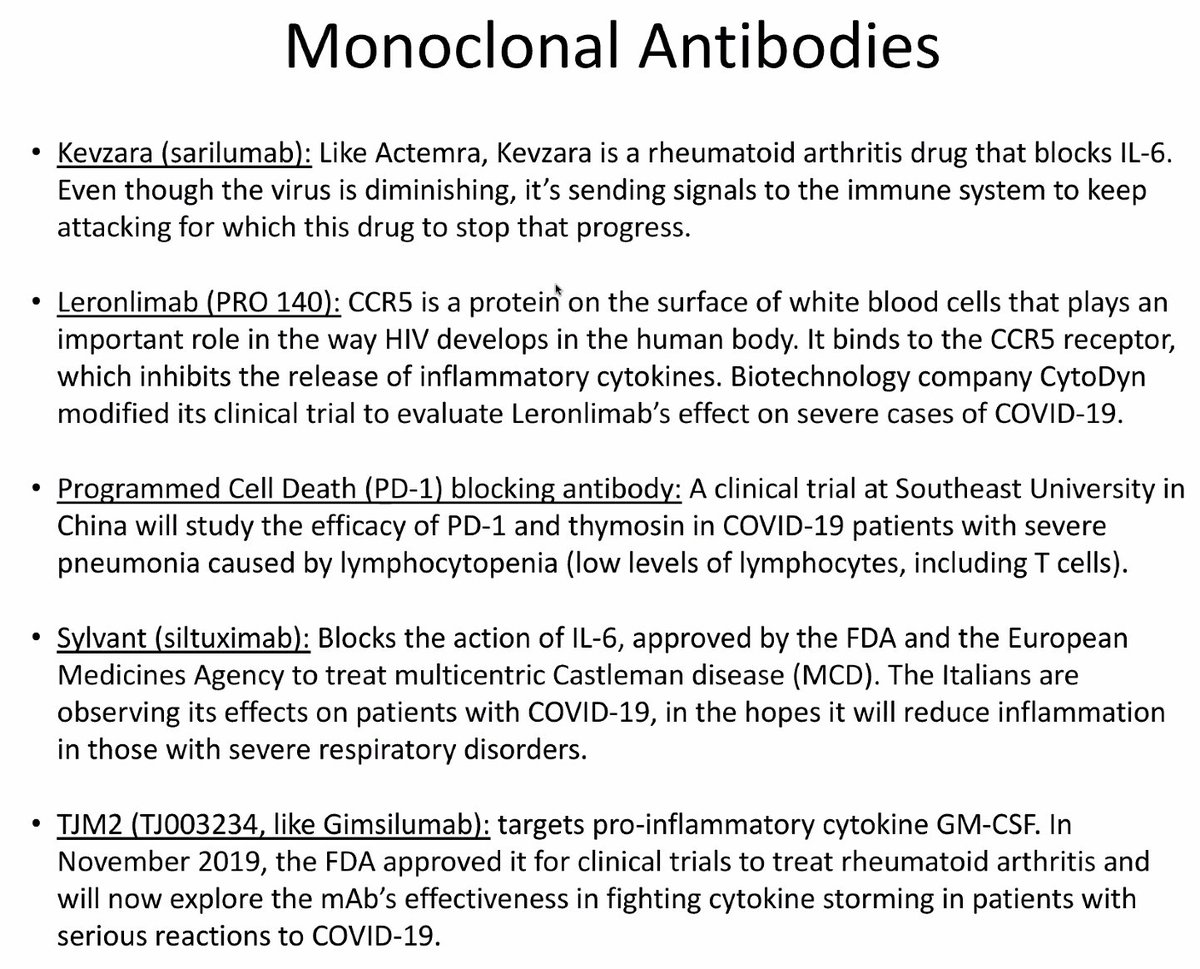
/57 Dr. @VinodThourani on #CTSNetLive #COVID19:
Monoclonal antibodies coming down the pipeline as a potential therapy for #COVID19
Monoclonal antibodies coming down the pipeline as a potential therapy for #COVID19
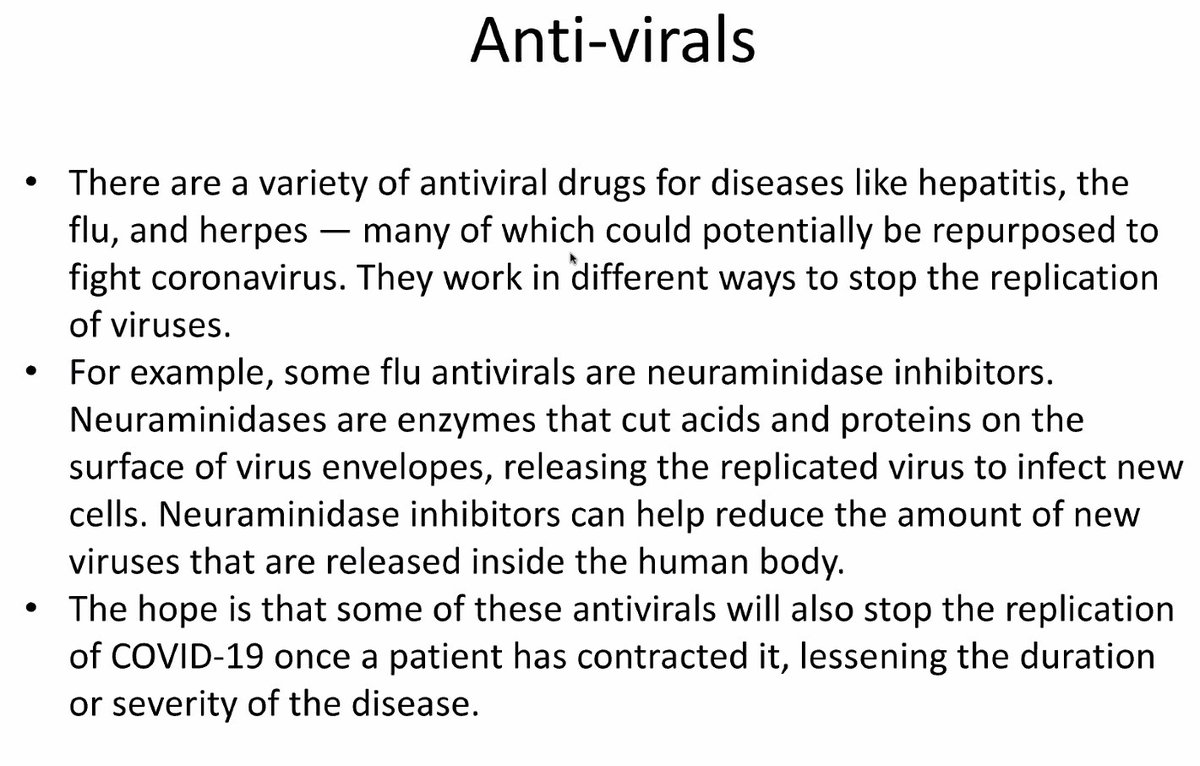
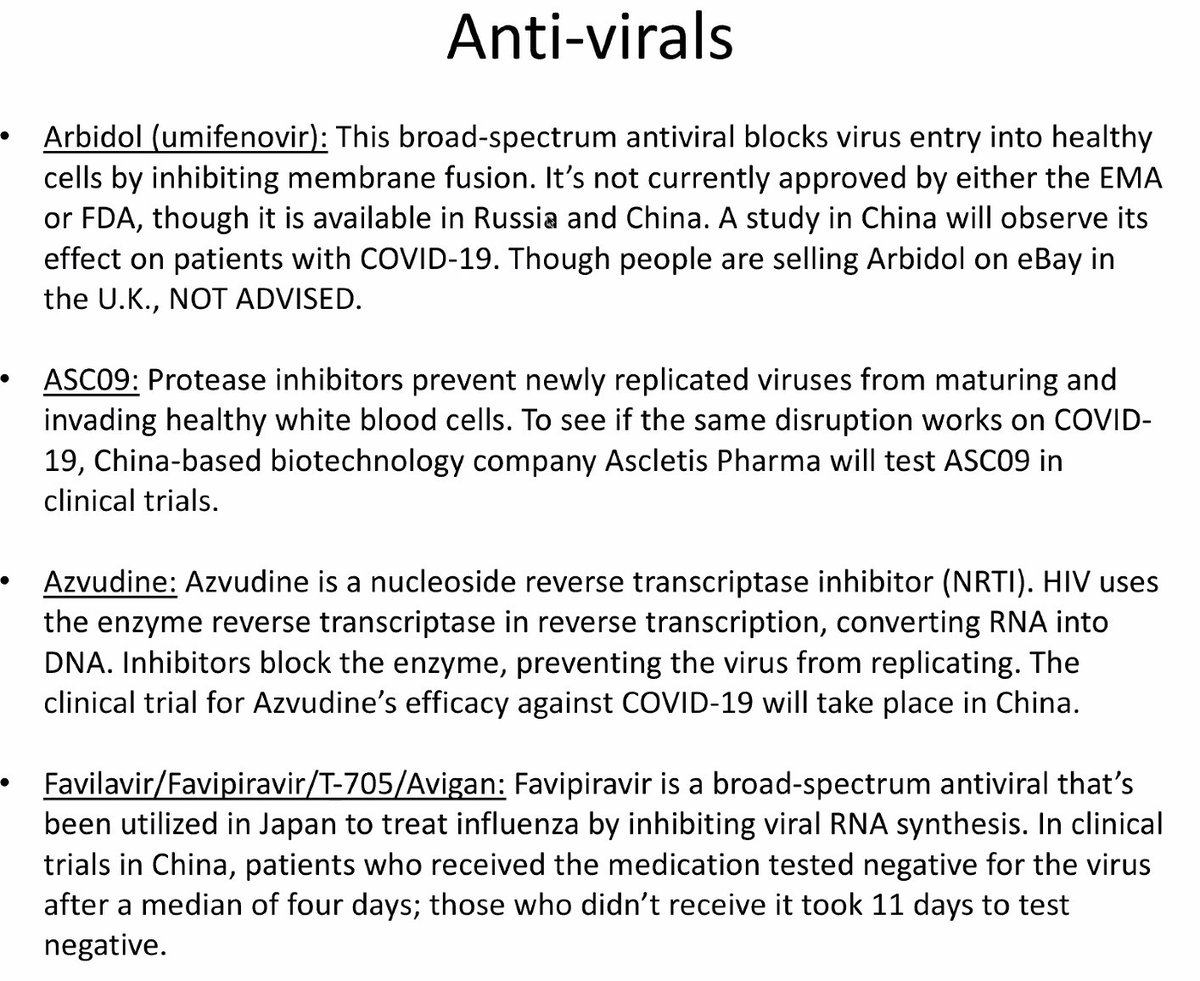
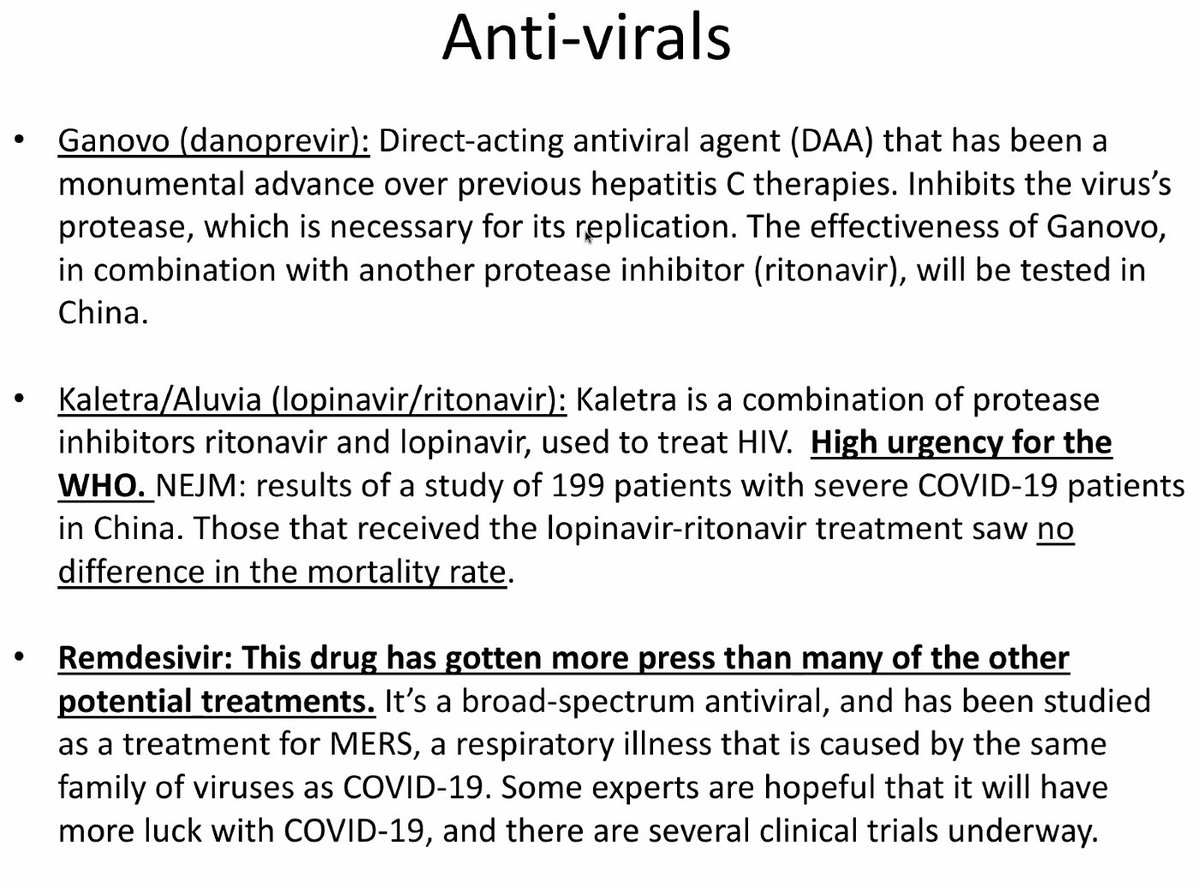
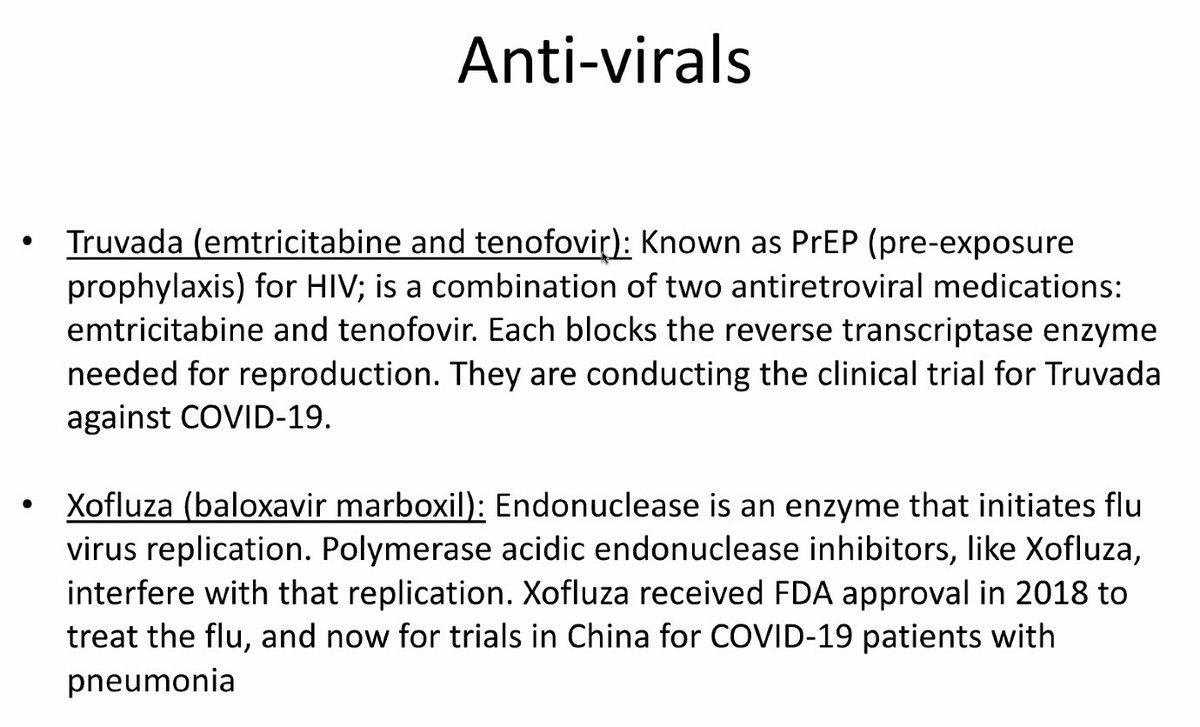
/58 Dr. @VinodThourani on #CTSNetLive #COVID19:
Antivirals coming down the pipeline as a potential therapy for #COVID19
Antivirals coming down the pipeline as a potential therapy for #COVID19
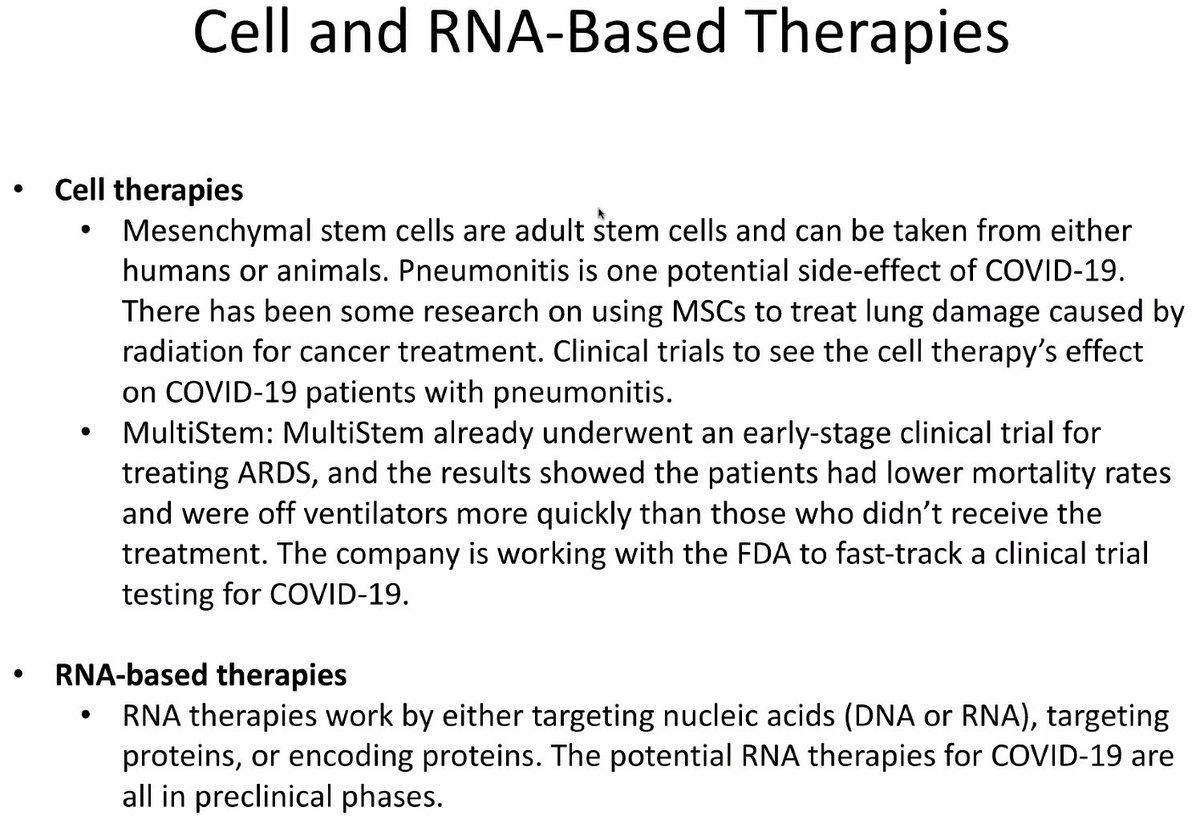
/59 Dr. @VinodThourani on #CTSNetLive #COVID19:
Cell and RNA-based therapies coming down the pipeline as a potential therapy for #COVID19
Cell and RNA-based therapies coming down the pipeline as a potential therapy for #COVID19
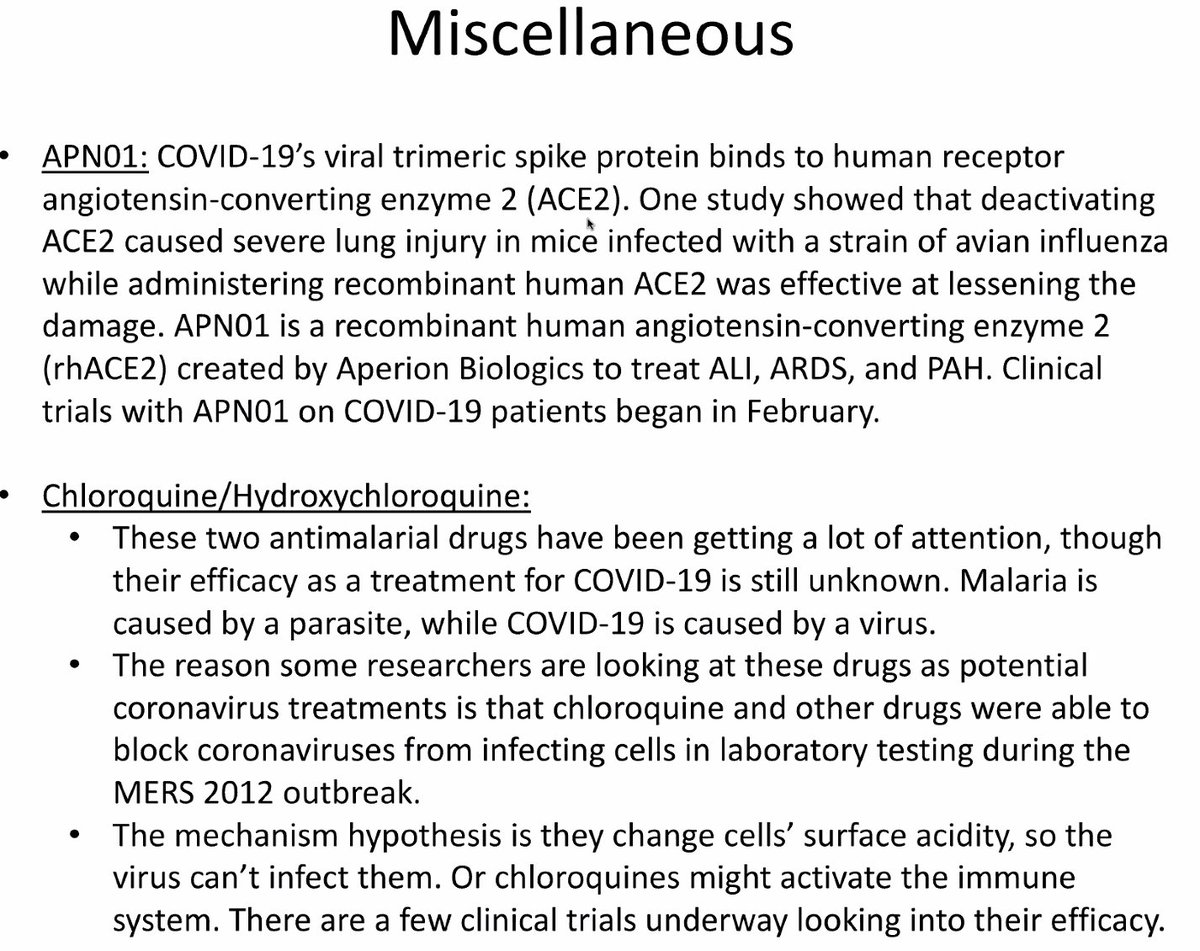
/60 Dr. @VinodThourani on #CTSNetLive #COVID19:
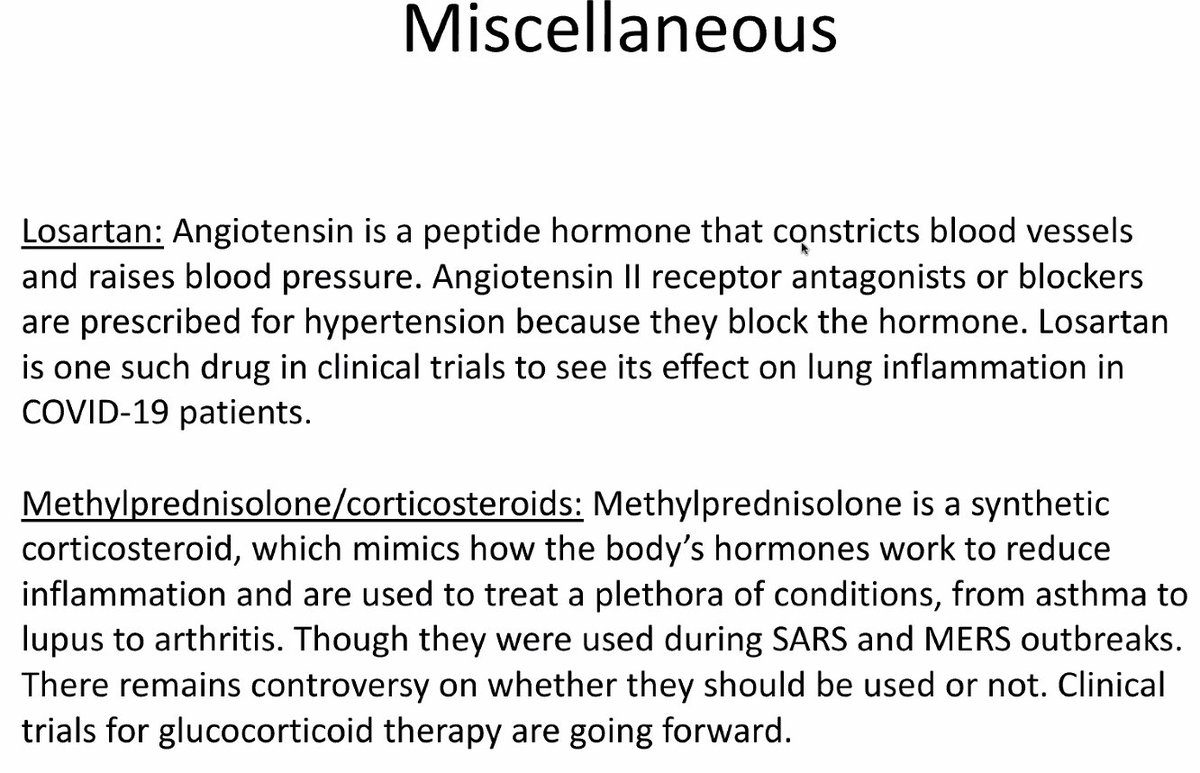
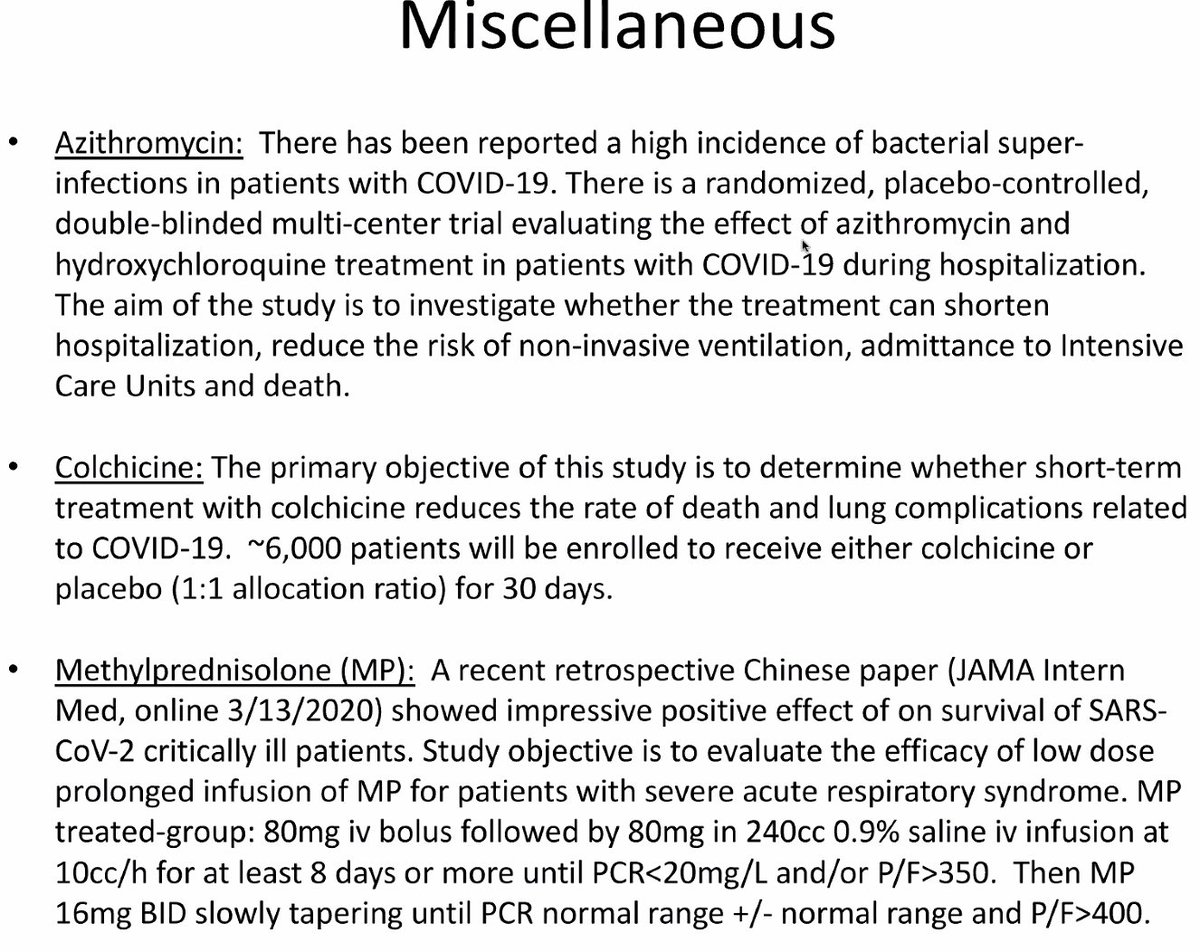
Miscellaneous therapies coming down the pipeline as a potential therapy for #COVID19
Miscellaneous therapies coming down the pipeline as a potential therapy for #COVID19
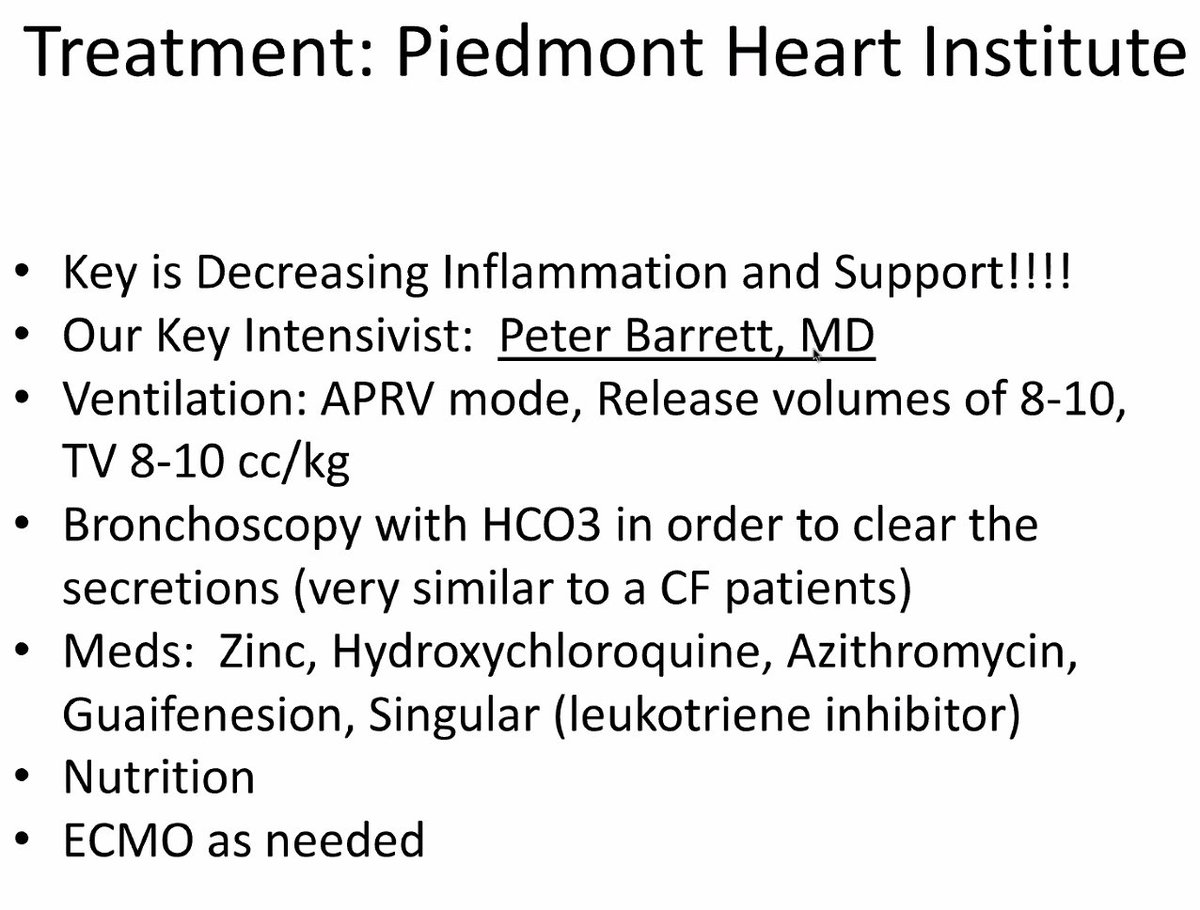
/61 Dr. @VinodThourani on #CTSNetLive #COVID19:
What they are doing at Piedmont Heart Institute
- Ventilation
- Bronchoscopy
- Zinc, hydroxychloroquine, azithromycine, singular
- Nutrition
- ECMO
What they are doing at Piedmont Heart Institute
- Ventilation
- Bronchoscopy
- Zinc, hydroxychloroquine, azithromycine, singular
- Nutrition
- ECMO
/62 Dr. @VinodThourani on #CTSNetLive #COVID19:
ECMO in
- severe reversible hypoxia / hypercarbia
- earlier than later in those without irreversible end-organ damage
- be thoughtful in utilizing this modality if ventilation is not working
ECMO in
- severe reversible hypoxia / hypercarbia
- earlier than later in those without irreversible end-organ damage
- be thoughtful in utilizing this modality if ventilation is not working
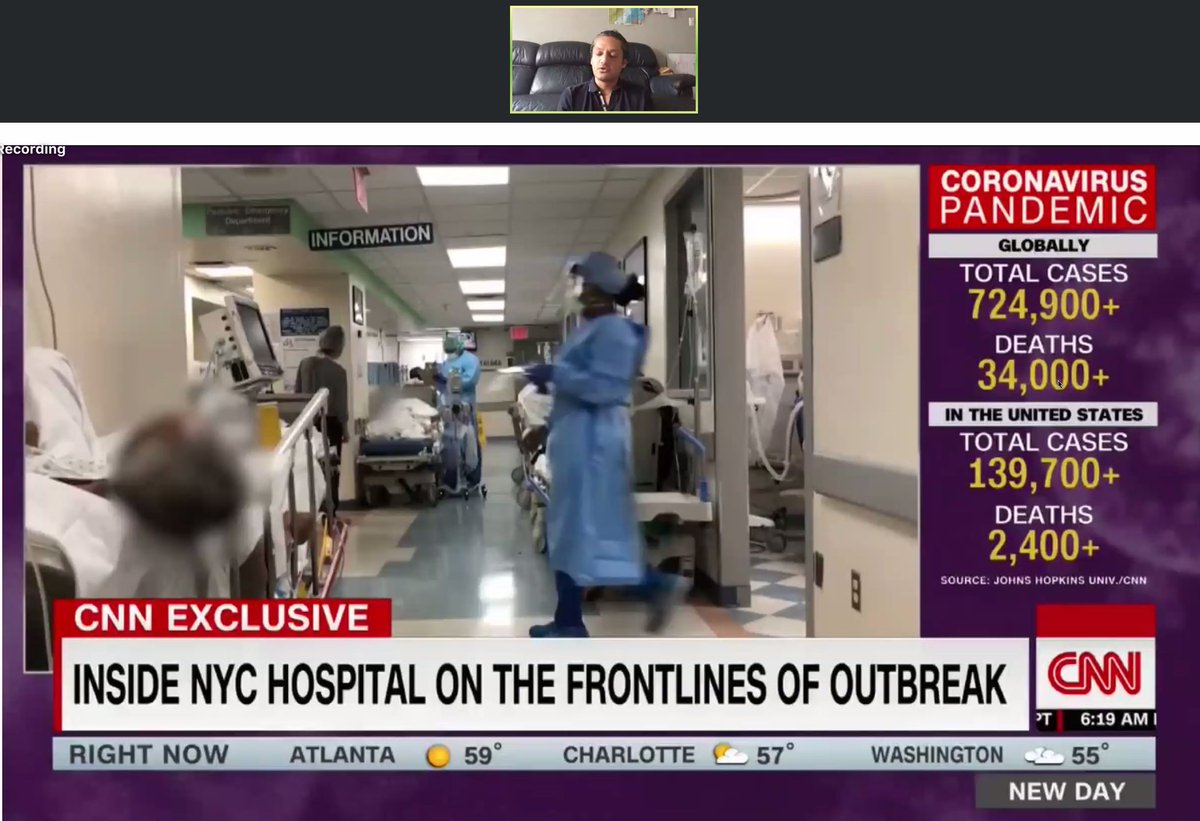
/63 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
"Ground Zero in New York: Our hospital before and during the surge. What have we learned?"
"Ground Zero in New York: Our hospital before and during the surge. What have we learned?"

/64 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
The situation in New York:
- hospital tents being set up in Central Park
- US ship to relieve hospitals - but strict criteria for pt admission
The situation in New York:
- hospital tents being set up in Central Park
- US ship to relieve hospitals - but strict criteria for pt admission
/65 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
At the start of the New York pandemic:
- COVID isolation rooms -> flooding in hallways -> reallocating other areas of hospital to become COVID designated areas -> ambulances flooding the roads
- Run out of ICUs
At the start of the New York pandemic:
- COVID isolation rooms -> flooding in hallways -> reallocating other areas of hospital to become COVID designated areas -> ambulances flooding the roads
- Run out of ICUs
/66 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
Situation now in New York:
- Nearly all hospitals on diversion
- Try to keep ER prioritized for people who need them
- People coding everywhere in stretchers - going apneic due to hypoxia
- Need to check on all pts on O2
Situation now in New York:
- Nearly all hospitals on diversion
- Try to keep ER prioritized for people who need them
- People coding everywhere in stretchers - going apneic due to hypoxia
- Need to check on all pts on O2
/67 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
- Pts (young and old) deteriorate quickly even though they may look fine initially
- Feel there is a failure in the healthcare system
- Need to protect healthcare workers
- Need a coordinated response to help prepare for surge
- Pts (young and old) deteriorate quickly even though they may look fine initially
- Feel there is a failure in the healthcare system
- Need to protect healthcare workers
- Need a coordinated response to help prepare for surge

/68 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
- Lack of #GetMePPE a huge issue, not available or being rationed
- Healthcare workers getting exposed to #COVID19 and getting sick or dying
- Lack of #GetMePPE a huge issue, not available or being rationed
- Healthcare workers getting exposed to #COVID19 and getting sick or dying
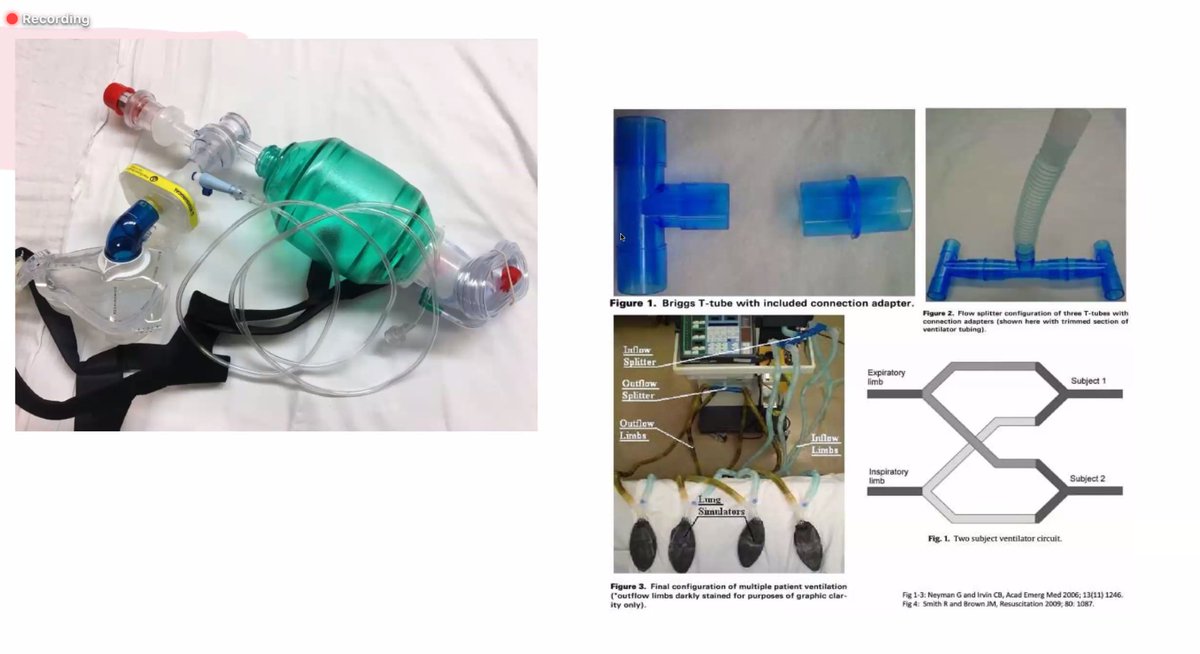
/69 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
Makeshift tools for intubation:
- CPAP mask attached to ambu bag to create tight seal and able to pre-oxygenate patients prior to intubation
- Video laryngoscopy
- Kink the tube to decrease spray
- Ventilator splitting
Makeshift tools for intubation:
- CPAP mask attached to ambu bag to create tight seal and able to pre-oxygenate patients prior to intubation
- Video laryngoscopy
- Kink the tube to decrease spray
- Ventilator splitting

/71 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
Closing thoughts -
- Take care of each other
- Look after yourself
- We will get through this together
Closing thoughts -
- Take care of each other
- Look after yourself
- We will get through this together
/72 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
Q: What PPE are you using in these environments? N95, surgical mask and mask with shield and using this for several shifts.
Q: Mgmt for pts with regular issues? Ex. STEMI -> TPA rather than cath lab etc.
Q: What PPE are you using in these environments? N95, surgical mask and mask with shield and using this for several shifts.
Q: Mgmt for pts with regular issues? Ex. STEMI -> TPA rather than cath lab etc.
/73 Dr. Chinnu Ancha on #CTSNetLive #COVID19:
Take home message
- secure your supply chain
- prepare your resources
- expand your hospitals capacity
- ensure you have 24/7 coverage for non-COVID emergencies
- outsource patient care if possible (ex. telemedicine, ambulatory)
Take home message
- secure your supply chain
- prepare your resources
- expand your hospitals capacity
- ensure you have 24/7 coverage for non-COVID emergencies
- outsource patient care if possible (ex. telemedicine, ambulatory)
/74 Thank you to moderators and panelists for such a fantastic #CTSNetLive Global #COVID19 Grand Rounds!
Stay well, be safe, look after each other. We will get through this. #tssmn
Make sure to also check out all the fantastic @ctsnetorg resources ctsnet.org/article/covid-…
Stay well, be safe, look after each other. We will get through this. #tssmn
Make sure to also check out all the fantastic @ctsnetorg resources ctsnet.org/article/covid-…
.@threadreaderapp unroll







